You might also like
- Daily Stoic Amor Fati Excerpt From The Obstacle Is The WayDocument7 pagesDaily Stoic Amor Fati Excerpt From The Obstacle Is The WaySirLouen100% (9)
- Troubleshooting Rotating Machinery: Including Centrifugal Pumps and Compressors, Reciprocating Pumps and Compressors, Fans, Steam Turbines, Electric Motors, and MoreFrom EverandTroubleshooting Rotating Machinery: Including Centrifugal Pumps and Compressors, Reciprocating Pumps and Compressors, Fans, Steam Turbines, Electric Motors, and MoreNo ratings yet
- The Ultimate Nikon SLR Handbook Vol 3Document19 pagesThe Ultimate Nikon SLR Handbook Vol 3Katie Freeman50% (4)
- Seal Reliability and Failure AnalysisDocument41 pagesSeal Reliability and Failure Analysiskarioke mohaNo ratings yet
- Apm Book PDFDocument314 pagesApm Book PDFZahid MasoodNo ratings yet
- ReliabilityDocument27 pagesReliabilityNelson LlenoNo ratings yet
- Training On Root Cause Analysis / Problem Solving TechniquesDocument66 pagesTraining On Root Cause Analysis / Problem Solving TechniquesDINESH SHARMANo ratings yet
- Uniformat IiDocument109 pagesUniformat Iiunicos100% (2)
- Evolution of Problem Solving Methods in ITDocument18 pagesEvolution of Problem Solving Methods in ITAzizah SafieNo ratings yet
- Abbreviations: For Customer Support On Your Building Construction Costs With Rsmeans Data, Call 800.448.8182Document4 pagesAbbreviations: For Customer Support On Your Building Construction Costs With Rsmeans Data, Call 800.448.8182TommyCasillas-GerenaNo ratings yet
- Abbreviations: For Customer Support On Your Building Construction Costs With Rsmeans Data, Call 800.448.8182Document4 pagesAbbreviations: For Customer Support On Your Building Construction Costs With Rsmeans Data, Call 800.448.8182TommyCasillas-GerenaNo ratings yet
- Basic Knowledge For Using Bearings SafelyDocument40 pagesBasic Knowledge For Using Bearings SafelypibearingNo ratings yet
- Reliability Analysis Applied On Centrifugal PumpsDocument9 pagesReliability Analysis Applied On Centrifugal PumpsJose Rodriguez Sanchez100% (2)
- Mechanical Seal Design, Operation and Maintenance ProblemsDocument5 pagesMechanical Seal Design, Operation and Maintenance Problemschazz29hkNo ratings yet
- Study of Failure Modes of Rolling Bearings: A ReviewDocument7 pagesStudy of Failure Modes of Rolling Bearings: A ReviewIJMERNo ratings yet
- Damage Assessment GuideDocument128 pagesDamage Assessment GuideAngel J. AliceaNo ratings yet
- Job Hazard Safety Analysis MachinesDocument39 pagesJob Hazard Safety Analysis Machinesdayglis100% (1)
- Simplified Method For Using The NFPA 70E Tables?Document43 pagesSimplified Method For Using The NFPA 70E Tables?Mohsin JamshaidNo ratings yet
- Iso22000 2005Document48 pagesIso22000 2005STELLA MARISNo ratings yet
- Failure Mode and Effect Analysis of Centrifugal PumpDocument2 pagesFailure Mode and Effect Analysis of Centrifugal PumpHAFIZMUHAMMAD SAJIDNo ratings yet
- What Is CAPA? CAPA Tools CAPA Workflow: Slide 1Document21 pagesWhat Is CAPA? CAPA Tools CAPA Workflow: Slide 1debendra naik50% (2)
- ABB Electrical Installation Handbook 2 - Electrical DevicesDocument134 pagesABB Electrical Installation Handbook 2 - Electrical Devicesanon_266748100% (2)
- FIRMAN T08072 10000 or 8000 Watt Tri Fuel Portable Generator User Manual - Manuals+Document4 pagesFIRMAN T08072 10000 or 8000 Watt Tri Fuel Portable Generator User Manual - Manuals+rperezz.agNo ratings yet
- 2019 LEED AP With Specialty Candidate HandbookDocument38 pages2019 LEED AP With Specialty Candidate HandbookLALITH KUMAR100% (1)
- Astm D4261-05 PDFDocument2 pagesAstm D4261-05 PDFdang2172014No ratings yet
- (Whitepaper) Essential Tips For Optimizing Your Preventive MaintenanceDocument11 pages(Whitepaper) Essential Tips For Optimizing Your Preventive MaintenanceNazar Alrodainy100% (1)
- Pump Troubleshooting: Problem Probable Cause SolutionDocument2 pagesPump Troubleshooting: Problem Probable Cause SolutionKarim MamdouhNo ratings yet
- Diploma in Cyber Security - Data Communication and NetworkingDocument57 pagesDiploma in Cyber Security - Data Communication and Networkingsrikant.singh62583No ratings yet
- Cause and Effect Analysis (Fishbone Diagram) : CA/PA-RCA: Basic ToolDocument23 pagesCause and Effect Analysis (Fishbone Diagram) : CA/PA-RCA: Basic ToolDipraj KayasthaNo ratings yet
- Accident Prevention Techniques: Prepared by Miss. R.M.BIST Mr. J.N.Trivedi Mr. D.B.Bhatu Mr. K.B.Gadher Mr. A.K.RAJDocument16 pagesAccident Prevention Techniques: Prepared by Miss. R.M.BIST Mr. J.N.Trivedi Mr. D.B.Bhatu Mr. K.B.Gadher Mr. A.K.RAJMr TrupenNo ratings yet
- Astm D 3276 PDFDocument62 pagesAstm D 3276 PDFJose Luis CT100% (3)
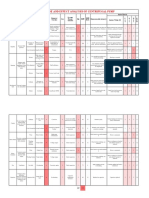
- RCA Report on Slurry Pump Seal LeakageDocument11 pagesRCA Report on Slurry Pump Seal LeakageTommyCasillas-GerenaNo ratings yet
- RCA Report on Slurry Pump Seal LeakageDocument11 pagesRCA Report on Slurry Pump Seal LeakageTommyCasillas-GerenaNo ratings yet
- Are You Doing Too Much PMDocument16 pagesAre You Doing Too Much PMFerry ArdiyantoNo ratings yet
- Ansi z10 Session 1r c2Document29 pagesAnsi z10 Session 1r c2666667No ratings yet
- Presentation Dust Suppression System Maitek EngDocument5 pagesPresentation Dust Suppression System Maitek EngGonzalo Muñoz MoreiraNo ratings yet
- Puerto Rico Building CodeDocument184 pagesPuerto Rico Building CodeJoel ArochoNo ratings yet
- NYS000179: Root Cause Analysis of 2009 CST Leak at Indian Point Unit 2Document39 pagesNYS000179: Root Cause Analysis of 2009 CST Leak at Indian Point Unit 2Aliyana ShresthaNo ratings yet
- The 2018 International Existing Building Code®: A Compilation of Wind Resistant ProvisionsDocument16 pagesThe 2018 International Existing Building Code®: A Compilation of Wind Resistant ProvisionsTommyCasillas-GerenaNo ratings yet
- 2010 IMCO CatalogDocument170 pages2010 IMCO Cataloggeav25653855No ratings yet
- Failure Reporting, Analysis, Corrective Action System: Presented By: Ricky Smith, CMRPDocument55 pagesFailure Reporting, Analysis, Corrective Action System: Presented By: Ricky Smith, CMRPTeodora DobricăNo ratings yet
- Solving Positive Displacement Pump ProblemsDocument46 pagesSolving Positive Displacement Pump ProblemsKamal UddinNo ratings yet
- SMRP Metric 5.5.38 Storeroom Maintenance Material CostDocument5 pagesSMRP Metric 5.5.38 Storeroom Maintenance Material CostJorge FracaroNo ratings yet
- Are You Doing To Much Preventive MaintenanceDocument16 pagesAre You Doing To Much Preventive Maintenancemello06No ratings yet
- RCFA and 5-Whys Tips for Successful UseDocument12 pagesRCFA and 5-Whys Tips for Successful UseadiljredsNo ratings yet
- How To Implement Maintenance Planning & SchedulingDocument18 pagesHow To Implement Maintenance Planning & SchedulingIrete FemiNo ratings yet
- Saptamsa and Navamsa Charts PDFDocument37 pagesSaptamsa and Navamsa Charts PDFjyothiNo ratings yet
- En 10305-4Document21 pagesEn 10305-4lorenzinho290100% (1)
- Mechanical Seal Troubleshooting GuideDocument38 pagesMechanical Seal Troubleshooting GuideKasih Azalia TeknindoNo ratings yet
- Trane SemiHermetic CompressorsDocument169 pagesTrane SemiHermetic CompressorsGerson RomeroNo ratings yet
- LAC - Air Oil Cooler With AC Motor For Industrial Use - HY10-6001 UKDocument12 pagesLAC - Air Oil Cooler With AC Motor For Industrial Use - HY10-6001 UKMorgan PalmaNo ratings yet
- Cleaning Public Areas EfficientlyDocument231 pagesCleaning Public Areas EfficientlyDj-Ram Vicente Vida100% (6)
- PSD SiemensDocument45 pagesPSD Siemensbrijendra2185% (13)
- Root Cause Analysis ToolsDocument15 pagesRoot Cause Analysis ToolscmlimNo ratings yet
- Non Imaging Fresnel Lenses Design and Performance of Solar ConcentartorDocument278 pagesNon Imaging Fresnel Lenses Design and Performance of Solar ConcentartorYoya LawiNo ratings yet
- Loctite Maintenance, Repair & Overhaul: Solutions Guide & Product SelectorDocument44 pagesLoctite Maintenance, Repair & Overhaul: Solutions Guide & Product SelectorGayuh W0% (1)
- Evaluating FMEA, FMECA and FMEDADocument6 pagesEvaluating FMEA, FMECA and FMEDAZakaria RadaNo ratings yet
- Centrifugal Pump Set Failure ModesDocument70 pagesCentrifugal Pump Set Failure ModesArif WidyatamaNo ratings yet
- 1 Meters For Liquids, Gases, and Solids in Suspension: Table 1: Applicability of Flow Metering TechnologiesDocument15 pages1 Meters For Liquids, Gases, and Solids in Suspension: Table 1: Applicability of Flow Metering Technologiespk_zhotNo ratings yet
- P178Document9 pagesP178keepmoshingNo ratings yet
- Measuring Bearing Currents & Shaft Voltages in Electric MotorsDocument59 pagesMeasuring Bearing Currents & Shaft Voltages in Electric Motorselectrical100% (1)
- Maintenance Presentation SlideDocument56 pagesMaintenance Presentation Slidekapun kumar nayakNo ratings yet
- Spare Part Management: Classification and Decision ModelsDocument24 pagesSpare Part Management: Classification and Decision ModelsGunawan SanjayaNo ratings yet
- Tensioner Training PresentationDocument29 pagesTensioner Training Presentationaravindan476No ratings yet
- Overall Equipment Effectiveness A Complete Guide - 2020 EditionFrom EverandOverall Equipment Effectiveness A Complete Guide - 2020 EditionNo ratings yet
- Tubular Casing Pumps by KSBDocument16 pagesTubular Casing Pumps by KSBGogy0% (1)
- Using A Conformity Matrix To Align Processes To ISO 9001 - 2015Document4 pagesUsing A Conformity Matrix To Align Processes To ISO 9001 - 2015esivaks2000No ratings yet
- Notes To File Guidance 04-20-12Document3 pagesNotes To File Guidance 04-20-12Sashwat TanayNo ratings yet
- ISCO Fusion ManualDocument96 pagesISCO Fusion ManualJoel CristobalNo ratings yet
- Case Study - Reliability at Chemical PlantDocument2 pagesCase Study - Reliability at Chemical PlantganeshdhageNo ratings yet
- Uss - Maintenance Technician MechanicalDocument11 pagesUss - Maintenance Technician Mechanicalapi-2452220920% (1)
- NASA Facilities Maintenance ProceduresDocument301 pagesNASA Facilities Maintenance ProceduresNguyễn Thanh SơnNo ratings yet
- Cre Insert PDFDocument4 pagesCre Insert PDFFirdaus TahirNo ratings yet
- Manual AMARILLO Drive Pump Repair Man 250 350 v0215Document23 pagesManual AMARILLO Drive Pump Repair Man 250 350 v0215Widi PrasetyoNo ratings yet
- FMEADocument14 pagesFMEASwati SinghNo ratings yet
- Water HeaterDocument20 pagesWater HeaterpegiNo ratings yet
- Environmental Control System A Complete Guide - 2020 EditionFrom EverandEnvironmental Control System A Complete Guide - 2020 EditionNo ratings yet
- Appendix A-Electrical Review ChecklistDocument3 pagesAppendix A-Electrical Review ChecklistTommyCasillas-GerenaNo ratings yet
- Dwayne Meadows, Ph.D. Dwayne - Meadows@noaa - GovDocument15 pagesDwayne Meadows, Ph.D. Dwayne - Meadows@noaa - GovTommyCasillas-GerenaNo ratings yet
- NSPMFRehab Specs TemplateDocument83 pagesNSPMFRehab Specs TemplateTommyCasillas-GerenaNo ratings yet
- Recent Advances in Repair and Rehabilitation of RCC Structures With Nonmetallic FibersDocument12 pagesRecent Advances in Repair and Rehabilitation of RCC Structures With Nonmetallic FibersWasim KhanNo ratings yet
- Springer Texts in Statistics: AdvisorsDocument225 pagesSpringer Texts in Statistics: AdvisorsTommyCasillas-GerenaNo ratings yet
- Reducing The Risks Nonstructural Earthquake Damage: A Practical GuideDocument139 pagesReducing The Risks Nonstructural Earthquake Damage: A Practical GuideCarlos Cardenas100% (1)
- Dwayne Meadows, Ph.D. Dwayne - Meadows@noaa - GovDocument15 pagesDwayne Meadows, Ph.D. Dwayne - Meadows@noaa - GovTommyCasillas-GerenaNo ratings yet
- Mitigation options to reduce building damageDocument26 pagesMitigation options to reduce building damageTommyCasillas-GerenaNo ratings yet
- Long-Term Performance of Epoxy-Coated Reinforcing Steel in Heavy Salt - Contaminated ConcreteDocument133 pagesLong-Term Performance of Epoxy-Coated Reinforcing Steel in Heavy Salt - Contaminated ConcreteajaymrNo ratings yet
- Wall Mounted Guide-And-Checklist-For-Cal-Schools PDFDocument56 pagesWall Mounted Guide-And-Checklist-For-Cal-Schools PDFTommyCasillas-GerenaNo ratings yet
- Residential Electrical ChecklistDocument3 pagesResidential Electrical ChecklistTommyCasillas-GerenaNo ratings yet
- Building Damage Issues in HurricanesDocument4 pagesBuilding Damage Issues in HurricanesTommyCasillas-GerenaNo ratings yet
- Puerto Rico Building Codes GuideDocument3 pagesPuerto Rico Building Codes GuideTommyCasillas-GerenaNo ratings yet
- Design, Installation, and Retrofit of Doors, Windows, and ShuttersDocument7 pagesDesign, Installation, and Retrofit of Doors, Windows, and ShuttersTommyCasillas-GerenaNo ratings yet
- Risk Category DesignationDocument2 pagesRisk Category DesignationHussamNo ratings yet
- Engineering ManagementDocument36 pagesEngineering ManagementTarek ElsafraniNo ratings yet
- Amendments to 2018 IBC Chapter 3-10 Means of EgressDocument98 pagesAmendments to 2018 IBC Chapter 3-10 Means of EgressTommyCasillas-GerenaNo ratings yet
- Resume 2024-FinalDocument1 pageResume 2024-Finalapi-716723342No ratings yet
- Se Unit 1Document77 pagesSe Unit 1sathyaaaaa1No ratings yet
- They Are Product, Price, Placement and PromotionDocument2 pagesThey Are Product, Price, Placement and PromotionVy HoàngNo ratings yet
- TSO C69bDocument28 pagesTSO C69btotololo78No ratings yet
- Analyzing Resources and CapabilitiesDocument6 pagesAnalyzing Resources and CapabilitiesImola FazakasNo ratings yet
- Living ThingsDocument12 pagesLiving ThingsangelcealoNo ratings yet
- V-Qa Full Final (PART-B) PDFDocument104 pagesV-Qa Full Final (PART-B) PDFKoushik DeyNo ratings yet
- Mobile and Wireless Communication Complete Lecture Notes #4Document20 pagesMobile and Wireless Communication Complete Lecture Notes #4Student Lecture Notes100% (1)
- Course Assignment: Language Analysis and Language Learning 681 Assignment 1Document11 pagesCourse Assignment: Language Analysis and Language Learning 681 Assignment 1Đinh Lan KhánhNo ratings yet
- HD 9 Manual 5900123 Rev F 10 1 13Document60 pagesHD 9 Manual 5900123 Rev F 10 1 13Karito NicoleNo ratings yet
- M.E. MPCDocument103 pagesM.E. MPCShobana SNo ratings yet
- Argument From IgnoranceDocument2 pagesArgument From Ignorancegio7850No ratings yet
- Salary Statement 10 01 2018Document7 pagesSalary Statement 10 01 2018lewin neritNo ratings yet
- De Bono 6 Action Shoesdoc - CompressDocument12 pagesDe Bono 6 Action Shoesdoc - CompressHazel RománNo ratings yet
- MagnetismDocument30 pagesMagnetismManiratna RoyNo ratings yet
- Dana 30 InformationDocument14 pagesDana 30 InformationBrianssrt4No ratings yet
- 35.4 Uses Principles of Effective Speech Writing Focusing On Facial Expressions, Gestures and MovementsDocument4 pages35.4 Uses Principles of Effective Speech Writing Focusing On Facial Expressions, Gestures and MovementsWayne Dolorico MillamenaNo ratings yet
- FEE 422 Practice Questions SolutionsDocument13 pagesFEE 422 Practice Questions SolutionsJoshua MNo ratings yet
- Waste Disposal Issues in Lalur VillageDocument27 pagesWaste Disposal Issues in Lalur VillageAnjana_EdathadanNo ratings yet
- Law of Insurance Eighth Semester SyllabusDocument3 pagesLaw of Insurance Eighth Semester SyllabusAastha PrakashNo ratings yet
- Data File: Äkta Explorer Ancillary EquipmentDocument4 pagesData File: Äkta Explorer Ancillary EquipmentCarlos Alberto Ramirez GarciaNo ratings yet