You might also like
- Brufen Granules Product SummaryDocument15 pagesBrufen Granules Product SummarySrechko MilichNo ratings yet
- Brufen: New Zealand Data SheetDocument12 pagesBrufen: New Zealand Data SheetFsNo ratings yet
- SE - Brufen 800 - SMPCDocument12 pagesSE - Brufen 800 - SMPCSrechko MilichNo ratings yet
- SE - Brufen 200400600 - SMPCDocument13 pagesSE - Brufen 200400600 - SMPCSrechko MilichNo ratings yet
- IBU 200 mg film coated tablet data sheetDocument15 pagesIBU 200 mg film coated tablet data sheetGpromotsNo ratings yet
- Summary of Product Characteristics: Apsifen-F Ibuprofen 600 MG Film-Coated TabletsDocument12 pagesSummary of Product Characteristics: Apsifen-F Ibuprofen 600 MG Film-Coated TabletsMeriam Gita Maulia SuhaidiNo ratings yet
- SE Brufen 2% SMPCDocument13 pagesSE Brufen 2% SMPCSrechko MilichNo ratings yet
- Ibuprofen Arrow Care TabDocument9 pagesIbuprofen Arrow Care TabshajahanputhusseriNo ratings yet
- New Zealand Data Sheet Nurofen Plus: 1. Trade Name of The Medicinal ProductDocument15 pagesNew Zealand Data Sheet Nurofen Plus: 1. Trade Name of The Medicinal ProductPhilipNo ratings yet
- Core Safety ProfileDocument7 pagesCore Safety Profileblue diamondNo ratings yet
- Ibuprofen 150mg + Paracetamol 500mg (Combodex)Document15 pagesIbuprofen 150mg + Paracetamol 500mg (Combodex)ddandan_2No ratings yet
- Ibufen 600 Caplets: Summary of Product CharacteristicsDocument13 pagesIbufen 600 Caplets: Summary of Product Characteristicsddandan_2No ratings yet
- SUMMARY OF PRODUCT CHARACTERISTICS Ibuprofen and Codeine 200mg/12.8mg Film-Coated TabletsDocument12 pagesSUMMARY OF PRODUCT CHARACTERISTICS Ibuprofen and Codeine 200mg/12.8mg Film-Coated TabletsDane WoodNo ratings yet
- IBUPROFEN (Arrowcare) : PresentationDocument6 pagesIBUPROFEN (Arrowcare) : PresentationShirmayne TangNo ratings yet
- Combiflam Tablets PI - 08072019Document13 pagesCombiflam Tablets PI - 08072019ArunNo ratings yet
- Wellbutrin Pi Approved 16may19Document15 pagesWellbutrin Pi Approved 16may19Max BernsteinNo ratings yet
- Brufen Sustained Release (SR) : Data SheetDocument11 pagesBrufen Sustained Release (SR) : Data SheetPrince Ali100% (1)
- 2021.07.30 Gen Payne PIDocument16 pages2021.07.30 Gen Payne PIZach ZwaneNo ratings yet
- Zyban DRDocument12 pagesZyban DRHardik JoshiNo ratings yet
- Otc Template Pi IbuprofenDocument3 pagesOtc Template Pi IbuprofenAnindaNo ratings yet
- SmPC Summary for Naproxen TabletsDocument13 pagesSmPC Summary for Naproxen TabletsAsif ZamanNo ratings yet
- Mefenamic Acid 50 mg5 ML Suspension - Summary of Product Characteristics (SMPC) - (Emc)Document1 pageMefenamic Acid 50 mg5 ML Suspension - Summary of Product Characteristics (SMPC) - (Emc)Gina UtamaNo ratings yet
- New Zealand Data Sheet for Ponstan CapsulesDocument13 pagesNew Zealand Data Sheet for Ponstan CapsulesHeng Hiang SengNo ratings yet
- Brufen Film-Coated Tablet ENG PL - 09001be68023cd70Document8 pagesBrufen Film-Coated Tablet ENG PL - 09001be68023cd70Esha RiazNo ratings yet
- Fenofibrate 200 MG Capsules - Summary of Product Characteristics (SMPC) - Print Friendly - (Emc)Document7 pagesFenofibrate 200 MG Capsules - Summary of Product Characteristics (SMPC) - Print Friendly - (Emc)bhavaniNo ratings yet
- Feldene Melt 20mg Tablets - Summary of Product Characteristics (SMPC) - Print Friendly - (Emc)Document10 pagesFeldene Melt 20mg Tablets - Summary of Product Characteristics (SMPC) - Print Friendly - (Emc)Maria BibiNo ratings yet
- Fenofibrate 200 MG Capsules: 1. Name of The Medicinal Product 2. Qualitative and Quantitative CompositionDocument8 pagesFenofibrate 200 MG Capsules: 1. Name of The Medicinal Product 2. Qualitative and Quantitative CompositionbhavaniNo ratings yet
- SE - Brufen 800 - PILDocument8 pagesSE - Brufen 800 - PILSrechko MilichNo ratings yet
- Etopan XL Physician Leaflet for Osteoarthritis and Rheumatoid ArthritisDocument9 pagesEtopan XL Physician Leaflet for Osteoarthritis and Rheumatoid Arthritisddandan_2No ratings yet
- Pantozol Control Epar Product Information - enDocument30 pagesPantozol Control Epar Product Information - enDeKa NineNo ratings yet
- Anx 130215 enDocument143 pagesAnx 130215 enzekyashawnNo ratings yet
- Ambroxol Hydrochloride, Terbutaline Sulphate and GuaiphenesinDocument7 pagesAmbroxol Hydrochloride, Terbutaline Sulphate and Guaiphenesinanup jhaNo ratings yet
- Aceclofenac 100 MG Film-Coated Tablets - Summary of Product Characteristics (SMPC) - Print Friendly - (eMC) PDFDocument9 pagesAceclofenac 100 MG Film-Coated Tablets - Summary of Product Characteristics (SMPC) - Print Friendly - (eMC) PDFHabibNo ratings yet
- Vortioxetine LeafletDocument21 pagesVortioxetine LeafletAnchit RathiNo ratings yet
- Name of The Medicinal Product: Short-Term TreatmentDocument10 pagesName of The Medicinal Product: Short-Term TreatmentasdwasdNo ratings yet
- Lipanthyl Penta PIDocument9 pagesLipanthyl Penta PIPhan Do Dang KhoaNo ratings yet
- SE - Brufen 200400600 - PILDocument9 pagesSE - Brufen 200400600 - PILSrechko MilichNo ratings yet
- Prescribing Info for Dostinex TabletsDocument9 pagesPrescribing Info for Dostinex TabletsasdwasdNo ratings yet
- Cadex Tablets and Caplets Product SummaryDocument9 pagesCadex Tablets and Caplets Product SummaryasdwasdNo ratings yet
- IbuprofenDocument3 pagesIbuprofenAnupama NagrajNo ratings yet
- BUTRANS-buprenorphine Patch, Extended Release Purdue Pharma LPDocument64 pagesBUTRANS-buprenorphine Patch, Extended Release Purdue Pharma LPmeiraimNo ratings yet
- Voltfast-Sep 2022.SIN-app260123 PDFDocument14 pagesVoltfast-Sep 2022.SIN-app260123 PDFChelang AbdulkareemNo ratings yet
- Florinef SPCDocument7 pagesFlorinef SPCJohn GoulianosNo ratings yet
- Ultibro Breezhaler Epar Product Information enDocument50 pagesUltibro Breezhaler Epar Product Information enMuqaj MuniraNo ratings yet
- Controloc 40: Prescribing InformationDocument10 pagesControloc 40: Prescribing InformationNavieen RajNo ratings yet
- Supralip 160 MG Film-Coated Tablets - Summary of Product Characteristics (SMPC) - Print Friendly - (Emc)Document8 pagesSupralip 160 MG Film-Coated Tablets - Summary of Product Characteristics (SMPC) - Print Friendly - (Emc)bhavaniNo ratings yet
- SE - Brufen 2% - PILDocument9 pagesSE - Brufen 2% - PILSrechko MilichNo ratings yet
- Riltrava Aerosphere Epar Product Information enDocument42 pagesRiltrava Aerosphere Epar Product Information enshihyanghuangNo ratings yet
- Pi Ibugesic Fever and PainDocument20 pagesPi Ibugesic Fever and PainAndrew PartridgeNo ratings yet
- Brintellix Epar Product Information - En@&56)Document104 pagesBrintellix Epar Product Information - En@&56)FsNo ratings yet
- Oxybutynin Hydrochloride Tablets 5 MG - Summary of Product Characteristics (SMPC) - Print Friendly - (Emc)Document7 pagesOxybutynin Hydrochloride Tablets 5 MG - Summary of Product Characteristics (SMPC) - Print Friendly - (Emc)surafelNo ratings yet
- Fenofibrate 267mg Capsules - Summary of Product Characteristics (SMPC) - Print Friendly - (Emc)Document8 pagesFenofibrate 267mg Capsules - Summary of Product Characteristics (SMPC) - Print Friendly - (Emc)bhavaniNo ratings yet
- Alendronate SodiumDocument16 pagesAlendronate SodiumasdwasdNo ratings yet
- MEFTAL P Suspension PIDocument10 pagesMEFTAL P Suspension PIpiyush patelNo ratings yet
- Fenofibrate 160mg Tablets - Summary of Product Characteristics (SMPC) - Print Friendly - (Emc)Document6 pagesFenofibrate 160mg Tablets - Summary of Product Characteristics (SMPC) - Print Friendly - (Emc)bhavaniNo ratings yet
- Pharma Cards.Document19 pagesPharma Cards.Brent NicholsNo ratings yet
- Allopurinol tablets summary of product characteristicsDocument12 pagesAllopurinol tablets summary of product characteristicsasdwasdNo ratings yet
- Generic Name: Albuterol Brand Name: Salbutamol, Proventil, Ventolin, Accuneb, Airet, Novo-SalbutamolDocument26 pagesGeneric Name: Albuterol Brand Name: Salbutamol, Proventil, Ventolin, Accuneb, Airet, Novo-SalbutamolAnna Joy Antone100% (1)
- Methods of Extracting Volatile OilsDocument18 pagesMethods of Extracting Volatile Oilsdilka dariyaNo ratings yet
- Resins and Oleo Resins Introduction: Hafiz Waheed UllahDocument10 pagesResins and Oleo Resins Introduction: Hafiz Waheed Ullahdilka dariyaNo ratings yet
- Cosmecuticals: Hafiz Waheed UllahDocument22 pagesCosmecuticals: Hafiz Waheed Ullahdilka dariyaNo ratings yet
- Wa0018Document12 pagesWa0018dilka dariyaNo ratings yet
- Phenolic Ether, Oxide Volatile Oils, Ester Volatile Oil: Hafiz Waheed UllahDocument27 pagesPhenolic Ether, Oxide Volatile Oils, Ester Volatile Oil: Hafiz Waheed Ullahdilka dariyaNo ratings yet
- Alcoholic Volatile Oils: Hafiz Waheed UllahDocument21 pagesAlcoholic Volatile Oils: Hafiz Waheed Ullahdilka dariya100% (1)
- Bioavailability - and - Bioequivalence - 2 PDFDocument18 pagesBioavailability - and - Bioequivalence - 2 PDFdilka dariyaNo ratings yet
- Clinical Pharmacokinetics Sample ChapterDocument44 pagesClinical Pharmacokinetics Sample Chapterpinkbutter100% (1)
- Ipomoea and Myrrh: Hafiz Waheed UllahDocument17 pagesIpomoea and Myrrh: Hafiz Waheed Ullahdilka dariyaNo ratings yet
- Advanced Excel 2010 2 - Formulas - 0Document4 pagesAdvanced Excel 2010 2 - Formulas - 0SunnyNo ratings yet
- Wm231 PP Manajemen KualitasDocument10 pagesWm231 PP Manajemen KualitasTengku Aditya MaulanaNo ratings yet
- Quality Control Book PDFDocument46 pagesQuality Control Book PDFSheikNo ratings yet
- Aims: Pharmaceutical Technology Teaches The DifferentDocument22 pagesAims: Pharmaceutical Technology Teaches The Differentdilka dariyaNo ratings yet
- Abbreviations Commonly Used in Obstetrics and Gynecology Physical ExaminationDocument2 pagesAbbreviations Commonly Used in Obstetrics and Gynecology Physical ExaminationwenwenwencheatNo ratings yet
- 10 4 5 Tablet-FriabilityDocument1 page10 4 5 Tablet-Friabilityarfa aliNo ratings yet
- CamScanner Scans - Multiple PagesDocument13 pagesCamScanner Scans - Multiple Pagesdilka dariyaNo ratings yet
- Nonlinear pharmacokinetics explainedDocument18 pagesNonlinear pharmacokinetics explainedSyed UmairNo ratings yet
- Compartmental Modeling in The Analysis of Biological SystemsDocument49 pagesCompartmental Modeling in The Analysis of Biological Systemsdilka dariyaNo ratings yet
- Faculity of Pharmacy Hajvery University, Euro Campus .LahoreDocument17 pagesFaculity of Pharmacy Hajvery University, Euro Campus .Lahoredilka dariyaNo ratings yet
- Clinical Notes-2Document67 pagesClinical Notes-2dilka dariyaNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument21 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsUnnati GargNo ratings yet
- Multiple CamScanner Scans in One DocumentDocument18 pagesMultiple CamScanner Scans in One Documentdilka dariyaNo ratings yet
- Assignment Title: Submitted To: Submitted byDocument18 pagesAssignment Title: Submitted To: Submitted bySyed UmairNo ratings yet
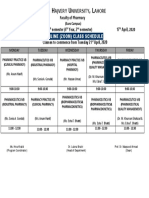
- T H U, L: Online (Zoom) Class ScheduleDocument1 pageT H U, L: Online (Zoom) Class Scheduledilka dariyaNo ratings yet
- Volatile Oils: Hafiz Waheed UllahDocument23 pagesVolatile Oils: Hafiz Waheed Ullahdilka dariyaNo ratings yet
- Publication 11 16756 6264 PDFDocument8 pagesPublication 11 16756 6264 PDFVikram VermaNo ratings yet
- Bioavailability Studies. Chap 3-2Document40 pagesBioavailability Studies. Chap 3-2dilka dariyaNo ratings yet
- T H U, L: Online (Zoom) Class ScheduleDocument1 pageT H U, L: Online (Zoom) Class Scheduledilka dariyaNo ratings yet
- Chemotherapy 1Document37 pagesChemotherapy 1dilka dariyaNo ratings yet
- Imigcs ManualDocument24 pagesImigcs ManualPrinceNo ratings yet
- Causes of Upper Gastrointestinal Bleeding in Adults UpToDateDocument37 pagesCauses of Upper Gastrointestinal Bleeding in Adults UpToDateJodene Rose RojasNo ratings yet
- Thesis Topics of MS General SurgeryDocument20 pagesThesis Topics of MS General SurgeryNaveed Khan75% (12)
- IMEDICS AKT Errors FINALDocument24 pagesIMEDICS AKT Errors FINALUmer AnwarNo ratings yet
- Gastric AnalysisDocument4 pagesGastric AnalysisMae DoinogNo ratings yet
- CME UGIB, Hypovolemic Shock 31.12.21 - FINALDocument58 pagesCME UGIB, Hypovolemic Shock 31.12.21 - FINALThayalan RaviNo ratings yet
- Omeprazole Drug StudyDocument3 pagesOmeprazole Drug StudySophia Loraine Dorone Jesura100% (1)
- Understanding Peptic Ulcer DiseaseDocument21 pagesUnderstanding Peptic Ulcer DiseaseTeresaSM19No ratings yet
- This Study Resource Was: Case 1: Hay Fever & ColdsDocument4 pagesThis Study Resource Was: Case 1: Hay Fever & ColdsMary Jennel RosNo ratings yet
- Why Do We Fall OBJ Class 9Document6 pagesWhy Do We Fall OBJ Class 9naman mahawerNo ratings yet
- ReemDocument13 pagesReemSAYED ZAKINo ratings yet
- Chootip 2017 Efficacy and Safety of "Yahom" As A Traditional Thai Herbal Therapy - A Systematic ReviewDocument14 pagesChootip 2017 Efficacy and Safety of "Yahom" As A Traditional Thai Herbal Therapy - A Systematic ReviewAkarat SivaphongthongchaiNo ratings yet
- Git GutDocument4 pagesGit GutAngelica Murillo Ang-AngcoNo ratings yet
- Protonix (Pantoprazole)Document1 pageProtonix (Pantoprazole)ENo ratings yet
- StomachDocument204 pagesStomachrajmv7No ratings yet
- GUIDELINES Final Year by Ali RazaDocument115 pagesGUIDELINES Final Year by Ali Raza5mxhkvcgtzNo ratings yet
- Mao Na Gyud NiDocument85 pagesMao Na Gyud NiJoanne Bernadette AguilarNo ratings yet
- Drugs acting on digestive systemDocument10 pagesDrugs acting on digestive systemRumana ShaikhNo ratings yet
- Upper Gastrointestinal TractDocument3 pagesUpper Gastrointestinal Tractmuhammad ied risandiNo ratings yet
- Rekap DataDocument48 pagesRekap Dataikhsan syakban a.sNo ratings yet
- Treating Peptic Ulcers with DrugsDocument35 pagesTreating Peptic Ulcers with DrugsPridho GaziansyahNo ratings yet
- ACVIM Consensus Statement Support For Rational Administration of Gastrointestinal Protectants To Dogs and CatsDocument19 pagesACVIM Consensus Statement Support For Rational Administration of Gastrointestinal Protectants To Dogs and Catsnenows_504807146No ratings yet
- General Surgery II Exam PaperDocument2 pagesGeneral Surgery II Exam PaperSheikh Muhammad TabieshNo ratings yet
- WHO List of Conditions Treated by Acupuncture - Healthy Family AcupunctureDocument3 pagesWHO List of Conditions Treated by Acupuncture - Healthy Family AcupunctureSreekanth KrishnamurthyNo ratings yet
- 13 Antacids and Controllers UpdDocument63 pages13 Antacids and Controllers Updone_nd_onlyuNo ratings yet
- Ethiopian National Drug FormularyDocument572 pagesEthiopian National Drug FormularyportosinNo ratings yet
- Epidemiology Approach To Association and CausationDocument52 pagesEpidemiology Approach To Association and Causationm@chie77No ratings yet
- Helicobacter PyloriDocument33 pagesHelicobacter Pyloritummalapalli venkateswara rao100% (6)
- Perforated Peptic Ulcer DiseaseDocument9 pagesPerforated Peptic Ulcer DiseaseMade Oka HeryanaNo ratings yet
- I Have Stomach Trouble A Lot of Paint and Nause. I Thing I Have Gastritis, But I Amtold There Are Several Kinds. Is It So?Document7 pagesI Have Stomach Trouble A Lot of Paint and Nause. I Thing I Have Gastritis, But I Amtold There Are Several Kinds. Is It So?amandaNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- How to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipFrom EverandHow to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipRating: 4.5 out of 5 stars4.5/5 (1135)
- Breaking the Habit of Being YourselfFrom EverandBreaking the Habit of Being YourselfRating: 4.5 out of 5 stars4.5/5 (1456)
- Briefly Perfectly Human: Making an Authentic Life by Getting Real About the EndFrom EverandBriefly Perfectly Human: Making an Authentic Life by Getting Real About the EndNo ratings yet
- Unstoppable You: A Teen Girl's Handbook for Joyful LivingFrom EverandUnstoppable You: A Teen Girl's Handbook for Joyful LivingRating: 4.5 out of 5 stars4.5/5 (21)
- How to Walk into a Room: The Art of Knowing When to Stay and When to Walk AwayFrom EverandHow to Walk into a Room: The Art of Knowing When to Stay and When to Walk AwayRating: 4.5 out of 5 stars4.5/5 (5)
- Neville Goddard Master Course to Manifest Your Desires Into Reality Using The Law of Attraction: Learn the Secret to Overcoming Your Current Problems and Limitations, Attaining Your Goals, and Achieving Health, Wealth, Happiness and Success!From EverandNeville Goddard Master Course to Manifest Your Desires Into Reality Using The Law of Attraction: Learn the Secret to Overcoming Your Current Problems and Limitations, Attaining Your Goals, and Achieving Health, Wealth, Happiness and Success!Rating: 5 out of 5 stars5/5 (284)
- The Bridesmaid: The addictive psychological thriller that everyone is talking aboutFrom EverandThe Bridesmaid: The addictive psychological thriller that everyone is talking aboutRating: 4 out of 5 stars4/5 (130)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Tech Detox for Teens: Finding Balance in a Digital WorldFrom EverandTech Detox for Teens: Finding Balance in a Digital WorldRating: 4.5 out of 5 stars4.5/5 (26)
- Chakras and Yoga: Finding Inner Harmony Through Practice, Awaken the Energy Centers for Optimal Physical and Spiritual Health.From EverandChakras and Yoga: Finding Inner Harmony Through Practice, Awaken the Energy Centers for Optimal Physical and Spiritual Health.Rating: 4 out of 5 stars4/5 (2)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Natural Memory Improvement TechniquesFrom EverandNatural Memory Improvement TechniquesRating: 4.5 out of 5 stars4.5/5 (54)
- Breaking Barriers, Building Strength: A Teen's Journey to Fearless LivingFrom EverandBreaking Barriers, Building Strength: A Teen's Journey to Fearless LivingRating: 4.5 out of 5 stars4.5/5 (25)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The House Mate: A gripping psychological thriller you won't be able to put downFrom EverandThe House Mate: A gripping psychological thriller you won't be able to put downRating: 4 out of 5 stars4/5 (126)
- Prisoners of Geography: Ten Maps That Explain Everything About the WorldFrom EverandPrisoners of Geography: Ten Maps That Explain Everything About the WorldRating: 4.5 out of 5 stars4.5/5 (1145)
- No Mud, No Lotus: The Art of Transforming SufferingFrom EverandNo Mud, No Lotus: The Art of Transforming SufferingRating: 5 out of 5 stars5/5 (173)
- The Waitress: The gripping, edge-of-your-seat psychological thriller from the bestselling author of The BridesmaidFrom EverandThe Waitress: The gripping, edge-of-your-seat psychological thriller from the bestselling author of The BridesmaidRating: 4 out of 5 stars4/5 (65)
- Deep Sleep Hypnosis: Guided Meditation For Sleep & HealingFrom EverandDeep Sleep Hypnosis: Guided Meditation For Sleep & HealingRating: 4.5 out of 5 stars4.5/5 (103)
- Summary: I'm Glad My Mom Died: by Jennette McCurdy: Key Takeaways, Summary & AnalysisFrom EverandSummary: I'm Glad My Mom Died: by Jennette McCurdy: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (2)
- For Women Only, Revised and Updated Edition: What You Need to Know About the Inner Lives of MenFrom EverandFor Women Only, Revised and Updated Edition: What You Need to Know About the Inner Lives of MenRating: 4.5 out of 5 stars4.5/5 (267)