You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Filter Integrity Test MachineDocument4 pagesFilter Integrity Test MachineAtul SharmaNo ratings yet
- Adime Malnutrition and OncolgyDocument6 pagesAdime Malnutrition and Oncolgyapi-300587226100% (1)
- HE - Food and Beverages CGDocument14 pagesHE - Food and Beverages CGJohn Leonard88% (8)
- Muscle Protein Turnover in Endurance Training - A ReviewDocument7 pagesMuscle Protein Turnover in Endurance Training - A ReviewAna Souza LimaNo ratings yet
- The Size PrincipleDocument3 pagesThe Size PrincipleAna Souza LimaNo ratings yet
- Os Efeitos Modulatorios Do Treinamento Com Exercicios Sobre As Disfuncoes Imunometabolicas Induzidas Pela ObesidadeDocument26 pagesOs Efeitos Modulatorios Do Treinamento Com Exercicios Sobre As Disfuncoes Imunometabolicas Induzidas Pela ObesidadeAna Souza LimaNo ratings yet
- Force, Work, Power, and Exercise.17Document2 pagesForce, Work, Power, and Exercise.17Ana Souza LimaNo ratings yet
- Force, Work, and Power in Athletic TrainingDocument13 pagesForce, Work, and Power in Athletic TrainingAna Souza LimaNo ratings yet
- A Relacao Da Gordura Visceral Com Hipertensao ArterialDocument14 pagesA Relacao Da Gordura Visceral Com Hipertensao ArterialAna Souza LimaNo ratings yet
- Larsson1979 - Muscle Strength and Speed of Movement in Relation To Age and Muscle Morphology PDFDocument6 pagesLarsson1979 - Muscle Strength and Speed of Movement in Relation To Age and Muscle Morphology PDFAna Souza LimaNo ratings yet
- Knee Biomechanics of The Dynamic PDFDocument15 pagesKnee Biomechanics of The Dynamic PDFRishabh KumarNo ratings yet
- Obesidade Sarcopênica e Sua Associação Com Doença RespiratóriaDocument6 pagesObesidade Sarcopênica e Sua Associação Com Doença RespiratóriaAna Souza LimaNo ratings yet
- Hunter2004 - eFFECTS OF RESISTANCE TRAINING ON OLDER ADULTSDocument20 pagesHunter2004 - eFFECTS OF RESISTANCE TRAINING ON OLDER ADULTSAna Souza LimaNo ratings yet
- Dose Response To RT in OlderDocument28 pagesDose Response To RT in OlderstarmittNo ratings yet
- Kraemer & Ratames - Treinamento Resistido - 2004Document15 pagesKraemer & Ratames - Treinamento Resistido - 2004pedromattarnogueira7734100% (2)
- Accepted Manuscript: Corresponding AuthorDocument38 pagesAccepted Manuscript: Corresponding AuthorAna Souza LimaNo ratings yet
- HG1Document9 pagesHG1jose carrasquillaNo ratings yet
- Histochemical Characteristics of Humna Skeletal Muscle During AgingDocument3 pagesHistochemical Characteristics of Humna Skeletal Muscle During AgingAna Souza LimaNo ratings yet
- Strengthtraining JAP 1988 PDFDocument7 pagesStrengthtraining JAP 1988 PDFEl BarbudoNo ratings yet
- IMAMURA1983 - Human Major Psoas Muscle and Sarcrospinalis Muscle in Relation To Age - A Study by Computed TomographyDocument4 pagesIMAMURA1983 - Human Major Psoas Muscle and Sarcrospinalis Muscle in Relation To Age - A Study by Computed TomographyAna Souza LimaNo ratings yet
- Muscle Tendon Interaction and Elastic Usage in Human WalkingDocument6 pagesMuscle Tendon Interaction and Elastic Usage in Human WalkingAna Souza LimaNo ratings yet
- As Respostas Bioquímicas e Neuromusculares Agudas Justificam A Classificação Do Exercício Resistido Do Tipo Força e hipertrofiaINGLES2014Document29 pagesAs Respostas Bioquímicas e Neuromusculares Agudas Justificam A Classificação Do Exercício Resistido Do Tipo Força e hipertrofiaINGLES2014Ana Souza LimaNo ratings yet
- Efeitos Da Potencializacao Pos Ativacao em AtletasDocument11 pagesEfeitos Da Potencializacao Pos Ativacao em AtletasAna Souza LimaNo ratings yet
- Deadlift Muscle Force and Activation Under Stable and Unstable Conditions - Força Muscular e Ativação Do Deadlift em Condições Estáveis e InstáveisDocument8 pagesDeadlift Muscle Force and Activation Under Stable and Unstable Conditions - Força Muscular e Ativação Do Deadlift em Condições Estáveis e InstáveisAna Souza LimaNo ratings yet
- Clark2008 Sacopenia DinapeniaDocument6 pagesClark2008 Sacopenia DinapeniaAna Souza LimaNo ratings yet
- Dose Response To RT in OlderDocument28 pagesDose Response To RT in OlderstarmittNo ratings yet
- Ijpcr 22 309Document6 pagesIjpcr 22 309Sriram NagarajanNo ratings yet
- August 2016Document15 pagesAugust 2016Pumper Trader0% (1)
- Alpha Full CaseDocument5 pagesAlpha Full CaseAnonymous 4IOzjRIB1No ratings yet
- Directorate of Education, GNCT of Delhi: Term-II (Session 2021-22)Document4 pagesDirectorate of Education, GNCT of Delhi: Term-II (Session 2021-22)Anjli KulshresthaNo ratings yet
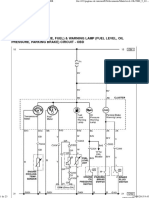
- Dokumen - Tips Daewoo Service Manual Instrument Cluster Matiz-2023Document23 pagesDokumen - Tips Daewoo Service Manual Instrument Cluster Matiz-2023urexalg AlgériaNo ratings yet
- Applications of Proton Exchange Membrane Fuel CellDocument20 pagesApplications of Proton Exchange Membrane Fuel CellRiri SasyNo ratings yet
- Año del Fortalecimiento de la Soberanía NacionalDocument4 pagesAño del Fortalecimiento de la Soberanía NacionalRYAN 28SKNo ratings yet
- Banking Question PapersDocument12 pagesBanking Question Papersmohak khinNo ratings yet
- BG 370 Operation & Maintenance ManualDocument32 pagesBG 370 Operation & Maintenance ManualRamasubramanian SankaranarayananNo ratings yet
- BurgerKing Versus McDonaldsDocument4 pagesBurgerKing Versus McDonaldsmarkus johannessenNo ratings yet
- Bengal PresentationDocument37 pagesBengal PresentationManish KumarNo ratings yet
- 1 Design Engineering Drawings For The EasyDry M500 JD Version PDFDocument169 pages1 Design Engineering Drawings For The EasyDry M500 JD Version PDFSelim Lukman100% (1)
- Service Manual: Side by Side S20B RSB21-A/GDocument16 pagesService Manual: Side by Side S20B RSB21-A/GjicutuNo ratings yet
- Questionnaire - Yash PareekDocument4 pagesQuestionnaire - Yash PareekYash PareekNo ratings yet
- If You Have Guts Then Dare To Be DIFFERENTDocument20 pagesIf You Have Guts Then Dare To Be DIFFERENTChirag Saiya (PHILOSOPHER) - SPIRITUAL Speaker and Writer100% (1)
- KOLHAN UNIVERSITY B.Sc Zoology Semester I Exam 2021 Provisional Marks CardDocument2 pagesKOLHAN UNIVERSITY B.Sc Zoology Semester I Exam 2021 Provisional Marks CardSmritiNo ratings yet
- A Review of Bempedoic Acid - A New Drug For Old ProblemDocument6 pagesA Review of Bempedoic Acid - A New Drug For Old ProblemVõ Ngọc Bích VânNo ratings yet
- PFC Katalog PPDocument128 pagesPFC Katalog PPbmsinghNo ratings yet
- 13th Month Pay Law and JurisprudenceDocument2 pages13th Month Pay Law and JurisprudenceJennylyn Biltz AlbanoNo ratings yet
- July 28Document8 pagesJuly 28thestudentageNo ratings yet
- St. Luke's Echocardiogram Patient GuideDocument2 pagesSt. Luke's Echocardiogram Patient Guideteju13aNo ratings yet
- Effects of Restorative Materials On Dental PulpDocument32 pagesEffects of Restorative Materials On Dental PulpUpasana BhandariNo ratings yet
- Report For Missing Sealing PlateDocument9 pagesReport For Missing Sealing PlateFazalmin shahNo ratings yet
- Solid Phase ExtractionDocument16 pagesSolid Phase ExtractionDAVID VELEZNo ratings yet
- بﻮﺤﻟا ﻦﺤﻃ ﺔﻧﺎﻘﺗ - Cereal Milling Technology: · January 2013Document202 pagesبﻮﺤﻟا ﻦﺤﻃ ﺔﻧﺎﻘﺗ - Cereal Milling Technology: · January 2013Moh Al Basher BabikerNo ratings yet
- 05 Building Laws Summary 11-03-21Document27 pages05 Building Laws Summary 11-03-21Lyka Mendoza MojaresNo ratings yet
- G8 - Element - Metal ReactionDocument29 pagesG8 - Element - Metal ReactionListya RahmawatiNo ratings yet