You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Top 10 Most Powerful Openings in Chess PDFDocument12 pagesTop 10 Most Powerful Openings in Chess PDFsyaf file gwNo ratings yet
- Constantin Floros, Kenneth Chalmers - New Ears For New Music-Peter Lang GMBH, Internationaler Verlag Der Wissenschaften (2014)Document242 pagesConstantin Floros, Kenneth Chalmers - New Ears For New Music-Peter Lang GMBH, Internationaler Verlag Der Wissenschaften (2014)paperocamillo100% (3)
- Treatment of Second To Third-Degree Burns in A PDFDocument6 pagesTreatment of Second To Third-Degree Burns in A PDFFebrian Parlangga MuisNo ratings yet
- Sales Manager Job DescriptionDocument8 pagesSales Manager Job Descriptionsalesmanagement264No ratings yet
- Alternate History of The WorldDocument2 pagesAlternate History of The WorldCamille Ann Faigao FamisanNo ratings yet
- MVVNL RGGVY Approved Vendor List: S.NO. Name of Material Vendor Name AddressDocument10 pagesMVVNL RGGVY Approved Vendor List: S.NO. Name of Material Vendor Name AddressELMEF LaboratoryNo ratings yet
- US. Peace Corps Tetun Language CourseDocument305 pagesUS. Peace Corps Tetun Language CoursePeter W Gossner100% (1)
- MLHP Final ListDocument36 pagesMLHP Final Listswapnitha tummaNo ratings yet
- Spare Parts Documentation: TD10004553 EN 00Document69 pagesSpare Parts Documentation: TD10004553 EN 00Emon Sharma100% (1)
- Revilla Law IRRDocument2 pagesRevilla Law IRRPaulNo ratings yet
- 2003catalog PDFDocument25 pages2003catalog PDFPH "Pete" PetersNo ratings yet
- 1 Hot Metal Tapping SOPDocument25 pages1 Hot Metal Tapping SOPSANJAY KUMAR PATINo ratings yet
- Damage Control Surgery in Children: J. HamillDocument5 pagesDamage Control Surgery in Children: J. HamillFebrian Parlangga MuisNo ratings yet
- Damage Control Surgery in Children: J. HamillDocument5 pagesDamage Control Surgery in Children: J. HamillFebrian Parlangga MuisNo ratings yet
- Damage Control Surgery in Children: J. HamillDocument5 pagesDamage Control Surgery in Children: J. HamillFebrian Parlangga MuisNo ratings yet
- Arul 2019Document6 pagesArul 2019Febrian Parlangga MuisNo ratings yet
- Open Book FractureDocument7 pagesOpen Book FractureFebrian Parlangga MuisNo ratings yet
- Glycoprotein Biomarker Panel For Pancreatic Cancer Discovered by Quantitative Proteomics AnalysisDocument12 pagesGlycoprotein Biomarker Panel For Pancreatic Cancer Discovered by Quantitative Proteomics AnalysisFebrian Parlangga MuisNo ratings yet
- Tzeng 2014Document9 pagesTzeng 2014Febrian Parlangga MuisNo ratings yet
- The Role of Cholelithiasis Risk Factors in Stone Types in Cholelithiasis Patients at Usu HospitalDocument7 pagesThe Role of Cholelithiasis Risk Factors in Stone Types in Cholelithiasis Patients at Usu HospitalFebrian Parlangga MuisNo ratings yet
- Surgical Informed Consent Process in Neurosurgery: Review ArticleDocument6 pagesSurgical Informed Consent Process in Neurosurgery: Review ArticleFebrian Parlangga MuisNo ratings yet
- Jkns 60 3 322Document5 pagesJkns 60 3 322Febrian Parlangga MuisNo ratings yet
- 1.1. Data Usia: DescriptivesDocument3 pages1.1. Data Usia: DescriptivesFebrian Parlangga MuisNo ratings yet
- Relationship Between Increased Intracranial Pressure and Mastoid EffusionDocument9 pagesRelationship Between Increased Intracranial Pressure and Mastoid EffusionFebrian Parlangga MuisNo ratings yet
- Emergency TREPP For Strangulated Inguinal Hernia Repair: A Consecutive Case SeriesDocument1 pageEmergency TREPP For Strangulated Inguinal Hernia Repair: A Consecutive Case SeriesFebrian Parlangga MuisNo ratings yet
- Impact of Microbial Findings On PlasticDocument6 pagesImpact of Microbial Findings On PlasticFebrian Parlangga MuisNo ratings yet
- PD-L1 Expression in Triple-Negative Breast Cancer: Research ArticleDocument14 pagesPD-L1 Expression in Triple-Negative Breast Cancer: Research ArticleFebrian Parlangga MuisNo ratings yet
- The History of Bone Marrow in Orthopaedic Surgery (Part I Trauma)Document14 pagesThe History of Bone Marrow in Orthopaedic Surgery (Part I Trauma)Febrian Parlangga MuisNo ratings yet
- Trans-Subxiphoid Robotic Surgery For Anterior Mediastinal DiseaseDocument7 pagesTrans-Subxiphoid Robotic Surgery For Anterior Mediastinal DiseaseFebrian Parlangga MuisNo ratings yet
- Cantinotti 2018Document3 pagesCantinotti 2018Febrian Parlangga MuisNo ratings yet
- FS0008 Toolangi State Forest Walking TrailsDocument2 pagesFS0008 Toolangi State Forest Walking TrailsMichael ConosNo ratings yet
- Choco Cherry BonbonDocument2 pagesChoco Cherry BonbonYarina MoralesNo ratings yet
- FOR of Tution Fee: Application ReimbursementDocument1 pageFOR of Tution Fee: Application ReimbursementBhavithavNo ratings yet
- Scrabble Scrabble Is A Word Game in Which Two or Four Players Score Points by Placing Tiles, EachDocument4 pagesScrabble Scrabble Is A Word Game in Which Two or Four Players Score Points by Placing Tiles, EachNathalie Faye De PeraltaNo ratings yet
- CWTS Narrative ReportDocument10 pagesCWTS Narrative ReportJa Rich100% (1)
- KNOLL and HIERY, The German Colonial Experience - IntroDocument6 pagesKNOLL and HIERY, The German Colonial Experience - IntroGloria MUNo ratings yet
- Corporation Tax CT41G-DciDocument1 pageCorporation Tax CT41G-DciHenry HarrodNo ratings yet
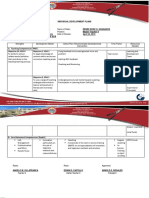
- Individual Development Plans: A. Teaching Competencies (PPST) Objective 13, KRA 4 Objective 1, KRA 1Document2 pagesIndividual Development Plans: A. Teaching Competencies (PPST) Objective 13, KRA 4 Objective 1, KRA 1Angelo VillafrancaNo ratings yet
- The Daily Jinx 0 - ENG-3 (1) - 1Document3 pagesThe Daily Jinx 0 - ENG-3 (1) - 1NoxNo ratings yet
- Managerial Accounting 14th Edition Warren Solutions Manual DownloadDocument28 pagesManagerial Accounting 14th Edition Warren Solutions Manual DownloadRose Speers100% (22)
- Revalida ResearchDocument3 pagesRevalida ResearchJakie UbinaNo ratings yet
- Discuss Both Views Introduction PracticeDocument3 pagesDiscuss Both Views Introduction PracticeSang NguyễnNo ratings yet
- 1167 Nine Planets in TamilDocument1 page1167 Nine Planets in TamilmanijaiNo ratings yet
- ch27 Matrices and ApplicationsDocument34 pagesch27 Matrices and Applicationschowa fellonNo ratings yet
- Essay On Stamp CollectionDocument5 pagesEssay On Stamp Collectionezmt6r5c100% (2)
- Aryaman Gupta: EducationDocument1 pageAryaman Gupta: EducationxoteviNo ratings yet
- DHS/ICE (ICEPIC) Information Sharing Status: Enforcement Systems BranchDocument22 pagesDHS/ICE (ICEPIC) Information Sharing Status: Enforcement Systems BranchImpello_TyrannisNo ratings yet
- RPS Spare CatalogDocument25 pagesRPS Spare Catalogसुरेश चंद Suresh ChandNo ratings yet
- Mapua Cwtsstudentsmodule (Ay08 09)Document62 pagesMapua Cwtsstudentsmodule (Ay08 09)anon-805332No ratings yet