You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Axiatonal Lines Connection IntroductionDocument9 pagesAxiatonal Lines Connection IntroductionDavid Lopes100% (1)
- Sysmex XS-500i PDFDocument4 pagesSysmex XS-500i PDFmohamedNo ratings yet
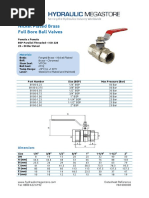
- Brass Low Pressure Ball ValvesDocument1 pageBrass Low Pressure Ball ValvespaniyaNo ratings yet
- Alnor EBT720 - 721 Data SheetDocument2 pagesAlnor EBT720 - 721 Data SheetpaniyaNo ratings yet
- Gree Manual p4Document13 pagesGree Manual p4paniyaNo ratings yet
- ZLT s10 Dialog UsermanualDocument2 pagesZLT s10 Dialog Usermanualpaniya100% (1)
- Rugged 5-In-1 Environmental MeterDocument1 pageRugged 5-In-1 Environmental MeterpaniyaNo ratings yet
- Gree Manual p2Document13 pagesGree Manual p2paniyaNo ratings yet
- HR-V Steering Column Inspection ProcedureDocument4 pagesHR-V Steering Column Inspection ProcedurepaniyaNo ratings yet
- Removal & Installation: Suspension Tire Pressure Monitoring System - Service Information - HR-VDocument1 pageRemoval & Installation: Suspension Tire Pressure Monitoring System - Service Information - HR-VpaniyaNo ratings yet
- Service Manual Installation GuideDocument13 pagesService Manual Installation GuidepaniyaNo ratings yet
- Torque Specifications (Ka/Kc Models)Document5 pagesTorque Specifications (Ka/Kc Models)paniyaNo ratings yet
- Remove evaporator assy from air conditioner service manualDocument13 pagesRemove evaporator assy from air conditioner service manualpaniyaNo ratings yet
- Gree Manual p1Document13 pagesGree Manual p1paniyaNo ratings yet
- Datenblatt / Data Sheet U51DL-012KK-5Document6 pagesDatenblatt / Data Sheet U51DL-012KK-5paniyaNo ratings yet
- Description: Eps System Description - Eps ControlDocument34 pagesDescription: Eps System Description - Eps ControlpaniyaNo ratings yet
- Specification Table: Standards and Service LimitsDocument11 pagesSpecification Table: Standards and Service Limitsvadim vadimNo ratings yet
- Removal & Installation: Steering EPS Motor / Control Unit - Service Information - HR-VDocument2 pagesRemoval & Installation: Steering EPS Motor / Control Unit - Service Information - HR-VpaniyaNo ratings yet
- DTC Troubleshooting: Before You Troubleshoot, Review The General Troubleshooting InformationDocument32 pagesDTC Troubleshooting: Before You Troubleshoot, Review The General Troubleshooting InformationpaniyaNo ratings yet
- 18200776-1c15-496d-8e17-9b69d4f11289Document2 pages18200776-1c15-496d-8e17-9b69d4f11289rdbranaweeraNo ratings yet
- S-849 - December 2018 Page - 3Document1 pageS-849 - December 2018 Page - 3paniyaNo ratings yet
- Ambu PEEP ValvesDocument2 pagesAmbu PEEP ValvespaniyaNo ratings yet
- S-849 - December 2018 Page - 6Document1 pageS-849 - December 2018 Page - 6paniyaNo ratings yet
- Datenblatt / Data Sheet U51DL-012KK-5Document6 pagesDatenblatt / Data Sheet U51DL-012KK-5paniyaNo ratings yet
- S-849 - December 2018 Page - 5Document1 pageS-849 - December 2018 Page - 5paniyaNo ratings yet
- IE PEEPValve 493480001 V03 0413 PDFDocument2 pagesIE PEEPValve 493480001 V03 0413 PDFCoffee ĐenNo ratings yet
- Helix Portable Ventilators: Sustainable First Choice FlexibleDocument3 pagesHelix Portable Ventilators: Sustainable First Choice FlexiblepaniyaNo ratings yet
- Ambu PEEP ValvesDocument2 pagesAmbu PEEP ValvespaniyaNo ratings yet
- 18200776-1c15-496d-8e17-9b69d4f11289Document2 pages18200776-1c15-496d-8e17-9b69d4f11289rdbranaweeraNo ratings yet
- Diaphragm Pump - CompressorDocument2 pagesDiaphragm Pump - CompressorpaniyaNo ratings yet
- AUS PEEPValves 493480097 V02 0712Document2 pagesAUS PEEPValves 493480097 V02 0712paniyaNo ratings yet
- Human Strategies For A Virtual World: Baldwin BergesDocument32 pagesHuman Strategies For A Virtual World: Baldwin BergesmoisesNo ratings yet
- GATE 2004 - Question Paper TF: Textile Engineering and Fiber ScienceDocument29 pagesGATE 2004 - Question Paper TF: Textile Engineering and Fiber ScienceChandra Deep MishraNo ratings yet
- Fabric in ArchitectureDocument28 pagesFabric in ArchitecturesubalakshmiNo ratings yet
- IE 337 Metal Casting Processes & TerminologyDocument48 pagesIE 337 Metal Casting Processes & TerminologylinkinunNo ratings yet
- KidzeeDocument16 pagesKidzeeXLS OfficeNo ratings yet
- Self Healing ConcreteDocument20 pagesSelf Healing ConcreteshivangNo ratings yet
- 2016 CMCDocument536 pages2016 CMCStefan WeissNo ratings yet
- 11 - NRG - Cathodic Protection DesignDocument15 pages11 - NRG - Cathodic Protection DesignBalan100% (1)
- StrippingDocument17 pagesStrippingGhavban David0% (1)
- Pedigree StudiesDocument4 pagesPedigree StudiesJonas WelliverNo ratings yet
- Bypass Sony KDL-55W900A 4X LED Blinking ErrorDocument7 pagesBypass Sony KDL-55W900A 4X LED Blinking ErroruzenNo ratings yet
- Ref1 Tc-211 Eng Ver2Document10 pagesRef1 Tc-211 Eng Ver2Naim ParvejNo ratings yet
- qf001 - Welocalize Supplier Mutual Nda - 2018-Signed PDFDocument9 pagesqf001 - Welocalize Supplier Mutual Nda - 2018-Signed PDFapaci femoNo ratings yet
- TX AsiaDemandForecast 2018Document12 pagesTX AsiaDemandForecast 2018Muhammad AsadNo ratings yet
- Star Ii HoneywellDocument4 pagesStar Ii HoneywellAlejandro MagnoNo ratings yet
- Duracraft Humidifier ManuDocument9 pagesDuracraft Humidifier ManuJulio RodriguezNo ratings yet
- Sika Monotop®-160 Migrating: Product Data SheetDocument3 pagesSika Monotop®-160 Migrating: Product Data Sheetslavisa05No ratings yet
- Pitch Angle Control For A Small-Scale Darrieus VAWTDocument11 pagesPitch Angle Control For A Small-Scale Darrieus VAWThuy4ngooNo ratings yet
- GOLDEN DAWN 3 8 Highlights of The Fourth Knowledge LectureDocument7 pagesGOLDEN DAWN 3 8 Highlights of The Fourth Knowledge LectureF_RCNo ratings yet
- 2 - Chapter Two Horizontal Distance MeasurmentDocument47 pages2 - Chapter Two Horizontal Distance MeasurmentmikeNo ratings yet
- Learning in Artificial IntelligenceDocument6 pagesLearning in Artificial IntelligenceAnikNo ratings yet
- Treadmill Error Code GuideDocument19 pagesTreadmill Error Code GuideŞener MutluNo ratings yet
- Helve Tic ADocument9 pagesHelve Tic AwemeihNo ratings yet
- What Is Agile and Why Do I Care? Blacks in Technology 2018Document44 pagesWhat Is Agile and Why Do I Care? Blacks in Technology 2018AlexJB100% (2)
- ESG V3 SyllabusDocument12 pagesESG V3 SyllabusAaronNo ratings yet
- RXF-C: Air Conditioning Technical DataDocument18 pagesRXF-C: Air Conditioning Technical DataJuan LezamaNo ratings yet
- They Are Product, Price, Placement and PromotionDocument2 pagesThey Are Product, Price, Placement and PromotionVy HoàngNo ratings yet
- Alayo, M. Internationalization and Entrepreneurial Orientation of Family SMEs The Influence of The Family CharacterArticle 2019Document12 pagesAlayo, M. Internationalization and Entrepreneurial Orientation of Family SMEs The Influence of The Family CharacterArticle 2019Riezz MauladiNo ratings yet