You might also like
- USMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsFrom EverandUSMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsRating: 5 out of 5 stars5/5 (9)
- Clinical Management Review 2023-2024: Volume 1: USMLE Step 3 and COMLEX-USA Level 3From EverandClinical Management Review 2023-2024: Volume 1: USMLE Step 3 and COMLEX-USA Level 3Rating: 5 out of 5 stars5/5 (1)
- BAMS Students MnemonicsDocument8 pagesBAMS Students MnemonicsMSKCNo ratings yet
- Expanded Program On Immunization (Philippines)Document14 pagesExpanded Program On Immunization (Philippines)Erick AbarientosNo ratings yet
- Right To Refuse Flu ShotsDocument4 pagesRight To Refuse Flu ShotsBZ Riger100% (2)
- Epi PowerpointDocument29 pagesEpi PowerpointFelisa Lacsamana Gregorio100% (3)
- Expanded Program On Immunization (Philippines)Document14 pagesExpanded Program On Immunization (Philippines)Erick AbarientosNo ratings yet
- Adult ScheduleDocument3 pagesAdult ScheduledrmanojvimalNo ratings yet
- Adult Immunization ScheduleDocument3 pagesAdult Immunization ScheduleBryan Mae H. DegorioNo ratings yet
- Typhoid Fever Follow-Up PDFDocument16 pagesTyphoid Fever Follow-Up PDFPlot BUnniesNo ratings yet
- Guidelines For Vaccination in Normal Adults in India - PMCDocument14 pagesGuidelines For Vaccination in Normal Adults in India - PMCSKMH INSURANCENo ratings yet
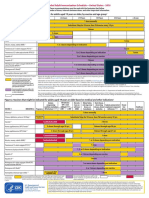
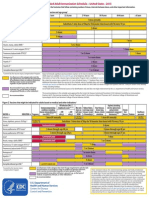
- Figure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupDocument2 pagesFigure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupmsarasNo ratings yet
- Antibiotik For DearrheaDocument11 pagesAntibiotik For DearrheaFerinaTarizaIINo ratings yet
- Research Article: Efforts To Improve Immunization Coverage During Pregnancy Among Ob-GynsDocument9 pagesResearch Article: Efforts To Improve Immunization Coverage During Pregnancy Among Ob-GynsTantiaDeviNo ratings yet
- 6.3.1 PSNZ Influenza Vaccine Reclassification Application Jan 18Document9 pages6.3.1 PSNZ Influenza Vaccine Reclassification Application Jan 18Kresna CahyadiNo ratings yet
- Peace Corps MTG FOIA Volunteer Health SupportDocument199 pagesPeace Corps MTG FOIA Volunteer Health SupportAccessible Journal Media: Peace Corps DocumentsNo ratings yet
- Adult Pocafeket SizeDocument2 pagesAdult Pocafeket SizedadfNo ratings yet
- Health Advice and Immunizations for TravelersFrom EverandHealth Advice and Immunizations for TravelersNo ratings yet
- Ofad 022Document7 pagesOfad 022An iNo ratings yet
- What Everyone Should Know About VaccinesDocument3 pagesWhat Everyone Should Know About VaccinesNicholay AtanassovNo ratings yet
- General Recommendation On ImmunizationDocument19 pagesGeneral Recommendation On ImmunizationRickyNoviantoNo ratings yet
- The Need For Another Typhoid Fever Vaccine: EditorialcommentaryDocument3 pagesThe Need For Another Typhoid Fever Vaccine: Editorialcommentaryshelly_shellyNo ratings yet
- Rotavirus Vaccines: Targeting The Developing World: SupplementarticleDocument7 pagesRotavirus Vaccines: Targeting The Developing World: SupplementarticleAbigailNo ratings yet
- Table 2: Summary of WHO Position Papers - Recommended Routine Immunizations For ChildrenDocument8 pagesTable 2: Summary of WHO Position Papers - Recommended Routine Immunizations For Childrenfadityo1No ratings yet
- Immunization Programs For Infants, Children, Adolescents, and Adults: Clinical Practice Guidelines by The Infectious Diseases Society of AmericaDocument24 pagesImmunization Programs For Infants, Children, Adolescents, and Adults: Clinical Practice Guidelines by The Infectious Diseases Society of AmericaEugene YeboahNo ratings yet
- Cholera ImmunisationDocument2 pagesCholera ImmunisationShynne RPhNo ratings yet
- Seasonal InfluenzaDocument4 pagesSeasonal InfluenzaRachitNo ratings yet
- Art 19661Document4 pagesArt 19661toribio1898No ratings yet
- EPIDocument10 pagesEPIBo ChoiNo ratings yet
- H1N1 Clinician Guidance Final Version1Document2 pagesH1N1 Clinician Guidance Final Version1cha_cruz_6No ratings yet
- VaccineDocument3 pagesVaccinePapitas FritasNo ratings yet
- Diabetes: Primary PreventionDocument7 pagesDiabetes: Primary PreventionVidal IzayNo ratings yet
- Practice Changing UpDates - UpToDateDocument13 pagesPractice Changing UpDates - UpToDatemayteveronica1000No ratings yet
- Adult Combined ScheduleDocument5 pagesAdult Combined SchedulelcmurilloNo ratings yet
- Anaerobe: Lynne V. McfarlandDocument7 pagesAnaerobe: Lynne V. Mcfarlanderna sulistiyawatiNo ratings yet
- Epi NotesDocument5 pagesEpi NoteshoneykrizelNo ratings yet
- Good Health in the Tropics: Advice to Travellers and SettlersFrom EverandGood Health in the Tropics: Advice to Travellers and SettlersNo ratings yet
- Guia de Vacunacion FelinaDocument5 pagesGuia de Vacunacion FelinaRaul KimNo ratings yet
- WSAVA Vaccination Guidelines 2024Document40 pagesWSAVA Vaccination Guidelines 2024Final ShineNo ratings yet
- Vaccine-Preventable Diseases and Vaccines: 6.1 General ConsiderationsDocument63 pagesVaccine-Preventable Diseases and Vaccines: 6.1 General ConsiderationsjuliaNo ratings yet
- Vaccines: Frequency of Adverse Events Following Q Fever Immunisation in Young AdultsDocument13 pagesVaccines: Frequency of Adverse Events Following Q Fever Immunisation in Young AdultslilahgreenyNo ratings yet
- Annex 48 Clinical Guidelines For Covid in Malaysia 4th Edition 19102021 FinaleDocument175 pagesAnnex 48 Clinical Guidelines For Covid in Malaysia 4th Edition 19102021 FinaleEfendi AnuarNo ratings yet
- Rotaviruses Diarrhea: What Are The Benefits of The Rotavirus Vaccine?Document5 pagesRotaviruses Diarrhea: What Are The Benefits of The Rotavirus Vaccine?Mikko ArriesgoddessNo ratings yet
- Table 2: Summary of WHO Position Papers - Recommended Routine Immunizations For ChildrenDocument7 pagesTable 2: Summary of WHO Position Papers - Recommended Routine Immunizations For ChildrenKrishnendu PramanikNo ratings yet
- Annals of Medicine - HPV VaccineDocument12 pagesAnnals of Medicine - HPV VaccineJudicial Watch, Inc.100% (3)
- Nutrients: The Use of Enteral Nutrition in The Management of StrokeDocument6 pagesNutrients: The Use of Enteral Nutrition in The Management of StrokeMiranda MetriaNo ratings yet
- Nutrients: The Use of Enteral Nutrition in The Management of StrokeDocument6 pagesNutrients: The Use of Enteral Nutrition in The Management of StrokeMita SeptoryNo ratings yet
- Expanded Program On ImmunizationDocument4 pagesExpanded Program On ImmunizationMac Lester DumagNo ratings yet
- Types of ImmunizationsDocument21 pagesTypes of Immunizationsmacmactongos100% (6)
- Varicella-Zoster Virus (Chickenpox) : Click The Icon To See An X-Ray of Pneumonia Following Exposure To ChickenpoxDocument4 pagesVaricella-Zoster Virus (Chickenpox) : Click The Icon To See An X-Ray of Pneumonia Following Exposure To ChickenpoxerfinaNo ratings yet
- 1 - CEA - UAS Juni 2020Document9 pages1 - CEA - UAS Juni 2020astri rahayuNo ratings yet
- Akin Et Al Diabetes Vaccination Cost EffectivenessDocument14 pagesAkin Et Al Diabetes Vaccination Cost Effectivenessreza_adrian_2No ratings yet
- Immunization Routine Table1Document9 pagesImmunization Routine Table1MeeKo VideñaNo ratings yet
- Squires 2017Document10 pagesSquires 2017Emile CardNo ratings yet
- Summary of The WHO Position On Rubella Vaccine-July 2020Document3 pagesSummary of The WHO Position On Rubella Vaccine-July 2020Enchantia R. NightshadeNo ratings yet
- Tentang PCVDocument12 pagesTentang PCVJanuwar LukitaNo ratings yet
- National Vaccination ProgramDocument10 pagesNational Vaccination ProgramMysheb SSNo ratings yet
- Adult Combined ScheduleDocument5 pagesAdult Combined ScheduleAwal Safar MNo ratings yet
- SF Vaccination Leaflet - WebDocument12 pagesSF Vaccination Leaflet - Webaakash11No ratings yet
- Stay Healthy, Stay On Top of Vaccinations: CDC Click Here For The CDC's Full Vaccination ChartDocument4 pagesStay Healthy, Stay On Top of Vaccinations: CDC Click Here For The CDC's Full Vaccination ChartcircularreasoningNo ratings yet
- Adult ScheduleDocument3 pagesAdult ScheduleerilarchiNo ratings yet
- Psmid CoAdministration of COVID nonCOVID VaxDocument3 pagesPsmid CoAdministration of COVID nonCOVID VaxarchtgozarNo ratings yet
- 10 JU Detail Fill Up FormDocument2 pages10 JU Detail Fill Up FormMSKCNo ratings yet
- Coconut Oil and Virgin Coconut Oil An Insight IntoDocument3 pagesCoconut Oil and Virgin Coconut Oil An Insight IntoMSKCNo ratings yet
- Pcog Profile of Ageratum Conyzoides PL & Simplicia.Document5 pagesPcog Profile of Ageratum Conyzoides PL & Simplicia.MSKCNo ratings yet
- Korea 6.monograph Part IIDocument239 pagesKorea 6.monograph Part IIMSKCNo ratings yet
- Media EjournalofdenistryDocument3 pagesMedia EjournalofdenistryMSKCNo ratings yet
- ABS Ay Panaceae For Oral HealthDocument1 pageABS Ay Panaceae For Oral HealthMSKCNo ratings yet
- Rasasindura Chandradoya Rasa Pharm AnalDocument3 pagesRasasindura Chandradoya Rasa Pharm AnalMSKCNo ratings yet
- Chapter 03 Respiratory Nafisa Dilshan 102 2221203 - 102Document6 pagesChapter 03 Respiratory Nafisa Dilshan 102 2221203 - 102MSKCNo ratings yet
- SIFCRACT English BrochureDocument6 pagesSIFCRACT English BrochureMSKCNo ratings yet
- Jioh 02 04 010Document4 pagesJioh 02 04 010MSKCNo ratings yet
- Polymorphism Prostate CancerDocument5 pagesPolymorphism Prostate CancerMSKCNo ratings yet
- Oil Pulling Therapy 2008Document2 pagesOil Pulling Therapy 2008MSKCNo ratings yet
- Sunthyadi Yoga Kavala and Pratisarana in TonsillitisDocument2 pagesSunthyadi Yoga Kavala and Pratisarana in TonsillitisMSKCNo ratings yet
- 060 Chemical Properties 10sDocument10 pages060 Chemical Properties 10sMSKCNo ratings yet
- Objectives: The Nature of MatterDocument40 pagesObjectives: The Nature of MatterMSKCNo ratings yet
- 010 Matter and EnergyDocument25 pages010 Matter and EnergyMSKCNo ratings yet
- 050 Chemical and Physical Properties of Matter 13sDocument13 pages050 Chemical and Physical Properties of Matter 13sMSKCNo ratings yet
- 040 Physical & Chemical Properties 13sDocument13 pages040 Physical & Chemical Properties 13sMSKCNo ratings yet
- Electronic Tongue Plant Rasa AIIMS NMRDocument4 pagesElectronic Tongue Plant Rasa AIIMS NMRMSKCNo ratings yet
- Rev Ahara PakaDocument5 pagesRev Ahara PakaMSKCNo ratings yet
- CTRI RA Ay Med Guru Snigdha Guna of Kapha - Clin Higwadi Curna - Sunthyadi Kvath in Ama VataDocument3 pagesCTRI RA Ay Med Guru Snigdha Guna of Kapha - Clin Higwadi Curna - Sunthyadi Kvath in Ama VataMSKCNo ratings yet
- Yuvan Pidika Acne EtiologyDocument8 pagesYuvan Pidika Acne EtiologyMSKCNo ratings yet
- 1 o Tanwar Sthanya KshayaDocument7 pages1 o Tanwar Sthanya KshayaMSKCNo ratings yet
- Ayurveda Perspective of Pediatric Disease (Bala Roga)Document3 pagesAyurveda Perspective of Pediatric Disease (Bala Roga)MSKCNo ratings yet
- 10 Reporting Formats HP Oct2017Document65 pages10 Reporting Formats HP Oct2017Devendra Singh Tomar100% (1)
- eZH Ealth: Dosage Seq. Date (Mm/dd/yyyy) Vaccine Brand Name of Vaccinator Batch No. Lot NoDocument1 pageeZH Ealth: Dosage Seq. Date (Mm/dd/yyyy) Vaccine Brand Name of Vaccinator Batch No. Lot NoRvBombetaNo ratings yet
- Vaccines & AutismDocument5 pagesVaccines & AutismDennis FerrellNo ratings yet
- 2022 To 2024 Workplan National Advisory Committee On Immunization (NACI) - Canada - CaDocument9 pages2022 To 2024 Workplan National Advisory Committee On Immunization (NACI) - Canada - CakelvinkinergyNo ratings yet
- Immunization ReportDocument38 pagesImmunization ReportAlyssa GwenNo ratings yet
- Maklumat Vaksinasi: Vaccination DetailsDocument1 pageMaklumat Vaksinasi: Vaccination DetailsZulkarnain KamalNo ratings yet
- What About Autism?: How Do We Know?Document2 pagesWhat About Autism?: How Do We Know?jenysazedaNo ratings yet
- Quotes On VaccinesDocument25 pagesQuotes On VaccinesilluzoneDOTnet100% (2)
- Toronto Public Health - Immunization of ChildrenDocument8 pagesToronto Public Health - Immunization of ChildrenCityNewsTorontoNo ratings yet
- Novel COVID-19 VaccineDocument25 pagesNovel COVID-19 VaccineJuan VidrioNo ratings yet
- Session 10 KaddarDocument38 pagesSession 10 KaddarsuybaNo ratings yet
- VaccinesDocument29 pagesVaccinesCassandra EnriquezNo ratings yet
- Assignment VDocument2 pagesAssignment VShagun VermaNo ratings yet
- Certificate NayanDocument1 pageCertificate NayanNayan Netaji KumbharNo ratings yet
- Grade 10 Summative TestDocument4 pagesGrade 10 Summative TestJaymar B. MagtibayNo ratings yet
- Complete Vaccine ListingDocument5 pagesComplete Vaccine ListingSyed Esa MushranNo ratings yet
- Diphtheria and MeaslesDocument35 pagesDiphtheria and MeaslesMurugesanNo ratings yet
- Jurnal Difteri English PDFDocument9 pagesJurnal Difteri English PDFLisbet Anita SimamoraNo ratings yet
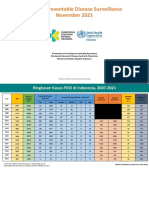
- 11 - VPD Surveillance Performance Analysis 2021 November 2021 (29122021)Document57 pages11 - VPD Surveillance Performance Analysis 2021 November 2021 (29122021)Kiky RizkyNo ratings yet
- DPT VaccinesDocument2 pagesDPT VaccinesSowmiyaNo ratings yet
- Immunization PPT - EditedDocument22 pagesImmunization PPT - EditedAlfred Mutua MutungaNo ratings yet
- COVID - 19 Treatment and VaccinesDocument2 pagesCOVID - 19 Treatment and Vaccinesridwan_olawale_1No ratings yet
- Certificate - 2022-12-23T121112.931Document1 pageCertificate - 2022-12-23T121112.931Hasan JamalNo ratings yet
- Covid VaccinesDocument41 pagesCovid Vaccinesashima mehtaNo ratings yet
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary DetailsK1K5KNo ratings yet
- EPI Scorecard - Sudan - Q1 - 2018Document1 pageEPI Scorecard - Sudan - Q1 - 2018محمد أبو القاسم عليNo ratings yet
- BSN 1a Micro para ReportDocument2 pagesBSN 1a Micro para ReportJohn Steven Bringuelo FloroNo ratings yet
- ImmunisationDocument29 pagesImmunisationOjambo FlaviaNo ratings yet
- Freedom To Choose COVID-19 Vaccine: The Dengvaxia ScareDocument3 pagesFreedom To Choose COVID-19 Vaccine: The Dengvaxia ScareAlyanna Ysabelle VistanNo ratings yet