You might also like
- USMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsFrom EverandUSMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsRating: 5 out of 5 stars5/5 (9)
- Virologic Failure in HIV: An Updated Clinician’s Guide to Assessment and ManagementFrom EverandVirologic Failure in HIV: An Updated Clinician’s Guide to Assessment and ManagementNo ratings yet
- The Sinovac VaccineDocument4 pagesThe Sinovac VaccineMontasir BalambagNo ratings yet
- Adult Combined ScheduleDocument5 pagesAdult Combined SchedulelcmurilloNo ratings yet
- WHO Immunization RecommendationsDocument9 pagesWHO Immunization RecommendationsMeeKo VideñaNo ratings yet
- Adult Combined ScheduleDocument5 pagesAdult Combined ScheduleAwal Safar MNo ratings yet
- WHO Position Papers - Recommended Routine Immunizations for ChildrenDocument8 pagesWHO Position Papers - Recommended Routine Immunizations for Childrenfadityo1No ratings yet
- Adult Immunization Schedule and RecommendationsDocument3 pagesAdult Immunization Schedule and RecommendationsdrmanojvimalNo ratings yet
- Indian Academy of Pediatrics (IAP) Recommended Immunization Schedule 2013Document14 pagesIndian Academy of Pediatrics (IAP) Recommended Immunization Schedule 2013Mahesh ShankarNo ratings yet
- Journal Diare 3Document11 pagesJournal Diare 3ririsofyanNo ratings yet
- Annex 48 Clinical Guidelines For Covid in Malaysia 4th Edition 19102021 FinaleDocument175 pagesAnnex 48 Clinical Guidelines For Covid in Malaysia 4th Edition 19102021 FinaleEfendi AnuarNo ratings yet
- INFECTIOUS DISEASES (November 2021)Document21 pagesINFECTIOUS DISEASES (November 2021)DiegoMosqueraNo ratings yet
- HIV and Pregnancy: How To Manage Conflicting Recommendations From Evidence-Based GuidelinesDocument6 pagesHIV and Pregnancy: How To Manage Conflicting Recommendations From Evidence-Based GuidelinesIsmaelJoséGonzálezGuzmánNo ratings yet
- Figure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupDocument2 pagesFigure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupmsarasNo ratings yet
- WHO 2019 NCoV Vaccines SAGE Recommendation Sinovac CoronaVac 2021.1 EngDocument7 pagesWHO 2019 NCoV Vaccines SAGE Recommendation Sinovac CoronaVac 2021.1 EngMartha Gatica GuevaraNo ratings yet
- Adult ScheduleDocument3 pagesAdult SchedulelcmurilloNo ratings yet
- MY VaxigripTetra NH (0522)Document14 pagesMY VaxigripTetra NH (0522)prasanthgkrishnan1402No ratings yet
- COVID-19 Vaccine Surveillance Report: Week 1Document54 pagesCOVID-19 Vaccine Surveillance Report: Week 1camaferNo ratings yet
- WHO Rotavirus Vaccine Position - Reduce Child DeathsDocument2 pagesWHO Rotavirus Vaccine Position - Reduce Child DeathsYohan MaulanaNo ratings yet
- Interim Recommendations For Use of The Pfizer-Biontech Covid-19 Vaccine, Bnt162B2, Under Emergency Use ListingDocument14 pagesInterim Recommendations For Use of The Pfizer-Biontech Covid-19 Vaccine, Bnt162B2, Under Emergency Use Listingmarie-eve guyNo ratings yet
- WHO 2019 NCoV Vaccines SAGE Recommendation AZD1222 2021.1 EngDocument7 pagesWHO 2019 NCoV Vaccines SAGE Recommendation AZD1222 2021.1 EngChristianNo ratings yet
- WHO 2019 NCoV Vaccines SAGE Recommendation AZD1222 2021.3 EngDocument12 pagesWHO 2019 NCoV Vaccines SAGE Recommendation AZD1222 2021.3 EngAliciaNo ratings yet
- COVID-19 Vaccine Surveillance Report: Week 2Document55 pagesCOVID-19 Vaccine Surveillance Report: Week 2Kosta GavrasNo ratings yet
- Vacunas 2012Document7 pagesVacunas 2012dr.alexisleon9124No ratings yet
- SOGC Guideline on Immunization in PregnancyDocument6 pagesSOGC Guideline on Immunization in PregnancyMohamed SulimanNo ratings yet
- General Recommendation On ImmunizationDocument19 pagesGeneral Recommendation On ImmunizationRickyNoviantoNo ratings yet
- WHO Immunization Schedule ChildrenDocument9 pagesWHO Immunization Schedule Childrenashchua21No ratings yet
- Gardasil LeafletDocument51 pagesGardasil LeafletEllaNo ratings yet
- WWKSF Vaccine EffectivenessDocument18 pagesWWKSF Vaccine Effectivenesspieguy314No ratings yet
- SAGE Updates COVID-19 Vaccination GuidanceDocument5 pagesSAGE Updates COVID-19 Vaccination GuidancejohnNo ratings yet
- Anti Rheumatic Drug in Pregnancy & LactationDocument41 pagesAnti Rheumatic Drug in Pregnancy & LactationNayem comNo ratings yet
- Adult Immunization ScheduleDocument3 pagesAdult Immunization ScheduleBryan Mae H. DegorioNo ratings yet
- Guidelines for Vaccination in Normal Adults in India - PMCDocument14 pagesGuidelines for Vaccination in Normal Adults in India - PMCSKMH INSURANCENo ratings yet
- British Society For Rheumatology Guideline On Prescribing Drugs in Pregnancy and Breastfeeding Immunomodulatory Anti-Rheumatic Drugs and CorticosteroidsDocument41 pagesBritish Society For Rheumatology Guideline On Prescribing Drugs in Pregnancy and Breastfeeding Immunomodulatory Anti-Rheumatic Drugs and CorticosteroidsKori Karina Cueva TovarNo ratings yet
- COVID 19 Vaccines in Pregnancy and Lactation FINALDocument4 pagesCOVID 19 Vaccines in Pregnancy and Lactation FINALBhekisisa HealthNo ratings yet
- Rotavirus Vaccines For Infants - 2019 - UptodateDocument26 pagesRotavirus Vaccines For Infants - 2019 - Uptodatewinnie MontalvoNo ratings yet
- MR Bangladesh Jiw024 2016Document8 pagesMR Bangladesh Jiw024 2016RIRA MABRURATINo ratings yet
- Human Papillomavirus Vaccines Who Position Paper May 2017recomme 2017Document3 pagesHuman Papillomavirus Vaccines Who Position Paper May 2017recomme 2017Putri AlfiraNo ratings yet
- Prospect Prevenar EnglezaDocument63 pagesProspect Prevenar EnglezaNicoleta CiobotarNo ratings yet
- ASRM COVID-19 Vaccine GuidanceDocument4 pagesASRM COVID-19 Vaccine GuidancePatricia FernándezNo ratings yet
- Splenectomy: DisclaimerDocument5 pagesSplenectomy: DisclaimerMimi FatinNo ratings yet
- Interim Recommendations For Use of The Inactivated Covid-19 Vaccine, Coronavac, Developed by SinovacDocument9 pagesInterim Recommendations For Use of The Inactivated Covid-19 Vaccine, Coronavac, Developed by SinovacNathaly BarretoNo ratings yet
- Olagunju 2012Document22 pagesOlagunju 2012Anonymous x4Ba2BNo ratings yet
- Summary of The WHO Position On Rubella Vaccine-July 2020Document3 pagesSummary of The WHO Position On Rubella Vaccine-July 2020Enchantia R. NightshadeNo ratings yet
- Adult Pocafeket SizeDocument2 pagesAdult Pocafeket SizedadfNo ratings yet
- UK Vaccine Surveillance Report Week 42Document29 pagesUK Vaccine Surveillance Report Week 42Cam SlaterNo ratings yet
- UKHSA Vaccine Surveillance Report Week 48Document47 pagesUKHSA Vaccine Surveillance Report Week 48Al StatiliusNo ratings yet
- TDM 41 431Document13 pagesTDM 41 431miss betawiNo ratings yet
- Alarm I: Ourth Dition of The Nternational RogramDocument10 pagesAlarm I: Ourth Dition of The Nternational RogramayfanNo ratings yet
- HIV Cohorte UgandaDocument10 pagesHIV Cohorte UgandaMaluNo ratings yet
- Jama Sha 2019 It 190019Document2 pagesJama Sha 2019 It 190019xtineNo ratings yet
- Management of Premature Rupture of Membranes: Ashraf Olabi and Lucy Shikh MousaDocument7 pagesManagement of Premature Rupture of Membranes: Ashraf Olabi and Lucy Shikh MousaDesi SafiraNo ratings yet
- Section 44Document5 pagesSection 44Mark Christian GlindroNo ratings yet
- Pediatric GuidelinesDocument334 pagesPediatric GuidelinesNovel RamadhaniNo ratings yet
- 2015 Article 794Document9 pages2015 Article 794Hyung ArdiNo ratings yet
- Cervarix LeafletDocument83 pagesCervarix LeafletEllaNo ratings yet
- Therapeutic Changes of Systemic Lupus Erythematosus (SLE) Patients in Pregnancy and Feto-Maternal Outcomes: A Retrospective Cohort StudyDocument14 pagesTherapeutic Changes of Systemic Lupus Erythematosus (SLE) Patients in Pregnancy and Feto-Maternal Outcomes: A Retrospective Cohort StudyayuNo ratings yet
- Kehamilan EktopikDocument9 pagesKehamilan EktopikEka AfriliaNo ratings yet
- The Janssen Ad26.COV2.S COVID-19 Vaccine - What You Need To KnowDocument5 pagesThe Janssen Ad26.COV2.S COVID-19 Vaccine - What You Need To KnowdianavemNo ratings yet
- States, 2011 United Recommended Childhood and Adolescent Immunization SchedulesDocument7 pagesStates, 2011 United Recommended Childhood and Adolescent Immunization SchedulesDolores KilpatrickNo ratings yet
- Approach To The Adult With Nausea and Vomiting - UpToDateDocument20 pagesApproach To The Adult With Nausea and Vomiting - UpToDatemayteveronica1000No ratings yet
- Overview of Infertility and Pregnancy Outcome in Cancer Survivors - UpToDateDocument24 pagesOverview of Infertility and Pregnancy Outcome in Cancer Survivors - UpToDatemayteveronica1000No ratings yet
- Overview of Infertility and Pregnancy Outcome in Cancer Survivors - UpToDateDocument24 pagesOverview of Infertility and Pregnancy Outcome in Cancer Survivors - UpToDatemayteveronica1000No ratings yet
- Patients With Cancer - Overview of The Clinical Features and Diagnosis of Psychiatric Disorders - UpToDateDocument36 pagesPatients With Cancer - Overview of The Clinical Features and Diagnosis of Psychiatric Disorders - UpToDatemayteveronica1000No ratings yet
- Pregestational (Preexisting) Diabetes - Preconception Counseling, Evaluation, and Management - UpToDateDocument40 pagesPregestational (Preexisting) Diabetes - Preconception Counseling, Evaluation, and Management - UpToDatemayteveronica1000No ratings yet
- Electrical Stimulation For Gastroparesis - UpToDateDocument14 pagesElectrical Stimulation For Gastroparesis - UpToDatemayteveronica1000No ratings yet
- Electrical Stimulation For Gastroparesis - UpToDateDocument14 pagesElectrical Stimulation For Gastroparesis - UpToDatemayteveronica1000No ratings yet
- Treatment of Gastroparesis - UpToDateDocument28 pagesTreatment of Gastroparesis - UpToDatemayteveronica1000No ratings yet
- Patients With Cancer - Overview of The Clinical Features and Diagnosis of Psychiatric Disorders - UpToDateDocument36 pagesPatients With Cancer - Overview of The Clinical Features and Diagnosis of Psychiatric Disorders - UpToDatemayteveronica1000No ratings yet
- Approach To The Infant or Child With Nausea and Vomiting - UpToDateDocument47 pagesApproach To The Infant or Child With Nausea and Vomiting - UpToDatemayteveronica1000No ratings yet
- Constrictive Pericarditis - Management and Prognosis - UpToDateDocument22 pagesConstrictive Pericarditis - Management and Prognosis - UpToDatemayteveronica1000No ratings yet
- Hepatic, Pancreatic, and Rare Gastrointestinal Complications of Immune Checkpoint Inhibitor Therapy - UpToDateDocument29 pagesHepatic, Pancreatic, and Rare Gastrointestinal Complications of Immune Checkpoint Inhibitor Therapy - UpToDatemayteveronica1000No ratings yet
- Chylopericardium and Cholesterol Pericarditis - UpToDateDocument15 pagesChylopericardium and Cholesterol Pericarditis - UpToDatemayteveronica1000No ratings yet
- Approach To The Adult With Nausea and Vomiting - UpToDateDocument20 pagesApproach To The Adult With Nausea and Vomiting - UpToDatemayteveronica1000No ratings yet
- Management of Pericardial Effusion and Acute Pericarditis During Pregnancy - UpToDateDocument23 pagesManagement of Pericardial Effusion and Acute Pericarditis During Pregnancy - UpToDatemayteveronica1000No ratings yet
- Postpartum Unipolar Major Depression - General Principles of Treatment - UpToDateDocument15 pagesPostpartum Unipolar Major Depression - General Principles of Treatment - UpToDatemayteveronica1000No ratings yet
- Physiologic Response To Hypoglycemia in Healthy Individuals and Patients With Diabetes MellitusDocument14 pagesPhysiologic Response To Hypoglycemia in Healthy Individuals and Patients With Diabetes Mellitusmayteveronica1000No ratings yet
- Constrictive Pericarditis - Clinical Features and Causes - UpToDateDocument20 pagesConstrictive Pericarditis - Clinical Features and Causes - UpToDatemayteveronica1000No ratings yet
- Anesthesia For Cardiac Surgery - General Principles - UpToDateDocument66 pagesAnesthesia For Cardiac Surgery - General Principles - UpToDatemayteveronica1000No ratings yet
- Body Dysmorphic Disorder - General Principles of Treatment - UpToDateDocument17 pagesBody Dysmorphic Disorder - General Principles of Treatment - UpToDatemayteveronica1000No ratings yet
- Bipolar Major Depression in Adults - General Principles of Treatment - UpToDateDocument23 pagesBipolar Major Depression in Adults - General Principles of Treatment - UpToDatemayteveronica1000No ratings yet
- Approach To The Immunocompromised Patient With Fever and Pulmonary InfiltratesDocument50 pagesApproach To The Immunocompromised Patient With Fever and Pulmonary Infiltratesmayteveronica1000No ratings yet
- Approach To Hypoglycemia in Infants and Children - UpToDateDocument31 pagesApproach To Hypoglycemia in Infants and Children - UpToDateyohanes gabriel dwirianto w.aNo ratings yet
- Clinical Presentation and Diagnostic Evaluation of Ventilator-Associated PneumoniaDocument33 pagesClinical Presentation and Diagnostic Evaluation of Ventilator-Associated Pneumoniamayteveronica1000No ratings yet
- Pegylated Interferon For Treatment of Chronic Hepatitis B Virus InfectionDocument33 pagesPegylated Interferon For Treatment of Chronic Hepatitis B Virus Infectionmayteveronica1000No ratings yet
- Hypoglycemia in Adults With Diabetes MellitusDocument30 pagesHypoglycemia in Adults With Diabetes Mellitusmayteveronica1000No ratings yet
- One Lung Ventilation - General Principles - UpToDateDocument25 pagesOne Lung Ventilation - General Principles - UpToDatemayteveronica1000No ratings yet
- Pneumonia in Children - Inpatient Treatment - UpToDateDocument48 pagesPneumonia in Children - Inpatient Treatment - UpToDatejess.khoo.1204No ratings yet
- Overview of Community-Acquired Pneumonia in AdultsDocument73 pagesOverview of Community-Acquired Pneumonia in Adultsmayteveronica1000No ratings yet
- Opioid Withdrawal in AdolescentsDocument21 pagesOpioid Withdrawal in Adolescentsmayteveronica1000No ratings yet
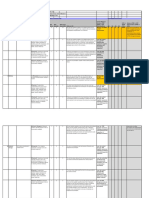
- PROCESS - Risk Assessment & HACCP Planning: Section 7.4.1Document4 pagesPROCESS - Risk Assessment & HACCP Planning: Section 7.4.1Wisnu samuel Atmaja triwarsitaNo ratings yet
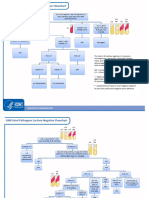
- GNR Stool Pathogens Lactose Negative FlowchartDocument2 pagesGNR Stool Pathogens Lactose Negative FlowchartKeithNo ratings yet
- Hospital departments, medical terms, and anatomyDocument18 pagesHospital departments, medical terms, and anatomyThanh ToànNo ratings yet
- NCM 103 Administering Intramuscular MedicationDocument16 pagesNCM 103 Administering Intramuscular MedicationAdrynnette Cruz-LastimadoNo ratings yet
- LAC 2-OUTPUT On LDM2Document10 pagesLAC 2-OUTPUT On LDM2NaruffRalliburNo ratings yet
- Experienced Pharmacist Seeking New OpportunityDocument3 pagesExperienced Pharmacist Seeking New OpportunityIman ElshafieNo ratings yet
- JVSM 2325 4645 05 0032Document9 pagesJVSM 2325 4645 05 0032Yayew MaruNo ratings yet
- Indian EthosDocument19 pagesIndian Ethosshahid veettil100% (2)
- Safety and Influence of A Novel Powder Form of Coconut Inflorescence Sap On Glycemic Index and LipidDocument1 pageSafety and Influence of A Novel Powder Form of Coconut Inflorescence Sap On Glycemic Index and LipidPriscila CerqueiraNo ratings yet
- Analysis of The Causes and Effects of Recidivism in The Nigerian Prison System Otu, M - SorochiDocument10 pagesAnalysis of The Causes and Effects of Recidivism in The Nigerian Prison System Otu, M - SorochiFahad MemonNo ratings yet
- Sylvia PlathDocument12 pagesSylvia Plathapi-534201968No ratings yet
- Muscle & Fittness: Resents TheDocument34 pagesMuscle & Fittness: Resents TheauqaabNo ratings yet
- Narrative ReportDocument2 pagesNarrative ReportRhisia RaborNo ratings yet
- Case Study Attendance Score DisputeDocument3 pagesCase Study Attendance Score DisputeSyed Aamir Ahmed0% (2)
- Reading 3Document3 pagesReading 3Astri R SitumorangNo ratings yet
- Ey Work SampleDocument10 pagesEy Work SampleKris ANo ratings yet
- Breastfeeding Benefits and RecommendationsDocument46 pagesBreastfeeding Benefits and RecommendationsPriya bhattiNo ratings yet
- Introduction To Criminology: By: Catherine G. Acedo, RcrimDocument34 pagesIntroduction To Criminology: By: Catherine G. Acedo, RcrimJEEHAN DELA CRUZNo ratings yet
- Essential Falls Management Series: Managing Falls in Assisted Living (Tideiksaar Excerpt)Document11 pagesEssential Falls Management Series: Managing Falls in Assisted Living (Tideiksaar Excerpt)Health Professions Press, an imprint of Paul H. Brookes Publishing Co., Inc.No ratings yet
- Grade 8 BowDocument7 pagesGrade 8 BowJorely Barbero MundaNo ratings yet
- The History of The Treatment of Maxillo-Facial TraumaDocument21 pagesThe History of The Treatment of Maxillo-Facial TraumaThanh NguyễnNo ratings yet
- Improve Balance and Coordination with Soccer LessonsDocument9 pagesImprove Balance and Coordination with Soccer LessonsAlvin Corpuz JrNo ratings yet
- Research Paper Topics For Developmental PsychologyDocument7 pagesResearch Paper Topics For Developmental PsychologyxbvtmpwgfNo ratings yet
- UPSC Prelims 2021 Geography Revision: High Probable Topics Part 2Document86 pagesUPSC Prelims 2021 Geography Revision: High Probable Topics Part 2PreethiNo ratings yet
- What Is Criminal Rehabilitation?: Lisa Forsberg Thomas DouglasDocument24 pagesWhat Is Criminal Rehabilitation?: Lisa Forsberg Thomas DouglasAisa VenturaNo ratings yet
- HTTPS: - Dacemirror - Sci-Hub - TW - Journal-Article - Soares2017 PDFDocument10 pagesHTTPS: - Dacemirror - Sci-Hub - TW - Journal-Article - Soares2017 PDFdarinsafinazNo ratings yet
- CareGroup Case Study QuestionsDocument1 pageCareGroup Case Study QuestionsEnrica Melissa PanjaitanNo ratings yet
- 9 ErDocument13 pages9 Ermartin Ignacio Zapata LaguadoNo ratings yet
- DSP 15-12-23Document36 pagesDSP 15-12-23Fu'ad ParkhaniNo ratings yet
- Reducing Negativity in A WorkplaceDocument12 pagesReducing Negativity in A WorkplaceAna Jane Morales CasaclangNo ratings yet