You might also like
- What Can Science Tell Us About DeathDocument5 pagesWhat Can Science Tell Us About DeathGG7M1 gervacioNo ratings yet
- What Happens When We DieDocument2 pagesWhat Happens When We DieTsenguujinNo ratings yet
- Continuity of Consciousness After DeathDocument42 pagesContinuity of Consciousness After Deathdick_henriqueNo ratings yet
- 7 Reasons to Believe in the Afterlife: A Doctor Reviews the Case for Consciousness after DeathFrom Everand7 Reasons to Believe in the Afterlife: A Doctor Reviews the Case for Consciousness after DeathNo ratings yet
- Near-Death Experience - Consciousness and The Brain - LommelDocument18 pagesNear-Death Experience - Consciousness and The Brain - LommelAndrás SzabóNo ratings yet
- Mind Over Matter: Evidence That Consciousness Is Connected To, and Affects The Physical World Around UsDocument25 pagesMind Over Matter: Evidence That Consciousness Is Connected To, and Affects The Physical World Around UsKosta KourabisNo ratings yet
- Is Brain Death Actually DeathDocument20 pagesIs Brain Death Actually DeathMário RibeiroNo ratings yet
- THE PROOFS OF LIFE AFTER DEATH Robert ThompsonDocument370 pagesTHE PROOFS OF LIFE AFTER DEATH Robert ThompsonericstevencookNo ratings yet
- Annals NY Academy of Science - 2022 - Parnia - Guidelines and Standards For The Study of Death and Recalled Experiences ofDocument17 pagesAnnals NY Academy of Science - 2022 - Parnia - Guidelines and Standards For The Study of Death and Recalled Experiences ofValter da Rosa BorgesNo ratings yet
- Turning the Hourglass: Children’S Passage Through Traumas and Past LivesFrom EverandTurning the Hourglass: Children’S Passage Through Traumas and Past LivesNo ratings yet
- Beyond Knowing: Mysteries and Messages of Death and Life from a Forensic PathologistFrom EverandBeyond Knowing: Mysteries and Messages of Death and Life from a Forensic PathologistRating: 4.5 out of 5 stars4.5/5 (6)
- Quanta, Spirit, and Mindful Matter: A Journey Beyond the Sixth SenseFrom EverandQuanta, Spirit, and Mindful Matter: A Journey Beyond the Sixth SenseNo ratings yet
- Raymond Moody, Life After Life Executive SummaryDocument12 pagesRaymond Moody, Life After Life Executive SummaryGudipi Janardhan100% (1)
- Greene Journal of Near Death Studies - 1999!17!151 191Document41 pagesGreene Journal of Near Death Studies - 1999!17!151 191360DNo ratings yet
- Beyond Earth Through Heaven’S Gates: Communication and Insights from Our Spiritual WorldFrom EverandBeyond Earth Through Heaven’S Gates: Communication and Insights from Our Spiritual WorldNo ratings yet
- Journey to Infinity: The Quest for Eternal Life and the Secrets of Immortality: Religion and SpiritualityFrom EverandJourney to Infinity: The Quest for Eternal Life and the Secrets of Immortality: Religion and SpiritualityNo ratings yet
- (Re-) Mapping The Concept of DreamingDocument5 pages(Re-) Mapping The Concept of DreamingEduardo VLNo ratings yet
- The Modern Book of the Dead: A Revolutionary Perspective on Death, the Soul, and What Really Happens in the Life to ComeFrom EverandThe Modern Book of the Dead: A Revolutionary Perspective on Death, the Soul, and What Really Happens in the Life to ComeNo ratings yet
- Clairvoyance (Barnes & Noble Digital Library)From EverandClairvoyance (Barnes & Noble Digital Library)Rating: 2.5 out of 5 stars2.5/5 (3)
- Understanding Heaven: Research and Personal Views of the AfterlifeFrom EverandUnderstanding Heaven: Research and Personal Views of the AfterlifeNo ratings yet
- Death - A Mysterious PhenomenonDocument3 pagesDeath - A Mysterious PhenomenonDr. Farida ViraniNo ratings yet
- Life After Death: Why Reincarnation Is The Only Afterlife Option : Who Were You In The Past And Who You Will Be In The FutureFrom EverandLife After Death: Why Reincarnation Is The Only Afterlife Option : Who Were You In The Past And Who You Will Be In The FutureNo ratings yet
- The Last Frontier: Exploring the Afterlife and Transforming Our Fear of DeathFrom EverandThe Last Frontier: Exploring the Afterlife and Transforming Our Fear of DeathRating: 2.5 out of 5 stars2.5/5 (2)
- Beyond the Veil to Heaven: Inexplicable Manifestations and Signs from a Woman’S Transition to Heaven While Maintaining Earthly Life ConnectionsFrom EverandBeyond the Veil to Heaven: Inexplicable Manifestations and Signs from a Woman’S Transition to Heaven While Maintaining Earthly Life ConnectionsNo ratings yet
- The Force Is With Us: The Higher Consciousness That Science Refuses to AcceptFrom EverandThe Force Is With Us: The Higher Consciousness That Science Refuses to AcceptNo ratings yet
- The Haunted Mind:: A Psychoanalyst Looks at the SupernaturalFrom EverandThe Haunted Mind:: A Psychoanalyst Looks at the SupernaturalRating: 4 out of 5 stars4/5 (2)
- What Happens When We Die TheoryDocument4 pagesWhat Happens When We Die TheoryMartin TuzimNo ratings yet
- Messages From The Spirit Realm: An Overview of the After LifeFrom EverandMessages From The Spirit Realm: An Overview of the After LifeNo ratings yet
- There Is Nothing Paranormal About Near-Death PDFDocument3 pagesThere Is Nothing Paranormal About Near-Death PDFMohammad Al-SalehNo ratings yet
- Taking The Paranormal and Spiritual World Seriously. Theories: Thoughts - ExperiencesFrom EverandTaking The Paranormal and Spiritual World Seriously. Theories: Thoughts - ExperiencesNo ratings yet
- Case Study Review - Morton GhostDocument5 pagesCase Study Review - Morton GhostBryan J WilliamsNo ratings yet
- Is There Life After DeathDocument4 pagesIs There Life After DeathWasif IrfanNo ratings yet
- Download: Afterlife Uncovering The Secrets of Life After DeathDocument2 pagesDownload: Afterlife Uncovering The Secrets of Life After DeathsteveNo ratings yet
- CarlJung PsiEncyclopediaDocument25 pagesCarlJung PsiEncyclopediaDjane VillarinNo ratings yet
- Near Death Experiences Astounding True Stories Lifestyle TransformationsFrom EverandNear Death Experiences Astounding True Stories Lifestyle TransformationsRating: 3 out of 5 stars3/5 (1)
- A - The Man and His Activities: Cod e Image Phonetic Value Ideogram and Phonogram Illustrated Article UseDocument45 pagesA - The Man and His Activities: Cod e Image Phonetic Value Ideogram and Phonogram Illustrated Article UseSlopa StefanNo ratings yet
- Life-Inevitable or FlukeDocument7 pagesLife-Inevitable or FlukeSlopa StefanNo ratings yet
- Hawking's 'Escher-Verse' Could Be Theory of EverythingDocument3 pagesHawking's 'Escher-Verse' Could Be Theory of EverythingSlopa StefanNo ratings yet
- Engineering Lifelong RomanceDocument3 pagesEngineering Lifelong RomanceSlopa StefanNo ratings yet
- Neutrinos - The Next Big Small ThingDocument7 pagesNeutrinos - The Next Big Small ThingSlopa StefanNo ratings yet
- Hawking's 'Escher-Verse' Could Be Theory of EverythingDocument3 pagesHawking's 'Escher-Verse' Could Be Theory of EverythingSlopa StefanNo ratings yet
- First Glimpse at How Viruses May Have Invented DNADocument3 pagesFirst Glimpse at How Viruses May Have Invented DNASlopa StefanNo ratings yet
- Death-The Blurred Line Between Dead and AliveDocument3 pagesDeath-The Blurred Line Between Dead and AliveSlopa StefanNo ratings yet
- Before The Big BangDocument4 pagesBefore The Big BangSlopa StefanNo ratings yet
- Engineering Lifelong RomanceDocument3 pagesEngineering Lifelong RomanceSlopa StefanNo ratings yet
- 11 Particles For 11 Physics PuzzlesDocument7 pages11 Particles For 11 Physics PuzzlesSlopa StefanNo ratings yet
- Decoding Antiquity: Eight Scripts That Still Can't Be Read: Andrew Robinson Subscribe and Save HistoriesDocument8 pagesDecoding Antiquity: Eight Scripts That Still Can't Be Read: Andrew Robinson Subscribe and Save HistoriesSlopa StefanNo ratings yet
- Was the First Craniate on the Road to CognitionDocument17 pagesWas the First Craniate on the Road to CognitionSlopa StefanNo ratings yet
- EightDocument1 pageEightSlopa StefanNo ratings yet
- TreeDocument1 pageTreeAlexander VZNo ratings yet
- TreeDocument1 pageTreeAlexander VZNo ratings yet
- A SARS-like Cluster of Circulating Bat Coronaviruses Shows Potential For Human EmergenceDocument8 pagesA SARS-like Cluster of Circulating Bat Coronaviruses Shows Potential For Human EmergenceSavingtheRepubliccomNo ratings yet
- Abundant Ammonia in Primitive Asteroids - ExobiologyDocument4 pagesAbundant Ammonia in Primitive Asteroids - ExobiologySlopa StefanNo ratings yet
- Abundant Ammonia in Primitive Asteroids - ExobiologyDocument4 pagesAbundant Ammonia in Primitive Asteroids - ExobiologySlopa StefanNo ratings yet
- Annexure I: Block / Building Fire Safety Audit-Check List Fire Safety Audit ChecklistDocument5 pagesAnnexure I: Block / Building Fire Safety Audit-Check List Fire Safety Audit ChecklistGaurav Singh67% (3)
- Ultrasound-Guided Lumbar Central Neuraxial Block 2016Document8 pagesUltrasound-Guided Lumbar Central Neuraxial Block 2016drkis20100% (1)
- Cricket Academy Head Coach RoleDocument4 pagesCricket Academy Head Coach Roletauseef1716No ratings yet
- Five Feet Apart ReviewDocument7 pagesFive Feet Apart ReviewBianca HequilanNo ratings yet
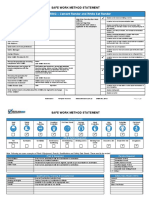
- 3075 SWMS RendererDocument13 pages3075 SWMS Renderernik KooNo ratings yet
- Lifting Vs Volumizing-The Difference in Facial Minimally Invasive Procedures When Respecting The Line of LigamentsDocument7 pagesLifting Vs Volumizing-The Difference in Facial Minimally Invasive Procedures When Respecting The Line of LigamentsArcelino Farias100% (1)
- Opiates 1986 George R Lenz Suzanne M Evans D Eric Walters Anton J Hopfinger Academic Press ISBN 012443830X 0-12-443830 X 978 0124438309Document287 pagesOpiates 1986 George R Lenz Suzanne M Evans D Eric Walters Anton J Hopfinger Academic Press ISBN 012443830X 0-12-443830 X 978 0124438309Nick Coffey100% (4)
- CPT 2021 guide for identifying medical proceduresDocument7 pagesCPT 2021 guide for identifying medical proceduresChester FernandezNo ratings yet
- Immediate DenturesDocument35 pagesImmediate DenturesSimran SahniNo ratings yet
- VGEC 2024_Thư mời hội nghịDocument8 pagesVGEC 2024_Thư mời hội nghịkhongquantam101010No ratings yet
- 1992 2007 Kpds Ilgisiz Cumle Sorulari Seyfihocacom - Pdf.pdfsifreDocument24 pages1992 2007 Kpds Ilgisiz Cumle Sorulari Seyfihocacom - Pdf.pdfsifreozgurekinsuNo ratings yet
- Affidavit of Accident Dominador Rosario BagamaspadDocument2 pagesAffidavit of Accident Dominador Rosario BagamaspadJaime GonzalesNo ratings yet
- Display PDFDocument8 pagesDisplay PDFSri BalajiNo ratings yet
- Health Information Technology-HISMLSDocument1 pageHealth Information Technology-HISMLSJanela Escalante TaboraNo ratings yet
- Project ProposalDocument16 pagesProject ProposalMashaal FasihNo ratings yet
- Vitamin Water - Arnel Ricafranca PDFDocument32 pagesVitamin Water - Arnel Ricafranca PDFAlaa EssamNo ratings yet
- 4.schedule Waste Management UTM - SWMP - 22mei2018 PDFDocument54 pages4.schedule Waste Management UTM - SWMP - 22mei2018 PDFfaraNo ratings yet
- 100 Item Exam On Fundamentals of Nursing - Pulse - Blood Pressure PDFDocument12 pages100 Item Exam On Fundamentals of Nursing - Pulse - Blood Pressure PDFJawad AkbarNo ratings yet
- Connectors 2Document14 pagesConnectors 2Irene SánchezNo ratings yet
- Nursing and Midwifery Board Candidate Handbook RN OSCE ExaminationDocument25 pagesNursing and Midwifery Board Candidate Handbook RN OSCE ExaminationkemalayazNo ratings yet
- PIL For Sudafed DecongestantDocument2 pagesPIL For Sudafed DecongestantOdunlamiNo ratings yet
- Unilag MSC Environmenatl Toxicology SampleDocument4 pagesUnilag MSC Environmenatl Toxicology SamplebdianNo ratings yet
- 2020 Lamberti RCT Effectiveness of RBFT Slow Walking On Mobility in Severe Multiple SclerosisDocument11 pages2020 Lamberti RCT Effectiveness of RBFT Slow Walking On Mobility in Severe Multiple SclerosisArmin ParavlićNo ratings yet
- Vacation With Sunny Leone - Without FlightDocument4 pagesVacation With Sunny Leone - Without FlightkalidasdoraemonNo ratings yet
- Penile Injection TherapyDocument4 pagesPenile Injection Therapydr NayanBharadwajNo ratings yet
- Appendix7 I-131Document4 pagesAppendix7 I-131Crizzz001No ratings yet
- MSDS for Feldspar PowderDocument7 pagesMSDS for Feldspar PowderRıdvan SürmeliNo ratings yet
- Can Mindfulness in Health Care Professionals Improve Patient Care An Integrative Review and Proposed Model.Document15 pagesCan Mindfulness in Health Care Professionals Improve Patient Care An Integrative Review and Proposed Model.ALIXNo ratings yet
- Press Final - Abstract Book PDFDocument157 pagesPress Final - Abstract Book PDFAmbesh JhaNo ratings yet
- Insurance Fraud PPT (Final)Document30 pagesInsurance Fraud PPT (Final)Gaurav Savlani83% (6)