You might also like
- Types and Causes of Burns ExplainedDocument4 pagesTypes and Causes of Burns Explainedgreshel254981No ratings yet
- Burn Types, Causes, Classification and TreatmentDocument10 pagesBurn Types, Causes, Classification and TreatmentSonny Dizon PareñasNo ratings yet
- Arianne Bernardo BSN-3B1: Erythema Pain Epidermis Sunburns Blistering Nerve DermisDocument5 pagesArianne Bernardo BSN-3B1: Erythema Pain Epidermis Sunburns Blistering Nerve DermisArianne BernardoNo ratings yet
- Burn RehabilitationDocument14 pagesBurn Rehabilitationoo2eeNo ratings yet
- Types of BurnsDocument5 pagesTypes of BurnsJheanAlphonsineT.Means100% (2)
- Arsuri Burns ENGDocument82 pagesArsuri Burns ENGRomanescu RalucaNo ratings yet
- Luka Bakar Dan ListrikDocument55 pagesLuka Bakar Dan Listrikramadhanadlansyah7No ratings yet
- Luka Bakar Dan ListrikDocument55 pagesLuka Bakar Dan Listrikramadhanadlansyah7No ratings yet
- Understanding Burn DegreesDocument2 pagesUnderstanding Burn DegreesAnu TripathiNo ratings yet
- A Wound With Coagulative Necrosis Is Called Burn. A Burn Is A Wound in Which There Is Coagulative Necrosis of The TissueDocument17 pagesA Wound With Coagulative Necrosis Is Called Burn. A Burn Is A Wound in Which There Is Coagulative Necrosis of The Tissuewww nambisons comNo ratings yet
- BurnsDocument1 pageBurnsasdfghjNo ratings yet
- Skin ShortDocument10 pagesSkin ShortKashar SaeedNo ratings yet
- Burns: Major and Minor BurnsDocument25 pagesBurns: Major and Minor BurnsTrisha TannerNo ratings yet
- BurnsDocument3 pagesBurnsShaz Zrin100% (1)
- Deep Partial Thickness BurnsDocument8 pagesDeep Partial Thickness BurnsHencynt SoriaNo ratings yet
- BURNDocument39 pagesBURNMuhammad MakkiNo ratings yet
- BURNSDocument93 pagesBURNSRobin Mathew0% (1)
- Review and Comprehension P. 108 (Madayag, Rachel Eve G)Document2 pagesReview and Comprehension P. 108 (Madayag, Rachel Eve G)Rachel MadayagNo ratings yet
- Burns and ShockDocument13 pagesBurns and Shockjames garciaNo ratings yet
- Burn IntroDocument2 pagesBurn IntroAllis RubioNo ratings yet
- Burns AmbossDocument9 pagesBurns AmbossPati MuresanNo ratings yet
- Burns AmbossDocument9 pagesBurns AmbossPati MuresanNo ratings yet
- Medterm IntegumentaryDocument10 pagesMedterm IntegumentaryVince BalloriNo ratings yet
- Integumentary System Functions and StructureDocument12 pagesIntegumentary System Functions and StructureLly Isidoro100% (2)
- Skin Structure and FunctionsDocument25 pagesSkin Structure and FunctionsUniversal DiscoveringNo ratings yet
- Burn RehabilitationDocument5 pagesBurn Rehabilitationdrng48No ratings yet
- Burns SemDocument29 pagesBurns SemEsther Marie SazonNo ratings yet
- Integumentary System (Skin)Document35 pagesIntegumentary System (Skin)Holly TadesseNo ratings yet
- Medical Classification of BurnsDocument1 pageMedical Classification of Burnsscartoneros_1No ratings yet
- NCM 104 - SensoryDocument149 pagesNCM 104 - SensoryveralynnpNo ratings yet
- Luka Bakar Nov 2017 BanjarmasinDocument52 pagesLuka Bakar Nov 2017 BanjarmasinNovita RidhaNo ratings yet
- Chapter 5 Integumentary Study GuideDocument3 pagesChapter 5 Integumentary Study GuideSuperjunior8No ratings yet
- By: Aileen C. Contreras-Limjoco M.DDocument48 pagesBy: Aileen C. Contreras-Limjoco M.Dclara jocomilNo ratings yet
- Anaphy ReviewerDocument8 pagesAnaphy ReviewerMark GonzalesNo ratings yet
- The Integumentary System: DermisDocument11 pagesThe Integumentary System: DermisAnonymous AVSgz8UNo ratings yet
- Nursing Care Plan of Integument SystemDocument27 pagesNursing Care Plan of Integument SystemAlfianGafar67% (3)
- Sensory Skin DisorderDocument149 pagesSensory Skin Disorderfhey19No ratings yet
- Burns: Picture of Wound Wound Indicator/descriptor Management Aims Recommended Products Relevant LinksDocument3 pagesBurns: Picture of Wound Wound Indicator/descriptor Management Aims Recommended Products Relevant Linksfrenzie_velocityNo ratings yet
- Integumentary System: Skin and Its DerivativesDocument39 pagesIntegumentary System: Skin and Its DerivativesGlory Ann BautistaNo ratings yet
- Burns Etiology & ClassificationDocument31 pagesBurns Etiology & Classificationahmedzakaria0No ratings yet
- Zoology Lecture (Reviewer)Document4 pagesZoology Lecture (Reviewer)Maria GrasyaNo ratings yet
- HUMAN ORGAN SYSTEMS: INTEGUMENTARY AND SKELETALDocument3 pagesHUMAN ORGAN SYSTEMS: INTEGUMENTARY AND SKELETALDenine Dela Rosa OrdinalNo ratings yet
- 4integumentary SystemDocument139 pages4integumentary SystemMargreth MontejoNo ratings yet
- Assesment For Burns and Fluid Calculation PDFDocument10 pagesAssesment For Burns and Fluid Calculation PDFRagaviNo ratings yet
- Integumentary System: Burns and Wounds Clinical Case Study: Degree Burn Depth in Dermal Layers Description ImageDocument6 pagesIntegumentary System: Burns and Wounds Clinical Case Study: Degree Burn Depth in Dermal Layers Description ImageGabrielitoNo ratings yet
- BurnsDocument20 pagesBurnsrazAn swNo ratings yet
- bURNS NCLEXDocument10 pagesbURNS NCLEXpapa.pradoNo ratings yet
- Effective Skin Care For WomenDocument7 pagesEffective Skin Care For WomenFeirniadoll100% (1)
- Types of BurnsDocument6 pagesTypes of BurnsKavita WahiNo ratings yet
- Integumentary SystemDocument3 pagesIntegumentary SystemLindley PareñoNo ratings yet
- Burn Injury. Frostbite. Elrctrotrauma: Department of General SurgeryDocument135 pagesBurn Injury. Frostbite. Elrctrotrauma: Department of General SurgeryIbrahim AlmahmoudNo ratings yet
- Anatomy and Physiology-NotesDocument6 pagesAnatomy and Physiology-NotesAkirah Jewelle JaenNo ratings yet
- PhysiotherapyinburnsDocument93 pagesPhysiotherapyinburnsFinal internalNo ratings yet
- Burns 2Document34 pagesBurns 2Vaibhavi JainNo ratings yet
- SG3 - Burns ManagementDocument90 pagesSG3 - Burns ManagementDiyana ZatyNo ratings yet
- Finals MaternalDocument30 pagesFinals MaternalPreciousmae Talay JavierNo ratings yet
- Functions of The Integumentary SystemDocument7 pagesFunctions of The Integumentary SystemRoan MalicdemNo ratings yet
- DermatologyDocument15 pagesDermatologyAjay The RockerNo ratings yet
- How To Pick A CandidateDocument2 pagesHow To Pick A CandidateJeffrey KauvaNo ratings yet
- Amniotic Fluid VolumeDocument9 pagesAmniotic Fluid VolumeJeffrey KauvaNo ratings yet
- AnhydramnionDocument3 pagesAnhydramnionNi Wayan Ana PsNo ratings yet
- Amniotic Fluid Volume Rapid MR-based Assessment at 28-32 Weeks Gestation PDFDocument9 pagesAmniotic Fluid Volume Rapid MR-based Assessment at 28-32 Weeks Gestation PDFJeffrey KauvaNo ratings yet
- Amniotic Fluid Volume Rapid MR-based Assessment at 28-32 Weeks Gestation PDFDocument9 pagesAmniotic Fluid Volume Rapid MR-based Assessment at 28-32 Weeks Gestation PDFJeffrey KauvaNo ratings yet
- Amniotic Fluid and It's Abnormalities PDFDocument13 pagesAmniotic Fluid and It's Abnormalities PDFJeffrey KauvaNo ratings yet
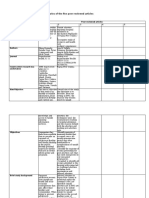
- Matrix 1: Critical Analysis Summaries of The Five Peer-Reviewed Articles Consequences andDocument9 pagesMatrix 1: Critical Analysis Summaries of The Five Peer-Reviewed Articles Consequences andJeffrey KauvaNo ratings yet
- Pacific Adventist University 2020 Academic CalendarDocument2 pagesPacific Adventist University 2020 Academic CalendarJeffrey KauvaNo ratings yet
- Physiology and Care During The Third Stage of LaborDocument2 pagesPhysiology and Care During The Third Stage of LaborJeffrey KauvaNo ratings yet
- Literature Review StrategiesDocument2 pagesLiterature Review Strategiesizeldien5870No ratings yet
- AMENDED Master Timetable (SoE PERIOD) - 27 April 2020Document28 pagesAMENDED Master Timetable (SoE PERIOD) - 27 April 2020Jeffrey KauvaNo ratings yet
- Literature Review Template: Writing CentreDocument1 pageLiterature Review Template: Writing CentreSeftiwin SungaNo ratings yet
- Assignment - Coverpage M&INDocument1 pageAssignment - Coverpage M&INJeffrey KauvaNo ratings yet
- Pulmonary Hypertension: 1. Identify Pulmonary Hypertension 2. Apply Required Collaborative and Nursing Care PlanDocument14 pagesPulmonary Hypertension: 1. Identify Pulmonary Hypertension 2. Apply Required Collaborative and Nursing Care PlanJeffrey KauvaNo ratings yet
- CCU Cognitive IssuesDocument15 pagesCCU Cognitive IssuesJeffrey KauvaNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument25 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsJeffrey KauvaNo ratings yet
- Critical Care EnvironmentDocument16 pagesCritical Care EnvironmentJeffrey KauvaNo ratings yet
- HN321 Subject Outline S120 CSDocument11 pagesHN321 Subject Outline S120 CSJeffrey KauvaNo ratings yet
- Taping Techniques: Moazzam Hussain Khan M.P.T. Sports Medicine New DelhiDocument38 pagesTaping Techniques: Moazzam Hussain Khan M.P.T. Sports Medicine New DelhiMeena SharmaNo ratings yet
- Causes of Baby Dumping: Family Breakups, Lack of Education, and PovertyDocument2 pagesCauses of Baby Dumping: Family Breakups, Lack of Education, and Povertysirthana697547No ratings yet
- Nelson Textbook of Pediatrics (2-Volume Set) by Robert M. Kliegman, Bonita F. Stanton, Joseph W. ST Geme III, Nina F. SchorDocument312 pagesNelson Textbook of Pediatrics (2-Volume Set) by Robert M. Kliegman, Bonita F. Stanton, Joseph W. ST Geme III, Nina F. SchorFaisal MomenNo ratings yet
- Plant Tissue Culture Media PDFDocument3 pagesPlant Tissue Culture Media PDFTitan Biotech100% (1)
- Careers Surrey 20181Document15 pagesCareers Surrey 20181Kevin_Nguyen117No ratings yet
- Quality Improvement: The Model For Improvement, PDSA Cycles, and Accelerating ImprovementDocument37 pagesQuality Improvement: The Model For Improvement, PDSA Cycles, and Accelerating ImprovementDewi ListyoriniNo ratings yet
- Nursing and Midwifery Board Candidate Handbook RN OSCE ExaminationDocument25 pagesNursing and Midwifery Board Candidate Handbook RN OSCE ExaminationkemalayazNo ratings yet
- 2020 Lamberti RCT Effectiveness of RBFT Slow Walking On Mobility in Severe Multiple SclerosisDocument11 pages2020 Lamberti RCT Effectiveness of RBFT Slow Walking On Mobility in Severe Multiple SclerosisArmin ParavlićNo ratings yet
- Midwifery LedDocument15 pagesMidwifery LedRizka Dita Hidayati100% (1)
- Concept PaperDocument3 pagesConcept Papergladylou siocoNo ratings yet
- Serological Monitoring by ELISADocument3 pagesSerological Monitoring by ELISAreza tavayef100% (1)
- Question and AnswerDocument4 pagesQuestion and AnswerShaf AbubakarNo ratings yet
- SSIPDocument4 pagesSSIPGlenn Clemente100% (2)
- Thomas Foot ReflexologyDocument112 pagesThomas Foot ReflexologySa MiNo ratings yet
- Artificial InseminationDocument3 pagesArtificial Inseminationapi-263932656No ratings yet
- Daily Ward AssignmentsDocument4 pagesDaily Ward AssignmentsMia Labrador Sta CruzNo ratings yet
- Anna Fagin Resume Aug 2014Document1 pageAnna Fagin Resume Aug 2014api-261821160No ratings yet
- Acute Complications of Diabetes MellitusDocument1 pageAcute Complications of Diabetes MellitusGerardLum100% (1)
- Nursing Care Plan for Patient SafetyDocument9 pagesNursing Care Plan for Patient SafetyACOB, Jamil C.No ratings yet
- Pedia ComputationsDocument5 pagesPedia ComputationsRheenz Fornoles100% (1)
- Top 5 Consumer Court CasesDocument7 pagesTop 5 Consumer Court CasesTanishka SoniNo ratings yet
- CPT 2021 guide for identifying medical proceduresDocument7 pagesCPT 2021 guide for identifying medical proceduresChester FernandezNo ratings yet
- Project ProposalDocument16 pagesProject ProposalMashaal FasihNo ratings yet
- Current Affairs Q&A PDF - November 2020 by AffairsCloudDocument214 pagesCurrent Affairs Q&A PDF - November 2020 by AffairsCloudraviNo ratings yet
- Intrathecal MTX & Cytarabine & Hydrocortisone V4 2.15Document2 pagesIntrathecal MTX & Cytarabine & Hydrocortisone V4 2.15GabrielNo ratings yet
- Small-Sided Games and Integrating Physical PreparationDocument196 pagesSmall-Sided Games and Integrating Physical Preparationbolebs1475% (4)
- Training Needs Analysis FormDocument4 pagesTraining Needs Analysis FormLizjasmine DimayaNo ratings yet
- CYBERBULLYINGDocument2 pagesCYBERBULLYINGAdinda CahayaNo ratings yet
- Antiglobulin TestDocument28 pagesAntiglobulin TestAvi Verma100% (1)
- Pesticide ApplicationDocument5 pagesPesticide ApplicationPrashant GurjarNo ratings yet