You might also like
- SS-QOL Stroke Quality of Life ScaleDocument2 pagesSS-QOL Stroke Quality of Life ScaleBayu WirantikaNo ratings yet
- Your Stroke Recovery JourneyDocument6 pagesYour Stroke Recovery JourneyDanielicah CruzNo ratings yet
- Specimen Qlq-c30 EnglishDocument2 pagesSpecimen Qlq-c30 EnglishFenny KusumasariNo ratings yet
- HN43 EnglishDocument2 pagesHN43 EnglishAayush KapoorNo ratings yet
- Answer Key: 1a Consuming PassionsDocument16 pagesAnswer Key: 1a Consuming PassionsCélia ZENNOUCHENo ratings yet
- QLQ-C30 English PDFDocument2 pagesQLQ-C30 English PDFabi nayaNo ratings yet
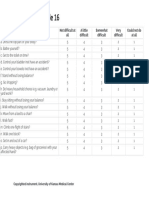
- Stroke Impact Scale 16Document1 pageStroke Impact Scale 16Cona KlaggesNo ratings yet
- Cuestionario FA12Document1 pageCuestionario FA12Julen Cruz QuiñonesNo ratings yet
- sf36 PDFDocument2 pagessf36 PDFinvading_jam7582No ratings yet
- B1+ UNIT 1 Flipped Classroom Video WorksheetDocument1 pageB1+ UNIT 1 Flipped Classroom Video WorksheetXime OlariagaNo ratings yet
- B2 End of Year Test Answer Key StandardDocument2 pagesB2 End of Year Test Answer Key StandardN.A.ÇNo ratings yet
- New LongitudinalDocument2 pagesNew LongitudinalArijit DeyNo ratings yet
- 2.2 Developing The Whole Person HandoutDocument2 pages2.2 Developing The Whole Person HandoutHero Shinichi HamadaNo ratings yet
- Progress Test2 ExtensionDocument5 pagesProgress Test2 ExtensionCarito MoyaNo ratings yet
- PERDEV Big Five Personality Inventory ResponseDocument2 pagesPERDEV Big Five Personality Inventory ResponseClyde Kendrick MachanNo ratings yet
- 50-Item Set of IPIP Big-Five Factor MarkersDocument3 pages50-Item Set of IPIP Big-Five Factor MarkersShawn LimNo ratings yet
- Speaking Skills Practice: Giving Your Opinion - Answers: PreparationDocument1 pageSpeaking Skills Practice: Giving Your Opinion - Answers: PreparationovelNo ratings yet
- Direct and Indirect Questions American English Student Ver2Document3 pagesDirect and Indirect Questions American English Student Ver2Gabrielle ReyesNo ratings yet
- The Big Five Personality Test (BFPT)Document6 pagesThe Big Five Personality Test (BFPT)Maliha NazarNo ratings yet
- Roadmap B2+ SB - AnswersDocument56 pagesRoadmap B2+ SB - AnswersshadowM84% (32)
- Reading + Writing Pre F (Key)Document39 pagesReading + Writing Pre F (Key)Thuy Dung PhunggNo ratings yet
- Keys to Happiness and Life LessonsDocument7 pagesKeys to Happiness and Life LessonsJacqueline SotoNo ratings yet
- The Level of Stress of Stress of Grade 12 Stem Students Experienced in Their Specialized Subjects in Malvar Senior Highschool QuestionaireDocument3 pagesThe Level of Stress of Stress of Grade 12 Stem Students Experienced in Their Specialized Subjects in Malvar Senior Highschool QuestionairePol Vince Bernard SalisiNo ratings yet
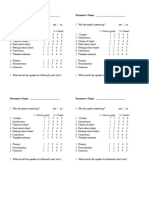
- Presenter's Name: - Presenter's NameDocument2 pagesPresenter's Name: - Presenter's NameJimNo ratings yet
- Harmonize 5 TRM AK Reading AKDocument4 pagesHarmonize 5 TRM AK Reading AKM. Noemí0% (1)
- Gateway 2ed C1 Workbook KeysDocument11 pagesGateway 2ed C1 Workbook KeysValentin Beckeshchenko100% (3)
- Coursebook Voyage B1Document10 pagesCoursebook Voyage B1Paula Arango100% (1)
- 5cuadernillofinal OkDocument31 pages5cuadernillofinal OkBlanca Ivett CasarrubiasNo ratings yet
- #002 - English TestDocument4 pages#002 - English TestGiang NguyễnNo ratings yet
- Self-Care Questionnaire: PHYSICAL WELLBEING-How Often Do YouDocument2 pagesSelf-Care Questionnaire: PHYSICAL WELLBEING-How Often Do YouPrasetya Hadi NugrahaNo ratings yet
- Quiz 5Document4 pagesQuiz 5Mariela Ortiz CepedaNo ratings yet
- SF-36 Website PDF PDFDocument5 pagesSF-36 Website PDF PDFAnonymous orRMyNUG6ENo ratings yet
- Progress Test 11 - Questions, QuestionsDocument2 pagesProgress Test 11 - Questions, Questionsمحمد الرميحNo ratings yet
- 02advantage1 UT2 Test Level2Document2 pages02advantage1 UT2 Test Level2Noelia ColomaNo ratings yet
- Cambridge Exam Practice for Units 1 and 2Document3 pagesCambridge Exam Practice for Units 1 and 2PaskuatorNo ratings yet
- The Big Five Personality Test (BFPT)Document6 pagesThe Big Five Personality Test (BFPT)FatimaNo ratings yet
- The Big Five Personality Test (BFPT)Document6 pagesThe Big Five Personality Test (BFPT)Joyce Aminel EspedidoNo ratings yet
- The Big Five Personality Test (BFPT)Document6 pagesThe Big Five Personality Test (BFPT)Haya AliNo ratings yet
- The Big Five Personality Test (BFPTDocument6 pagesThe Big Five Personality Test (BFPTshivangi unknownNo ratings yet
- The Big Five Personality Test (BFPT)Document6 pagesThe Big Five Personality Test (BFPT)Bagas IndiantoNo ratings yet
- The Big Five Personality Test (BFPTDocument6 pagesThe Big Five Personality Test (BFPTfurqan.malikNo ratings yet
- The Big Five Personality Test (BFPT)Document6 pagesThe Big Five Personality Test (BFPT)Ovidiu MoldovanNo ratings yet
- The Big Five Personality Test (BFPT)Document6 pagesThe Big Five Personality Test (BFPT)Robert PetracheNo ratings yet
- The Big Five Personality Test (BFPT)Document6 pagesThe Big Five Personality Test (BFPT)Muntaha SikandarNo ratings yet
- Teens Upper Intermediate Review 3 British English TeacherDocument12 pagesTeens Upper Intermediate Review 3 British English TeacherIgorNo ratings yet
- Gateway 2ed C1 Workbook KeysDocument11 pagesGateway 2ed C1 Workbook Keys26georgidimovNo ratings yet
- IC3 Upp-Int SB Answer-KeyDocument32 pagesIC3 Upp-Int SB Answer-KeyZitaNo ratings yet
- Phrasal Verbs 1 British English StudentDocument5 pagesPhrasal Verbs 1 British English StudentAline VilelaNo ratings yet
- Phrasal Verbs 1 British English TeacherDocument7 pagesPhrasal Verbs 1 British English TeacherAline VilelaNo ratings yet
- Intensive English 3: Week 4 Online Session 2 Unit 7: ProblemsDocument19 pagesIntensive English 3: Week 4 Online Session 2 Unit 7: ProblemsChrismell ValladaresNo ratings yet
- English 3: Unit 6: Accidents Online Session 1Document13 pagesEnglish 3: Unit 6: Accidents Online Session 1Rafael TrujilloNo ratings yet
- Teens Upper Intermediate Review 3 British English StudentDocument9 pagesTeens Upper Intermediate Review 3 British English StudentMaria Guadalupe Galván EstradaNo ratings yet
- Extra Answer KeyDocument24 pagesExtra Answer KeyDaryna AntonyukNo ratings yet
- Extra Workbook Answer Key: Ing FormDocument24 pagesExtra Workbook Answer Key: Ing FormMaya Collins-CokleyNo ratings yet
- Personal Factors Quality of Life WHOQOL-BREF & DISDocument5 pagesPersonal Factors Quality of Life WHOQOL-BREF & DISCharisse LoboNo ratings yet
- Focus4 2E Unit Test Vocabulary Grammar UoE Unit8 GroupA B ANSWERS PDFDocument1 pageFocus4 2E Unit Test Vocabulary Grammar UoE Unit8 GroupA B ANSWERS PDFКоля РублюкNo ratings yet
- Final Questionnaire. Coping Strategies, Stress and Academic PerformanceDocument4 pagesFinal Questionnaire. Coping Strategies, Stress and Academic PerformanceRonald Tres Reyes100% (1)
- Phrasal Verbs 1 British English Student Ver2Document5 pagesPhrasal Verbs 1 British English Student Ver2Sarah KhalilNo ratings yet
- Elementary Review 5 British English Teacher Ver2Document7 pagesElementary Review 5 British English Teacher Ver2Cristina GhindaNo ratings yet
- PDF Thomason CapstoneDocument10 pagesPDF Thomason CapstoneJohann Sebastian CruzNo ratings yet
- Correia Balance Outcome MeasDocument28 pagesCorreia Balance Outcome MeasJohann Sebastian CruzNo ratings yet
- God's Prayer for Serenity, Courage and WisdomDocument1 pageGod's Prayer for Serenity, Courage and WisdomJohann Sebastian CruzNo ratings yet
- NTG Reviewer '13Document413 pagesNTG Reviewer '13RuiVanNo ratings yet
- Neurologic ExaminationDocument6 pagesNeurologic ExaminationJohann Sebastian CruzNo ratings yet
- Principles of ChartingDocument7 pagesPrinciples of ChartingJohann Sebastian CruzNo ratings yet
- Compression Rubric PDFDocument1 pageCompression Rubric PDFJohann Sebastian CruzNo ratings yet
- 210wk7massage PDFDocument30 pages210wk7massage PDFMileNo ratings yet
- Physical Therapy Modalities PDFDocument31 pagesPhysical Therapy Modalities PDFArjun S RajNo ratings yet
- Pathophysiology of Bacterial Infections Cheat Sheet: by ViaDocument5 pagesPathophysiology of Bacterial Infections Cheat Sheet: by ViaJohann Sebastian CruzNo ratings yet
- SR Iv PDFDocument8 pagesSR Iv PDFJohann Sebastian CruzNo ratings yet
- SR OF CVsDocument16 pagesSR OF CVsJohann Sebastian CruzNo ratings yet
- Fma Ue English PDFDocument3 pagesFma Ue English PDFnistaraNo ratings yet
- Medicine The American Journal of SportsDocument7 pagesMedicine The American Journal of SportsJohann Sebastian CruzNo ratings yet
- PT 1 Midterm RubricDocument3 pagesPT 1 Midterm RubricJohann Sebastian CruzNo ratings yet
- WelcomeDocument5 pagesWelcomeCatNo ratings yet
- RA 7277 - Magna Carta of Disabled PersonsDocument18 pagesRA 7277 - Magna Carta of Disabled PersonsVanny Joyce Baluyut100% (3)
- The Ability of The Landing Error Scoring System To Detect Changes in Landing Mechanics: A Critically Appraised TopicDocument9 pagesThe Ability of The Landing Error Scoring System To Detect Changes in Landing Mechanics: A Critically Appraised TopicJohann Sebastian CruzNo ratings yet
- WelcomeDocument5 pagesWelcomeCatNo ratings yet
- KINESIOLOGY - Carmina Cortez, MD - September 27, 2017Document9 pagesKINESIOLOGY - Carmina Cortez, MD - September 27, 2017Johann Sebastian CruzNo ratings yet
- The Skeletal & Articular SystemsDocument11 pagesThe Skeletal & Articular SystemsJohann Sebastian CruzNo ratings yet
- PT research manual week 1 tasksDocument5 pagesPT research manual week 1 tasksJohann Sebastian CruzNo ratings yet
- Final MD HGD ReportDocument100 pagesFinal MD HGD ReportJohann Sebastian CruzNo ratings yet
- Physical Therapy Ethics - Gabard, Donald L. (SRG)Document210 pagesPhysical Therapy Ethics - Gabard, Donald L. (SRG)Eva Bella93% (15)
- Head and Neck - MusclesDocument3 pagesHead and Neck - MusclesJohann Sebastian CruzNo ratings yet
- Hispanic CultureDocument76 pagesHispanic CultureJohann Sebastian CruzNo ratings yet
- The African American Culture: An OverviewDocument61 pagesThe African American Culture: An OverviewJohann Sebastian CruzNo ratings yet
- Medicine The American Journal of SportsDocument7 pagesMedicine The American Journal of SportsJohann Sebastian CruzNo ratings yet
- Description PDFDocument1 pageDescription PDFJohann Sebastian CruzNo ratings yet
- PariharaDocument2 pagesPariharahrvNo ratings yet
- E-Way BillDocument1 pageE-Way BillShriyans DaftariNo ratings yet
- TQM 2 MARKSDocument12 pagesTQM 2 MARKSMARIYAPPANNo ratings yet
- PEOPLE IN MY TOWN - Song Worksheet PAULA 2019Document2 pagesPEOPLE IN MY TOWN - Song Worksheet PAULA 2019PauNo ratings yet
- 1605 HOBAS Jacking Pipes WebDocument16 pages1605 HOBAS Jacking Pipes Weballouche_abdNo ratings yet
- Tata Steel-MDP SessionDocument69 pagesTata Steel-MDP Sessionsasharma82No ratings yet
- Large Generators WEBDocument16 pagesLarge Generators WEBMaycon MaranNo ratings yet
- AS400 Config Audit Checklist Security BrigadeDocument4 pagesAS400 Config Audit Checklist Security BrigadeAlok DriveqNo ratings yet
- TEFL I Course Prepares Students to Teach EnglishDocument8 pagesTEFL I Course Prepares Students to Teach EnglishErma DomosNo ratings yet
- Gujrat Newspaper IndustryDocument14 pagesGujrat Newspaper IndustryAlok MahajanNo ratings yet
- Unit IV - CPU Scheduling and Algorithm Section 4.1 Scheduling Types Scheduling ObjectivesDocument18 pagesUnit IV - CPU Scheduling and Algorithm Section 4.1 Scheduling Types Scheduling ObjectivessmsaranyaNo ratings yet
- Age Hardening Gold Alloys For JewelryDocument4 pagesAge Hardening Gold Alloys For JewelryReinol Eko SianturiNo ratings yet
- Linkstar RCST Installation Guide: Version DDocument56 pagesLinkstar RCST Installation Guide: Version Djorge_chavez01No ratings yet
- Roof Beam Layout - r1Document1 pageRoof Beam Layout - r1Niraj ShindeNo ratings yet
- WEG Low Voltage Motor Control Center ccm03 50044030 Brochure English PDFDocument12 pagesWEG Low Voltage Motor Control Center ccm03 50044030 Brochure English PDFRitaban222No ratings yet
- First Preliminary Music Video ScriptDocument1 pageFirst Preliminary Music Video Scriptapi-455734096No ratings yet
- Literature Review On Waste Management in NigeriaDocument9 pagesLiterature Review On Waste Management in NigeriajzneaqwgfNo ratings yet
- Max-OT For Dummies - Bodybuilding - Com ForumsDocument21 pagesMax-OT For Dummies - Bodybuilding - Com ForumsPhong QuachNo ratings yet
- Airport Design GuidelinesDocument408 pagesAirport Design Guidelinesnickolololo67% (9)
- Glossary of Permafrost and Ground-Ice IPA 2005Document159 pagesGlossary of Permafrost and Ground-Ice IPA 2005NatitaGonzàlezDíazNo ratings yet
- The Brain from Inside Out Chapter 4 SummaryDocument20 pagesThe Brain from Inside Out Chapter 4 SummaryjuannnnNo ratings yet
- 32 Productivity Increase in A PeirceSmith Convert 153013Document14 pages32 Productivity Increase in A PeirceSmith Convert 153013amirlpNo ratings yet
- Business PolicyDocument17 pagesBusiness PolicyManish SinghNo ratings yet
- Regional Campus The English and Foreign Languages UniversityDocument2 pagesRegional Campus The English and Foreign Languages UniversitySidra KhanNo ratings yet
- Contoh Skripsi Bahasa Inggris Case StudyDocument18 pagesContoh Skripsi Bahasa Inggris Case StudyRizki Fajrita100% (14)
- Pradeep Kumaresan Resume - Software Testing ExperienceDocument3 pagesPradeep Kumaresan Resume - Software Testing ExperienceSANTANo ratings yet
- 01 - Narmada M PhilDocument200 pages01 - Narmada M PhilafaceanNo ratings yet
- CN Assignment 1 COE-540Document5 pagesCN Assignment 1 COE-540Ghazanfar LatifNo ratings yet
- Duane Grant, A099 743 627 (BIA Sept. 9, 2016)Document12 pagesDuane Grant, A099 743 627 (BIA Sept. 9, 2016)Immigrant & Refugee Appellate Center, LLCNo ratings yet
- BISE Sukkur HSC Part 2 Results 2015Document12 pagesBISE Sukkur HSC Part 2 Results 2015ajayNo ratings yet