You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- MODULE 6 Dissociative DisorderDocument8 pagesMODULE 6 Dissociative DisorderDaphneNo ratings yet
- Sitz Bath Procedure ChecklistDocument4 pagesSitz Bath Procedure ChecklistGeno Adrian T Pampanga100% (1)
- Icrobiology Human Immunodeficiency Virus AND Infectious DiseasesDocument13 pagesIcrobiology Human Immunodeficiency Virus AND Infectious DiseasesAvineet MalhotraNo ratings yet
- Kabir PathologyDocument6 pagesKabir PathologyHumayan KabirNo ratings yet
- NLEP-Bsc NSG pt-IVDocument6 pagesNLEP-Bsc NSG pt-IVSree LathaNo ratings yet
- The Miracle Meal - David OyedepoDocument25 pagesThe Miracle Meal - David OyedepoChukwuma LystanNo ratings yet
- Files 2Document18 pagesFiles 2shafeeque TNo ratings yet
- A Cardiomyopathy PPT NEWDocument62 pagesA Cardiomyopathy PPT NEWShetal Sharma100% (1)
- Cardiac Poison: DR Bibek Raj ParajuliDocument23 pagesCardiac Poison: DR Bibek Raj Parajuliranjithreddy916gmailNo ratings yet
- WES WGS Brochure Pages V2.1eng Web 20201019Document16 pagesWES WGS Brochure Pages V2.1eng Web 20201019drumerNo ratings yet
- Hypercalcitoninaemia in Pseudohypo-ParathyroidismDocument5 pagesHypercalcitoninaemia in Pseudohypo-Parathyroidismradu nicolaeNo ratings yet
- Research Paper On LiverDocument4 pagesResearch Paper On Liverhyzypif0gif3100% (1)
- A Comprehensive Review On Human Nail: International Journal of Medical and Health ResearchDocument3 pagesA Comprehensive Review On Human Nail: International Journal of Medical and Health ResearchEmaNo ratings yet
- Case Study On Children With Cardiac DisordersDocument3 pagesCase Study On Children With Cardiac DisordersAlyNo ratings yet
- Question Bank PT-II SET 02 Question Paper 2021Document20 pagesQuestion Bank PT-II SET 02 Question Paper 2021xyzNo ratings yet
- STUDY GUIDE 2 (Operaña, Ellayza)Document4 pagesSTUDY GUIDE 2 (Operaña, Ellayza)OPERAñA ELLAYZA RB DECANONo ratings yet
- PACK Ethiopia Training PresentationDocument10 pagesPACK Ethiopia Training PresentationAbebe TilahunNo ratings yet
- Teaching Neuroimage: A 41-Year-Old Woman Presented With Excessive Sweating of Contralateral Face and ExtremityDocument3 pagesTeaching Neuroimage: A 41-Year-Old Woman Presented With Excessive Sweating of Contralateral Face and ExtremityAndrei BicanNo ratings yet
- Anxiolytics and AntidepressantsDocument271 pagesAnxiolytics and AntidepressantsAmir PeljtoNo ratings yet
- Cases in PsychiatryDocument46 pagesCases in PsychiatryFatema TahaNo ratings yet
- Open Letter From The Mayors of Northeast TennesseeDocument1 pageOpen Letter From The Mayors of Northeast TennesseeNews 5 WCYBNo ratings yet
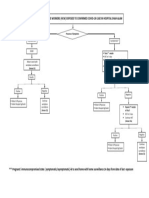
- Management of Healthcare Workers (HCW) Exposed To Confirmed Covid-19 Case in Hospital Shah AlamDocument1 pageManagement of Healthcare Workers (HCW) Exposed To Confirmed Covid-19 Case in Hospital Shah AlamNurhafizah IbrahimNo ratings yet
- 10 1016@j Det 2018 05 008Document8 pages10 1016@j Det 2018 05 008Renata GoulartNo ratings yet
- Catalogue 30Document199 pagesCatalogue 30thanh ba matNo ratings yet
- Risk Management WEEK 3Document11 pagesRisk Management WEEK 3Ralph Theodore QuintanaNo ratings yet
- I. Health, Wellness and Illness: Self-Esteem Love and Belongingness Self-ActualizationDocument3 pagesI. Health, Wellness and Illness: Self-Esteem Love and Belongingness Self-ActualizationYmon TuallaNo ratings yet
- Study - Scientifically Innovative Solution To Reducing Coronavirus Transmission (Shahid-Nasir July 2020)Document14 pagesStudy - Scientifically Innovative Solution To Reducing Coronavirus Transmission (Shahid-Nasir July 2020)Fatima ShahidNo ratings yet
- Headache: Migraine and Tension-Type HeadacheDocument12 pagesHeadache: Migraine and Tension-Type HeadacheLoren SangalangNo ratings yet
- Health Screening Questionnaire Ver 1.1 - Ooi Wei ShengDocument2 pagesHealth Screening Questionnaire Ver 1.1 - Ooi Wei ShengTerry wei shengNo ratings yet
- Related Studies AyeeeDocument6 pagesRelated Studies AyeeeNoelle CaballeraNo ratings yet