You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Adult Carer Quality of Life Questionnaire (AC-QoL)Document14 pagesAdult Carer Quality of Life Questionnaire (AC-QoL)Andi SusiloNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Seven Senses Chakra GuideDocument11 pagesSeven Senses Chakra GuidemhliuNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- First Episode Psychosis GuideDocument38 pagesFirst Episode Psychosis Guide'Josh G MwanikiNo ratings yet
- 2021 Va Ers DataDocument1,788 pages2021 Va Ers DataasdasdasdNo ratings yet
- Hodgkin LymphomaDocument32 pagesHodgkin LymphomaAndi SusiloNo ratings yet
- Learners With Chronic IllnessDocument22 pagesLearners With Chronic IllnessERICAMILES BARRIENTOS0% (1)
- Glucagon-Like Peptide 1 Receptor (GLP-1R) Expression by Nerve Fibres in Inflammatory Bowel Disease and Functional Effects in Cultured NeuronsDocument18 pagesGlucagon-Like Peptide 1 Receptor (GLP-1R) Expression by Nerve Fibres in Inflammatory Bowel Disease and Functional Effects in Cultured NeuronsAndi SusiloNo ratings yet
- Cirrhotic Cardiomyopathy HepatoDocument10 pagesCirrhotic Cardiomyopathy HepatoAndi SusiloNo ratings yet
- What Is Hyperthyroidism?Document12 pagesWhat Is Hyperthyroidism?Andi SusiloNo ratings yet
- In Vitro Antiviral Activity of Echinaforce® For COVID19Document14 pagesIn Vitro Antiviral Activity of Echinaforce® For COVID19Andi SusiloNo ratings yet
- Oa RaDocument16 pagesOa RaAndi SusiloNo ratings yet
- 1414 431X BJMBR 52 2 E7809 PDFDocument9 pages1414 431X BJMBR 52 2 E7809 PDFNaomi RamosNo ratings yet
- Vaksin Influenza COVID MortalityDocument17 pagesVaksin Influenza COVID MortalityAndi SusiloNo ratings yet
- Radiation Matters of The HeartDocument13 pagesRadiation Matters of The HeartAndi SusiloNo ratings yet
- Ada PDFDocument204 pagesAda PDFMario BarbozaNo ratings yet
- Radiation Matters of The HeartDocument13 pagesRadiation Matters of The HeartAndi SusiloNo ratings yet
- 1414 431X BJMBR 52 2 E7809 PDFDocument9 pages1414 431X BJMBR 52 2 E7809 PDFNaomi RamosNo ratings yet
- Laporan Pasien Baru Ruangan R2 Irdm Rsup Prof Dr. R. D. Kandou ManadoDocument2 pagesLaporan Pasien Baru Ruangan R2 Irdm Rsup Prof Dr. R. D. Kandou ManadoAndi SusiloNo ratings yet
- Management Lymphoma 2018 Indian Expert GroupDocument24 pagesManagement Lymphoma 2018 Indian Expert GroupAndi SusiloNo ratings yet
- Glucagon-Like Peptide 1 Receptor (GLP-1R) Expression by Nerve Fibres in Inflammatory Bowel Disease and Functional Effects in Cultured NeuronsDocument18 pagesGlucagon-Like Peptide 1 Receptor (GLP-1R) Expression by Nerve Fibres in Inflammatory Bowel Disease and Functional Effects in Cultured NeuronsAndi SusiloNo ratings yet
- Ibd GDDocument15 pagesIbd GDAndi SusiloNo ratings yet
- IBD GLP1R RelationDocument18 pagesIBD GLP1R RelationAndi SusiloNo ratings yet
- Oa RaDocument16 pagesOa RaAndi SusiloNo ratings yet
- Oa RaDocument16 pagesOa RaAndi SusiloNo ratings yet
- Abstract Profile of IgE Total in Chronic Kidney Disease PatientDocument1 pageAbstract Profile of IgE Total in Chronic Kidney Disease PatientAndi SusiloNo ratings yet
- Kakoullis 2019Document20 pagesKakoullis 2019Andi SusiloNo ratings yet
- Shiga E ColiDocument34 pagesShiga E ColiAndi SusiloNo ratings yet
- Ibd GLP1Document19 pagesIbd GLP1Andi SusiloNo ratings yet
- Jurnal Kardio3Document8 pagesJurnal Kardio3Andi SusiloNo ratings yet
- 5308635Document10 pages5308635LuluNo ratings yet
- Menopause in CKDDocument10 pagesMenopause in CKDAndi SusiloNo ratings yet
- Abstract Profile of IgE Total in Chronic Kidney Disease PatientDocument1 pageAbstract Profile of IgE Total in Chronic Kidney Disease PatientAndi SusiloNo ratings yet
- Penelitian IgE CKDDocument4 pagesPenelitian IgE CKDAndi SusiloNo ratings yet
- MCQ FinalDocument6 pagesMCQ FinalJerin XavierNo ratings yet
- A Twilight Sector Adventure: by Filamena YoungDocument24 pagesA Twilight Sector Adventure: by Filamena YoungKai927No ratings yet
- Sciencedirect: Thalassemia Major May Decrease The Frequency of Febrile Convulsions in ChildrenDocument4 pagesSciencedirect: Thalassemia Major May Decrease The Frequency of Febrile Convulsions in ChildrenZherlynPoetriBungzuNo ratings yet
- Life Is A Continous Process of AdjustmentDocument78 pagesLife Is A Continous Process of AdjustmentGulmoharNo ratings yet
- The Art of Surgery: The Strange World of The Placebo ResponseDocument4 pagesThe Art of Surgery: The Strange World of The Placebo ResponseTamsin Athalie NicholsonNo ratings yet
- BSNDocument5 pagesBSNNoriel GirayNo ratings yet
- Medical and Surgical Nursing - IIDocument2 pagesMedical and Surgical Nursing - IIYAMINIPRIYANNo ratings yet
- Housing Needs and Home Management Practi PDFDocument25 pagesHousing Needs and Home Management Practi PDFian_herbasNo ratings yet
- Management of Menopause - A View Towards Prevention (Lobo y Gompel, 2022)Document14 pagesManagement of Menopause - A View Towards Prevention (Lobo y Gompel, 2022)Susana RoyNo ratings yet
- PDFDocument12 pagesPDFGalih Miftah SgkNo ratings yet
- MODULE 6 Sir RobertDocument17 pagesMODULE 6 Sir RobertManilyn DominguezNo ratings yet
- Pulmonary Interventions-Page 1504: 1. Give at Least 3 Pulmonary Interventions For Cystic Fibrosis?Document3 pagesPulmonary Interventions-Page 1504: 1. Give at Least 3 Pulmonary Interventions For Cystic Fibrosis?ADOLF FRUELAN HIDALGONo ratings yet
- BM Notes SeniorDocument393 pagesBM Notes SeniorShreya KishorNo ratings yet
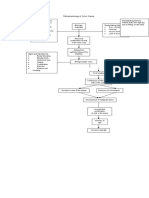
- Pathophysiology of Colon Cancer Predisposing Factors: Etiology: Precipitating Factors: Precipitating FactorsDocument1 pagePathophysiology of Colon Cancer Predisposing Factors: Etiology: Precipitating Factors: Precipitating FactorstatiNo ratings yet
- Galangal Root: Benefits, Uses, and Side EffectsDocument25 pagesGalangal Root: Benefits, Uses, and Side EffectsEstela BenegildoNo ratings yet
- San Jiao Chap 12Document3 pagesSan Jiao Chap 12Bolt VoNo ratings yet
- Common River Medicinal Plant Handbook FINAL4Document40 pagesCommon River Medicinal Plant Handbook FINAL4Shime EthiopianNo ratings yet
- ESSAYDocument2 pagesESSAYBokNo ratings yet
- LithiumDocument2 pagesLithiumdiet.nurseNo ratings yet
- Done - EDITED-HOPE1 - q1 - Mod5 - ObservesPersonalSafetyProtocolDocument21 pagesDone - EDITED-HOPE1 - q1 - Mod5 - ObservesPersonalSafetyProtocolVivencio Pascual JrNo ratings yet
- SGOT (Aspartate Aminotransferase, AST, Glutamic Oxaloacetic Transaminase)Document9 pagesSGOT (Aspartate Aminotransferase, AST, Glutamic Oxaloacetic Transaminase)Reman A. AlingasaNo ratings yet
- Sciencedirect: 2 World Conference On Business, Economics and Management - Wcbem2013Document5 pagesSciencedirect: 2 World Conference On Business, Economics and Management - Wcbem2013claaa_fhrNo ratings yet
- Brain Mechanisms in Manic DepressionDocument6 pagesBrain Mechanisms in Manic DepressionCharpapathNo ratings yet
- Hannover Polytrauma Score.4Document2 pagesHannover Polytrauma Score.4Azmi FarhadiNo ratings yet
- Safety Profile of Rotavac: Observational Prospective StudyDocument7 pagesSafety Profile of Rotavac: Observational Prospective StudyMalook Sekhon100% (1)
- Autism FinalesDocument228 pagesAutism Finaleselidabicaku9254No ratings yet