You might also like
- Life Span Development Seventeenth Edition John W Santrock Full ChapterDocument67 pagesLife Span Development Seventeenth Edition John W Santrock Full Chapterjohn.miller787100% (8)
- Ella Enchanted ScriptDocument17 pagesElla Enchanted ScriptAccio Mora67% (3)
- ICU RN Report SheetDocument2 pagesICU RN Report SheetKatie Hecker100% (1)
- Medsurg Report SheetDocument1 pageMedsurg Report Sheetjjuplifter100% (3)
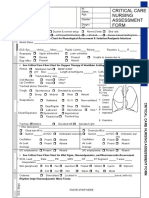
- Idoc - Pub - Critical Care Nursing Assessment FormDocument3 pagesIdoc - Pub - Critical Care Nursing Assessment FormNamra AnsariNo ratings yet
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsFrom EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsNo ratings yet
- Critical Care Nursing Assessment Form: R R R R R R R RDocument2 pagesCritical Care Nursing Assessment Form: R R R R R R R RPipit Permata100% (1)
- Marty's Report FormDocument1 pageMarty's Report FormmartydailyNo ratings yet
- 1 Patient Brain SheetDocument2 pages1 Patient Brain SheetcutevivesNo ratings yet
- SBARDocument1 pageSBARdrewstewNo ratings yet
- Central Line Cheat SheetDocument1 pageCentral Line Cheat SheetLara Mae100% (1)
- Telemetry-Intermediate Care Skills ChecklistDocument4 pagesTelemetry-Intermediate Care Skills ChecklistnorthweststaffingNo ratings yet
- Nursing Clinical Prep SheetDocument1 pageNursing Clinical Prep SheetPatty Pasarilla PassehlNo ratings yet
- Icusheet - Anotherone 4Document1 pageIcusheet - Anotherone 4queenzkNo ratings yet
- Zero Based BudgetDocument9 pagesZero Based Budgetapi-447860598No ratings yet
- Case Study On Piaget's Cognitive DevelopmentDocument11 pagesCase Study On Piaget's Cognitive DevelopmentJuvié BanaganNo ratings yet
- Nursing Brain - JGDocument2 pagesNursing Brain - JGapi-280874783No ratings yet
- Med Surg Report Sheet Night Shift FINALDocument2 pagesMed Surg Report Sheet Night Shift FINALCindy AnnNo ratings yet
- BrainSheet 2patient v3Document1 pageBrainSheet 2patient v3Shelly BassNo ratings yet
- DPN Icu PDFDocument1 pageDPN Icu PDFharoonNo ratings yet
- Kardex NotesDocument1 pageKardex NotesmarlenegableNo ratings yet
- Med Surg Report Sheet Night Shift FINAL2Document2 pagesMed Surg Report Sheet Night Shift FINAL2Cindy Ann100% (1)
- Brainsheet f04Document2 pagesBrainsheet f04mrsfelic08No ratings yet
- Physical Assessment FormDocument5 pagesPhysical Assessment FormJo MaldonadoNo ratings yet
- RM# Name: RM# Name: Age: Doctor/Consults: Age: Doctor/ConsultsDocument2 pagesRM# Name: RM# Name: Age: Doctor/Consults: Age: Doctor/Consultsseaturtles505No ratings yet
- ACLS Algorithms (2011)Document6 pagesACLS Algorithms (2011)senbonsakuraNo ratings yet
- Clinical KardexDocument2 pagesClinical KardexJackie Frey100% (2)
- IDCAP Clinical Assessment ToolsDocument4 pagesIDCAP Clinical Assessment ToolsIDCAP2011100% (1)
- Nursing SheetDocument1 pageNursing Sheetseaturtles505100% (1)
- Ccu Survival GuideDocument10 pagesCcu Survival Guideomegasauron0gmailcom100% (1)
- Soap TemplateDocument3 pagesSoap TemplaterohitNo ratings yet
- Clinical Organization Sheet NursingDocument1 pageClinical Organization Sheet NursingSarah S100% (1)
- Isolation:: Orders To Flush Central/hep Loc line/PICCDocument1 pageIsolation:: Orders To Flush Central/hep Loc line/PICCmmaturNo ratings yet
- DATE: - / - / - SUBJECT ID:: Washington University School of Medicine (Principal Investigator)Document3 pagesDATE: - / - / - SUBJECT ID:: Washington University School of Medicine (Principal Investigator)HariprasathNo ratings yet
- Vital Sign Measurements (Standard) : Subject Initials Subject ID Exam DateDocument1 pageVital Sign Measurements (Standard) : Subject Initials Subject ID Exam DatekevindjuandaNo ratings yet
- Nurses Report SheetDocument1 pageNurses Report Sheetnanahikmat lawalNo ratings yet
- Nurse Report SheetDocument1 pageNurse Report SheetTassos KolliasNo ratings yet
- Cardiac Study Guide PDFDocument11 pagesCardiac Study Guide PDF281175100% (1)
- Patient Sticker Patient Sticker: AM LabsDocument3 pagesPatient Sticker Patient Sticker: AM LabsNurse BettyNo ratings yet
- Neonatal Assessmnt Tool PDFDocument2 pagesNeonatal Assessmnt Tool PDFYestin Reece Corpus ArcegaNo ratings yet
- Emergency Nursing 118 LECDocument11 pagesEmergency Nursing 118 LECboxed juiceNo ratings yet
- Code Blue EvaluationDocument1 pageCode Blue EvaluationJessica Garlets0% (1)
- Diagnosis Past Medical History: WBC MicroDocument2 pagesDiagnosis Past Medical History: WBC MicroNicole NewlandNo ratings yet
- 2018-04-09 Pediatric Emergency Nursing Assessment Record FormDocument2 pages2018-04-09 Pediatric Emergency Nursing Assessment Record FormHengkyNo ratings yet
- Brain 1Document1 pageBrain 1Nurse BettyNo ratings yet
- New Icu SheetDocument3 pagesNew Icu SheetJan MarcusNo ratings yet
- Clinical Nursing SheetDocument2 pagesClinical Nursing Sheetnicole eduNo ratings yet
- Necrotizing Otitis 2022Document20 pagesNecrotizing Otitis 2022asmashNo ratings yet
- My Brain SheetDocument2 pagesMy Brain Sheetkellyae100% (1)
- Nursing Day Plan - ExcelDocument1 pageNursing Day Plan - ExceltennyrbNo ratings yet
- Patient A KARDEX 1Document2 pagesPatient A KARDEX 1Franz Patrick Legria, CPAC - SNNo ratings yet
- LDRP Report SheetDocument2 pagesLDRP Report SheetAngela Carrillo TrianoNo ratings yet
- IV TherapyDocument65 pagesIV TherapySarah Uy CaronanNo ratings yet
- ICU Progress NoteDocument7 pagesICU Progress NoteDiana Hylton100% (1)
- Downtime Daily Nursing Assessment & Care Plan: 1 of 5 Date: TimeDocument5 pagesDowntime Daily Nursing Assessment & Care Plan: 1 of 5 Date: TimerupaliNo ratings yet
- New Shift Report Sheet 2008Document1 pageNew Shift Report Sheet 2008cutevivesNo ratings yet
- Electrocardiography: Dr. Anand PatelDocument155 pagesElectrocardiography: Dr. Anand PatelDeepika PatelNo ratings yet
- Emergency Nurse Protocol Back PainDocument2 pagesEmergency Nurse Protocol Back PainSimon S. KledenNo ratings yet
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNo ratings yet
- EKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!From EverandEKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!No ratings yet
- Pain Assessment: Glendale Careeer College ADN ProgramDocument1 pagePain Assessment: Glendale Careeer College ADN ProgramLoraNo ratings yet
- Assessment Planning and Implementation EvaluationDocument2 pagesAssessment Planning and Implementation EvaluationLoraNo ratings yet
- Systems Assessment: SensationDocument2 pagesSystems Assessment: SensationLoraNo ratings yet
- Glendale Career College, ADN Lab Information SheetDocument4 pagesGlendale Career College, ADN Lab Information SheetLoraNo ratings yet
- Weekly Plan of Care 2019Document3 pagesWeekly Plan of Care 2019LoraNo ratings yet
- (Daily Total Points-9 Points Possible) : Clinical Performance Evaluation RecordDocument4 pages(Daily Total Points-9 Points Possible) : Clinical Performance Evaluation RecordLoraNo ratings yet
- The Nurses Role in Regulating The Neonates Temperature Lora F. Aquino Loma Linda University School of NursingDocument2 pagesThe Nurses Role in Regulating The Neonates Temperature Lora F. Aquino Loma Linda University School of NursingLoraNo ratings yet
- Glendale Career College-San Diego Campus Clinical Performance Evaluation Record NU119 Medical Surgical Nursing I - Lab Skills Student Name: FacultyDocument1 pageGlendale Career College-San Diego Campus Clinical Performance Evaluation Record NU119 Medical Surgical Nursing I - Lab Skills Student Name: FacultyLoraNo ratings yet
- Planning Phase Implementation Phase Rationale Evaluation PhaseDocument2 pagesPlanning Phase Implementation Phase Rationale Evaluation PhaseLora0% (1)
- Nursing Care Plan Ineffective ThermoregulationDocument2 pagesNursing Care Plan Ineffective ThermoregulationLoraNo ratings yet
- The Nurses Role in Thermoregulation Lora F. Aquino Loma Linda University School of NursingDocument7 pagesThe Nurses Role in Thermoregulation Lora F. Aquino Loma Linda University School of NursingLoraNo ratings yet
- Quarter 2 MODULE 4B Distinguish Various Types of Informational or Factual Text PDFDocument18 pagesQuarter 2 MODULE 4B Distinguish Various Types of Informational or Factual Text PDFSheril BabaranNo ratings yet
- 1MD 23-24 Course CoordpdfDocument1 page1MD 23-24 Course CoordpdfNiga BallsNo ratings yet
- An Analysis On Pepsico Inc.Document7 pagesAn Analysis On Pepsico Inc.mohidul islamNo ratings yet
- 3-Thomas - Orpas Icru Report 95Document28 pages3-Thomas - Orpas Icru Report 95Alexandru HUSTUCNo ratings yet
- Presidential Decree 603 - The Child and Youth Welfare CodeDocument31 pagesPresidential Decree 603 - The Child and Youth Welfare Codeaynguinomla100% (3)
- Design of Liquid Nitrogen (Ln2) Cryogenic TankDocument19 pagesDesign of Liquid Nitrogen (Ln2) Cryogenic Tankraviteja tankalaNo ratings yet
- CONGRESO MUNDIAL ENSILAJES5July2012Document526 pagesCONGRESO MUNDIAL ENSILAJES5July2012Dayana Camargo GarcìaNo ratings yet
- Heft 6B. Evetts (1892) - Inscriptions of The Reigns of Evi - Merodach (562-559), Neriglissar (559-555) and LaborosoarchodDocument136 pagesHeft 6B. Evetts (1892) - Inscriptions of The Reigns of Evi - Merodach (562-559), Neriglissar (559-555) and LaborosoarchodVlad StanguNo ratings yet
- Case Study 6 - J&J and Dow CorningDocument3 pagesCase Study 6 - J&J and Dow CorningAmanie OthmanNo ratings yet
- LCD Nye EditDocument1 pageLCD Nye EditKevin ParkerNo ratings yet
- Angga Pratama Haloho - 2003511035 - Abstract Assigment - Class ADocument3 pagesAngga Pratama Haloho - 2003511035 - Abstract Assigment - Class AChristmas14 ManjorangFMIPANo ratings yet
- Environmental Science: PaperDocument8 pagesEnvironmental Science: Paperbelqis ratuNo ratings yet
- New Wordpad DocumentDocument2 pagesNew Wordpad Documentspecial_boy_andreyNo ratings yet
- Neurotransmitter Cell CommunicationDocument25 pagesNeurotransmitter Cell CommunicationOtnil DNo ratings yet
- Ent SignsDocument10 pagesEnt SignsPrasun Sit SharmaNo ratings yet
- Variador MitsubishiDocument410 pagesVariador Mitsubishiasdrubal martinezNo ratings yet
- A Bibliography of The History of Child ADocument219 pagesA Bibliography of The History of Child AKonstantinos Mantas100% (2)
- Analysis and Prevention of Bearing FailuresDocument76 pagesAnalysis and Prevention of Bearing Failurestahazeeshan100% (1)
- Limited Powers of Attorney - Motion For Terminating Sanctions (Fraud Upon The Court)Document6 pagesLimited Powers of Attorney - Motion For Terminating Sanctions (Fraud Upon The Court)Odzer ChenmaNo ratings yet
- Product Line Sheet: Liquid Coatings Petrolatum Tapes & Protective OuterwrapsDocument3 pagesProduct Line Sheet: Liquid Coatings Petrolatum Tapes & Protective OuterwrapsIm ChinithNo ratings yet
- Đề Thi Giữa Học Kì 2 Tiếng Anh Lớp 7Document20 pagesĐề Thi Giữa Học Kì 2 Tiếng Anh Lớp 7Hạ VũNo ratings yet
- Soal Cloze Test Explanation - Global WarmingDocument2 pagesSoal Cloze Test Explanation - Global WarmingPanci SeSbs d'NightflierNo ratings yet
- University of Saint Louis Tuguegarao Tuguegarao CityDocument18 pagesUniversity of Saint Louis Tuguegarao Tuguegarao CityJaime TuguicNo ratings yet
- Lab en Autoclave Tuttnauer 05 11 17 - 0Document12 pagesLab en Autoclave Tuttnauer 05 11 17 - 0rachmonaaNo ratings yet
- Low Temperature RefrigerationDocument9 pagesLow Temperature Refrigerationguadalupe_cortes_21100% (2)
- 2 Stroke Engine Runs On Half ChokeDocument3 pages2 Stroke Engine Runs On Half ChokeWINNIE WAMBUI100% (1)
- Activity 1: Enzymes Source Substrate Product ActivityDocument2 pagesActivity 1: Enzymes Source Substrate Product ActivityMAEGAN MADRONIONo ratings yet