You might also like
- Public Health and Primary Care Skills Log BookDocument471 pagesPublic Health and Primary Care Skills Log BookMRS CHAKRAPANI92% (13)
- CHN Lessonplan (NRHM - National Rural Health Mission)Document23 pagesCHN Lessonplan (NRHM - National Rural Health Mission)Samjhana Neupane100% (5)
- Seminar On Skilled Birth SBA ModuleDocument50 pagesSeminar On Skilled Birth SBA ModuleSangita Patir83% (40)
- CHC VisitDocument48 pagesCHC VisitRamyasree BadeNo ratings yet
- WHO & UNICEF: A Brief OverviewDocument46 pagesWHO & UNICEF: A Brief OverviewA J Fathima100% (1)
- Lesson Plan On Wound CareDocument5 pagesLesson Plan On Wound CareA J Fathima0% (1)
- Procedure - Photo TherapyDocument4 pagesProcedure - Photo TherapyMaysa Ismail88% (8)
- Lesson Plan On Wound CareDocument5 pagesLesson Plan On Wound CareA J Fathima0% (1)
- Chapter 2 General Conditions of ServiceDocument7 pagesChapter 2 General Conditions of ServiceAnand KrishnaNo ratings yet
- The End of Poverty - Jaffrey SachsDocument32 pagesThe End of Poverty - Jaffrey SachsPulkit GargNo ratings yet
- National Family Welfare ProgramDocument27 pagesNational Family Welfare ProgramBhawna JoshiNo ratings yet
- Obg-Assignment On Family Welfare ServicesDocument20 pagesObg-Assignment On Family Welfare ServicesRashmi C S71% (7)
- National Health and Family Welfare ProgrammesDocument17 pagesNational Health and Family Welfare ProgrammesSandhya s67% (3)
- National Family Welfare ProgrammeDocument64 pagesNational Family Welfare ProgrammeNityananda Pattanaik67% (3)
- Reproductive and Child Health ProgramDocument42 pagesReproductive and Child Health ProgramNeethu VincentNo ratings yet
- National Health Programme Related To CHNDocument76 pagesNational Health Programme Related To CHNArchanaNo ratings yet
- Family Welfare ProgramDocument20 pagesFamily Welfare ProgramKinjal Vasava0% (1)
- MCH ProgrammeDocument14 pagesMCH ProgrammepriyankaNo ratings yet
- 04 HEALTH CARE DELIVERY SYSTEM INDIA For CHODocument34 pages04 HEALTH CARE DELIVERY SYSTEM INDIA For CHOKailash Nagar100% (1)
- AnemiaDocument16 pagesAnemiaKrishnaveni MurugeshNo ratings yet
- Family Welfare Programme in IndiaDocument25 pagesFamily Welfare Programme in IndiaTirumalesha DadigeNo ratings yet
- Strengthening healthcare through innovative Mother and Child Tracking SystemDocument42 pagesStrengthening healthcare through innovative Mother and Child Tracking SystemAnand gowdaNo ratings yet
- Esi Scheme and CGHS: Mrs. Namita Batra Guin Associate Professor Deptt. of Community Health NursingDocument19 pagesEsi Scheme and CGHS: Mrs. Namita Batra Guin Associate Professor Deptt. of Community Health NursinglivelinamiNo ratings yet
- Family Welfare ProgrammeDocument19 pagesFamily Welfare ProgrammeMahesh Sahu100% (2)
- National Health and Family Welfare Programme: India's Centrally Sponsored ProgramDocument2 pagesNational Health and Family Welfare Programme: India's Centrally Sponsored ProgramSree Latha100% (1)
- Hind Kusht Nivaran SanghDocument2 pagesHind Kusht Nivaran SanghfgvhjbvftyhnhNo ratings yet
- Small Family NormDocument10 pagesSmall Family NormPriya Sharma100% (5)
- Mission Indradhanush: Submitted By-Jayesh Agrawal Mba-Rural Development Semester-IstDocument20 pagesMission Indradhanush: Submitted By-Jayesh Agrawal Mba-Rural Development Semester-IstJayeshAgrawalNo ratings yet
- Reproductive and Child Health ProgrammeDocument37 pagesReproductive and Child Health ProgrammeVeena JV100% (2)
- Reproductive and Child Health ProgrammeDocument14 pagesReproductive and Child Health ProgrammeDr Siddharth DarjiNo ratings yet
- Training rural health workersDocument23 pagesTraining rural health workersBabita DhruwNo ratings yet
- UNIT-II - Health Organization at Village Level, Disctrict Level, State and Central Level - AnandDocument62 pagesUNIT-II - Health Organization at Village Level, Disctrict Level, State and Central Level - AnandAnand gowda100% (3)
- Unit 5 PPP CHN NDocument312 pagesUnit 5 PPP CHN NAnonymous hYMWbA100% (1)
- Filaria - Final 4Document14 pagesFilaria - Final 4Arun Jv100% (1)
- Revised National Tuberculosis Control Programme (RNTCP) Milestones and AchievementsDocument24 pagesRevised National Tuberculosis Control Programme (RNTCP) Milestones and Achievementsarunjv1234100% (1)
- Guidelines for ANMs and LHVs on Ante-natal Care and Skilled Birth AttendanceDocument80 pagesGuidelines for ANMs and LHVs on Ante-natal Care and Skilled Birth AttendanceTmanoj Praveen33% (3)
- Indian Red Cross Society: Providing humanitarian aid in IndiaDocument7 pagesIndian Red Cross Society: Providing humanitarian aid in IndiavndhilmechNo ratings yet
- Problem Statements PresentationDocument7 pagesProblem Statements PresentationAaliyaan KhanNo ratings yet
- Micro Birth PlanningDocument6 pagesMicro Birth Planningkajal thakur100% (2)
- CHN ApproachesDocument9 pagesCHN ApproachesMamta Rajput50% (2)
- Nurses Key Role in Implementing India's National Rural Health MissionDocument32 pagesNurses Key Role in Implementing India's National Rural Health MissionPabhat KumarNo ratings yet
- Small Family NormDocument21 pagesSmall Family NormKailash NagarNo ratings yet
- Elderly Primigravida, Adolescent Pregnancy, Grand MultiparaDocument3 pagesElderly Primigravida, Adolescent Pregnancy, Grand MultiparamercyNo ratings yet
- Gynecological disorders in pregnancy: A reviewDocument34 pagesGynecological disorders in pregnancy: A reviewsanthiyasandy100% (4)
- AYUSHMAN BHARAT - Lec 7th SemDocument61 pagesAYUSHMAN BHARAT - Lec 7th SempriyankaNo ratings yet
- Postnatal Care: Preventing Maternal DeathDocument26 pagesPostnatal Care: Preventing Maternal DeathShivani Shah100% (1)
- Sector wise healthcare delivery in India overviewDocument131 pagesSector wise healthcare delivery in India overviewAnand gowda100% (2)
- National Aids Control ProgrammeDocument25 pagesNational Aids Control ProgrammeSanket TelangNo ratings yet
- Yenepoya Nursing College Safe Childbirth ChecklistDocument16 pagesYenepoya Nursing College Safe Childbirth ChecklistAnand gowdaNo ratings yet
- Border District Cluster StrategyDocument2 pagesBorder District Cluster StrategyRAJU100% (1)
- Health SchemesDocument21 pagesHealth SchemesPankaj Khatri100% (1)
- Seminar On Organization of Camps and Clinics in Community SettingsDocument18 pagesSeminar On Organization of Camps and Clinics in Community SettingsRethina Bai C100% (2)
- CHN Job DescriptionDocument32 pagesCHN Job DescriptionsunielgowdaNo ratings yet
- Presentation ON Health Committee: Submitted To: Mrs. Krishnaveni M.SC (NSG) (Lecturar)Document16 pagesPresentation ON Health Committee: Submitted To: Mrs. Krishnaveni M.SC (NSG) (Lecturar)Krishnaveni Murugesh100% (1)
- Micro Birth PlanningDocument13 pagesMicro Birth PlanningAnand gowda100% (4)
- National Diabetes Control ProgrammeDocument30 pagesNational Diabetes Control ProgrammePinki Barman100% (1)
- Utilize Community Resources For Self and FamilyDocument38 pagesUtilize Community Resources For Self and FamilyHumera MisterNo ratings yet
- Rajiv Gandhi University of Health Sciences, Bangalore, Karnataka Synopsis Proforma For Registration of Subjects For DissertationDocument14 pagesRajiv Gandhi University of Health Sciences, Bangalore, Karnataka Synopsis Proforma For Registration of Subjects For Dissertationpavin0% (1)
- Counseling - GATHER approach-ANAND MLHPDocument9 pagesCounseling - GATHER approach-ANAND MLHPAnand gowdaNo ratings yet
- High Risk Approach in Maternal and Child HealthDocument6 pagesHigh Risk Approach in Maternal and Child Healthjyotshna sahoo100% (5)
- Assignmenton Episiotomy CareDocument5 pagesAssignmenton Episiotomy CarePriyaNo ratings yet
- School Health ServiceDocument6 pagesSchool Health ServiceJENISHA SWEETYNo ratings yet
- Antenatal Diet PlanDocument7 pagesAntenatal Diet PlanSunija Selvam100% (3)
- Unit 5Document95 pagesUnit 5Sona amoreux De JESUSNo ratings yet
- Reproductive and Child Health ProgrammeDocument10 pagesReproductive and Child Health ProgrammeMebin NinanNo ratings yet
- Ational Ealth Rogramme Elated O Hild Elfare: Presented byDocument98 pagesAtional Ealth Rogramme Elated O Hild Elfare: Presented byshubham vermaNo ratings yet
- Seminor 2 National Health.....Document11 pagesSeminor 2 National Health.....Ratna VimalNo ratings yet
- National Water SupplyDocument51 pagesNational Water SupplyA J Fathima100% (2)
- NHP 1Document46 pagesNHP 1A J FathimaNo ratings yet
- NHP 2Document42 pagesNHP 2A J FathimaNo ratings yet
- Health SchemesDocument70 pagesHealth SchemesA J FathimaNo ratings yet
- BSC N Regulations 2010 Ver 2Document183 pagesBSC N Regulations 2010 Ver 2Susan HepziNo ratings yet
- UN Agencies Improving Global HealthDocument30 pagesUN Agencies Improving Global HealthA J FathimaNo ratings yet
- Psychotherapy in ObstetricsDocument6 pagesPsychotherapy in ObstetricsA J FathimaNo ratings yet
- Demonstration ON Care of Newborn PhototherapyDocument28 pagesDemonstration ON Care of Newborn PhototherapyA J Fathima100% (1)
- LSCSDocument4 pagesLSCSA J FathimaNo ratings yet
- Psychotherapy in ObstetricsDocument6 pagesPsychotherapy in ObstetricsA J FathimaNo ratings yet
- Vital statistics uses and definitionsDocument5 pagesVital statistics uses and definitionsA J FathimaNo ratings yet
- Assignment ON Family Welfare: Submitted To: Submitted byDocument18 pagesAssignment ON Family Welfare: Submitted To: Submitted byA J FathimaNo ratings yet
- Demonstration ON Care of Newborn PhototherapyDocument28 pagesDemonstration ON Care of Newborn PhototherapyA J Fathima100% (1)
- Activity 6: Identification and Appropriate Management of Communicable DiseasesDocument2 pagesActivity 6: Identification and Appropriate Management of Communicable DiseasesA J FathimaNo ratings yet
- Demonstration ON Care of Newborn PhototherapyDocument28 pagesDemonstration ON Care of Newborn PhototherapyA J Fathima100% (1)
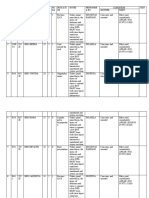
- Activity 28 Conducting Vaginal Examination: Fathima.SDocument2 pagesActivity 28 Conducting Vaginal Examination: Fathima.SA J FathimaNo ratings yet
- Activity 27 Monitoring Labour and Maintaining Partograph: Fathima.SDocument3 pagesActivity 27 Monitoring Labour and Maintaining Partograph: Fathima.SA J FathimaNo ratings yet
- Activity 29Document2 pagesActivity 29A J FathimaNo ratings yet
- Assessing and Caring for an Antenatal WomanDocument5 pagesAssessing and Caring for an Antenatal WomanA J FathimaNo ratings yet
- Wrist Stretching and Posture Guide: @kastor - UyDocument14 pagesWrist Stretching and Posture Guide: @kastor - UyIzzaldinNo ratings yet
- Annotated-Bibliography Final v2Document10 pagesAnnotated-Bibliography Final v2IrvingNo ratings yet
- Guia Clínica Royal CollegeDocument432 pagesGuia Clínica Royal CollegeFernanda Bermudez BustosNo ratings yet
- Word form siêu khó làm chao đảo thế giới ảo (nguồn tổng hợpDocument9 pagesWord form siêu khó làm chao đảo thế giới ảo (nguồn tổng hợpVu Ngoc Quynh AnhNo ratings yet
- Theories of AgingDocument6 pagesTheories of AgingNana Ba100% (1)
- PhD Thesis AcknowledgementDocument3 pagesPhD Thesis AcknowledgementNeelamegam DevarasuNo ratings yet
- Crystal pH Guide: Common & Uncommon CrystalsDocument4 pagesCrystal pH Guide: Common & Uncommon CrystalsyholicNo ratings yet
- 1628 6995 3 PBDocument32 pages1628 6995 3 PBPelayanan Tahanan Rutan KendariNo ratings yet
- Levels of Evidence Flow Chart Rev May 2019Document3 pagesLevels of Evidence Flow Chart Rev May 2019Karl RobleNo ratings yet
- Solid Waste Management Policy Framework: Gaps and IssuesDocument20 pagesSolid Waste Management Policy Framework: Gaps and IssuesThe Outer Marker100% (5)
- Musculoskeletal AssessmentDocument6 pagesMusculoskeletal Assessmentapi-315110874No ratings yet
- Frenillo LingualDocument9 pagesFrenillo LingualJosé DavidNo ratings yet
- Waste ManagementDocument2 pagesWaste Managementagatha bellNo ratings yet
- Volume3 Issue8 (4) 2014Document342 pagesVolume3 Issue8 (4) 2014iaetsdiaetsdNo ratings yet
- Hoja de Seguridad Clinafarm - Spray - SDS - InglesDocument9 pagesHoja de Seguridad Clinafarm - Spray - SDS - Inglessst incubacolNo ratings yet
- Draft - Msnotice - Medicalexamination - 180713Document31 pagesDraft - Msnotice - Medicalexamination - 180713Benjamin StricklandNo ratings yet
- COPD Update LancetDocument52 pagesCOPD Update LancetlilydariniNo ratings yet
- Brittle Bone Disease Causes Fragile BonesDocument30 pagesBrittle Bone Disease Causes Fragile BonesKhim GoyenaNo ratings yet
- Lapegue 2014Document17 pagesLapegue 2014SuhartiniNo ratings yet
- Family Medicine Concept and Patient ManagementDocument36 pagesFamily Medicine Concept and Patient ManagementSapta YudhaNo ratings yet
- MSDS PhenoxyethanolDocument4 pagesMSDS PhenoxyethanolKurt HaslmannNo ratings yet
- Notes On Child and Adolescent PsychiatryDocument172 pagesNotes On Child and Adolescent PsychiatryachikNo ratings yet
- Tugas BioStatistikDocument3 pagesTugas BioStatistikfrankyNo ratings yet
- Artikel Kebakaran Hutan Dan Lahan - 3344Document21 pagesArtikel Kebakaran Hutan Dan Lahan - 3344Ega Ista NengrumNo ratings yet
- Catalogo Accesorios MINDRAYDocument64 pagesCatalogo Accesorios MINDRAYitalo100% (2)
- SFDA Guidance For Drafting Risk Management Plans of COVID-19 VaccinesDocument16 pagesSFDA Guidance For Drafting Risk Management Plans of COVID-19 VaccinesadasdasNo ratings yet
- Phospholipid Scramblase An UpdateDocument7 pagesPhospholipid Scramblase An UpdateUmmiNo ratings yet
- Analysis of The Future Development Trend of The Pet IndustryDocument8 pagesAnalysis of The Future Development Trend of The Pet IndustryKuvar Santosh PatelNo ratings yet