Professional Documents
Culture Documents
Screen-and-Treat Approaches For Cervical Cancer Prevention in Low-Resource Settings
Uploaded by
Saddam FuadOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Screen-and-Treat Approaches For Cervical Cancer Prevention in Low-Resource Settings
Uploaded by
Saddam FuadCopyright:
Available Formats
ORIGINAL CONTRIBUTION
Screen-and-Treat Approaches for Cervical
Cancer Prevention in Low-Resource Settings
A Randomized Controlled Trial
Lynette Denny, MD, PhD Context Non–cytology-based screen-and-treat approaches for cervical cancer pre-
Louise Kuhn, PhD vention have been developed for low-resource settings, but few have directly ad-
Michelle De Souza, MD dressed efficacy.
Amy E. Pollack, MD, MPH Objective To determine the safety and efficacy of 2 screen-and-treat approaches
for cervical cancer prevention that were designed to be more resource-appropriate
William Dupree, MD than conventional cytology-based screening programs.
Thomas C. Wright, Jr, MD Design, Setting, and Patients Randomized clinical trial of 6555 nonpregnant women,
aged 35 to 65 years, recruited through community outreach and conducted between
E
ACH YEAR 471 000 CASES AND June 2000 and December 2002 at ambulatory women’s health clinics in Khayelitsha,
233 000 deaths occur from cer- South Africa.
vical cancer worldwide, of which Interventions All patients were screened using human papillomavirus (HPV) DNA
80% occur in less-developed testing and visual inspection with acetic acid (VIA). Women were subsequently ran-
countries that have access to less than domized to 1 of 3 groups: cryotherapy if she had a positive HPV DNA test result; cryo-
5% of global cancer treatment re- therapy if she had a positive VIA test result; or to delayed evaluation.
sources.1 The lifetime risk of a woman Main Outcome Measures Biopsy-confirmed high-grade cervical cancer precur-
developing cervical cancer in a low- sor lesions and cancer at 6 and 12 months in the HPV DNA and VIA groups compared
resource setting is approximately 2% to with the delayed evaluation (control) group; complications after cryotherapy.
4%.2-4 Cytology-based screening pro- Results The prevalence of high-grade cervical intraepithelial neoplasia and cancer (CIN
grams have markedly reduced the inci- 2⫹) was significantly lower in the 2 screen-and-treat groups at 6 months after random-
dence of cervical cancer in developed ization than in the delayed evaluation group. At 6 months, CIN 2⫹ was diagnosed in
countries that have the infrastructure to 0.80% (95% confidence interval [CI], 0.40%-1.20%) of the women in the HPV DNA
support these programs.5 However, group and 2.23% (95% CI, 1.57%-2.89%) in the VIA group compared with 3.55%
screening programs have proven diffi- (95% CI, 2.71%-4.39%) in the delayed evaluation group (P⬍.001 and P=.02 for the
cult to implement in low-resource set- HPV DNA and VIA groups, respectively). A subset of women underwent a second col-
tings. There are 2 predominant reasons poscopy 12 months after enrollment. At 12 months the cumulative detection of CIN
2⫹ among women in the HPV DNA group was 1.42% (95% CI, 0.88%-1.97%), 2.91%
why cytology-based programs have
(95% CI, 2.12%-3.69%) in the VIA group, and 5.41% (95% CI, 4.32%-6.50%) in the
proven difficult to implement and sus- delayed evaluation group. Although minor complaints, such as discharge and bleeding,
tain in low-resource settings. One is the were common after cryotherapy, major complications were rare.
nature of the screening test.6 High-
Conclusion Both screen-and-treat approaches are safe and result in a lower preva-
quality cytology laboratories are diffi- lence of high-grade cervical cancer precursor lesions compared with delayed evalua-
cult to maintain and there are often sub- tion at both 6 and 12 months.
stantial delays before the results become
Trial Registration Clinicaltrials.gov Identifier: NCT00233727.
available.7 Another is the extensive
JAMA. 2005;294:2173-2181 www.jama.com
workup that is typically used for women
with abnormal cytological results. In de-
Author Affiliations: Department of Obstetrics and Gyn- (Dr Pollack); and HealthNetwork Laboratory, Allen-
veloped countries, women with abnor- aecology, University of Cape Town, Cape Town, South town, Pa (Dr Dupree).
Africa (Drs Denny and De Souza); Gertrude H. Ser- Corresponding Author: Thomas C. Wright, Jr, MD,
gievsky Center and Departments of Epidemiology (Dr Department of Pathology, Room 16-404, P&S Bldg,
See also pp 2182, 2210, and 2225. Kuhn) and Pathology (Dr Wright), Columbia Univer- 630 W 168th St, New York, NY 10032 (tcw1
sity, New York, NY; EngenderHealth, New York, NY @columbia.edu).
©2005 American Medical Association. All rights reserved. (Reprinted) JAMA, November 2, 2005—Vol 294, No. 17 2173
Downloaded From: http://jama.jamanetwork.com/ by a New York Medical College User on 10/09/2015
CERVICAL CANCER PREVENTION IN LOW-RESOURCE SETTINGS
mal cytological results are usually re- Participants and domization was done using a computer-
ferred for colposcopy with biopsy before Clinical Examinations generated randomization schedule with
initiating treatment.8 Although this helps Never screened, nonpregnant women group assignments provided to the clin-
ensure that only women with high- aged 35 to 65 years were enrolled at 3 ics in sealed envelopes. Randomiza-
grade cervical cancer precursors re- clinical sites in close proximity in Khay- tion schedules were generated in
ceive treatment, colposcopy services and elitsha, South Africa. All women pro- batches of 300 to maintain a 1:1:1 ra-
histopathologic laboratories often are not vided informed consent, completed a tio between groups during study en-
available in low-resource settings. questionnaire, received counseling for rollment. Cryotherapy was performed
Recently, a novel approach to cervi- confidential human immunodeficiency by nurses using nitrous oxide and a
cal cancer prevention has been pro- virus (HIV) testing, a pregnancy test if cryosurgical unit (Wallach Surgical De-
posed that avoids the complex health not postmenopausal, anonymous HIV vices, Orange, Conn) with two
infrastructure required by traditional serotesting, and a vaginal speculum 3-minute freezes.17 Both treated and un-
approaches.9,10 This approach incorpo- examination performed by nurses trained treated women were asked to return at
rates non–cytology-based screening in VIA (also referred to as direct visual 4 weeks to complete a questionnaire.
methods such as human papillomavi- inspection as previously described14). At 6 months, a colposcopy was per-
rus (HPV) DNA testing or visual in- Cervical specimens were obtained for formed by a physician blinded to group
spection with acetic acid (VIA) fol- testing for Neisseria gonorrhoeae, Chla- assignment and clinical information. All
lowed by treatment using cryotherapy mydia trachomatis and high-risk types of acetowhite lesions required biopsy and
of all eligible women with positive test HPV, and cytology. The cervix was all women irrespective of whether a le-
results. Both of these approaches per- washed with 5% acetic acid and inspected sion was observed underwent an en-
form as well as or better than cytology- for gross abnormalities or areas of aceto- docervical curettage. Women with CIN
based screening for identifying high- whitening and a 35-mm photograph was 2⫹ were treated appropriately. Assess-
grade cervical cancer precursor lesions taken. ment and treatment of women who be-
and cryotherapy is a relatively low- Women with significant cervicitis or came pregnant during the study was
technology treatment method that is vulvovaginitis were treated using the postponed until 3 months postpar-
highly efficacious and has minimal mor- syndromic approach.15 Women who tum. Blood for anonymous HIV sero-
bidity.11-13 had positive test results for N gonor- testing was obtained. All women who
The screen-and-treat approaches de- rhoeae or C trachomatis received ap- had either HPV DNA or VIA positive
scribed herein have advantages for low- propriate treatment. A positive VIA test test results at enrollment and a subset
resource settings because they are not result was defined as any acetowhite le- who had either HPV DNA or VIA nega-
cytology-based screening programs and sion and no attempt was made to dif- tive test results (all women enrolled in
they do not require colposcopy ser- ferentiate the acetowhitening of meta- 2002) were scheduled for repeat col-
vices, which overcome 2 of the great- plasia from CIN.16 A total of 451 women poscopy at 12 months.
est barriers to cervical cancer preven- were excluded because they had le- The study was approved by the insti-
tion. However, the efficacy of the sions suspicious for cancer (n = 46), tutional review boards of Columbia Uni-
screen-and-treat approaches has not yet large acetowhite lesions extending over versity (New York, NY) and the Univer-
been established, and there are only lim- 70% of the cervix (n=17) or into en- sity of Cape Town (Cape Town, South
ited safety data.9 docervical canal (n=14), or were ineli- Africa). All participants provided writ-
gible for cryotherapy due to severe at- ten informed consent. A data and safety
METHODS rophy (n=83), polyps (n=135), cervix monitoring board monitored the trial.
Study Design distorted (n = 86), cervix not ad-
Our study was designed to measure equately visualized (n=55), and other Laboratory Testing
the impact of the screen-and-treat ap- reasons (n = 15). These excluded The Hybrid Capture 2 assay and high-
proach on the prevalence of high- women were referred for a colpos- risk probe mixture (Digene Corp, Gaith-
grade cervical intraepithelial neo- copy. Cervical cancer was detected in ersburg, Md) was used at the Univer-
plasia and cancer (CIN 2⫹). The 23 of these women, of whom 20 had a sity of Cape Town for HPV DNA testing.
randomized clinical trial described grossly visible lesion. Biopsies were processed at Columbia
herein compared 2 screen-and-treat Women returned 2 to 6 days later for University and evaluated by a single pa-
groups (HPV DNA testing and VIA) randomization to either the (1) HPV thologist who was blinded to the study
with a control group that received DNA group in which all women with randomization.18 Endocervical curet-
delayed evaluation. The primary positive HPV DNA test results re- tages containing high-grade cervical neo-
outcomes were biopsy-confirmed ceived cryotherapy; (2) VIA group in plasia were classified as positive for CIN
CIN 2⫹ at 6 months and significant which all women with positive VIA test 2⫹. At the end of the study, all biop-
complications within 6 months of ran- results received cryotherapy; or (3) de- sies classified as CIN and all biopsies
domization. layed evaluation (control) group. Ran- originally classified as normal from
2174 JAMA, November 2, 2005—Vol 294, No. 17 (Reprinted) ©2005 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by a New York Medical College User on 10/09/2015
CERVICAL CANCER PREVENTION IN LOW-RESOURCE SETTINGS
women who had an HPV DNA positive vals (CI) around the proportions were average of the Kaplan-Meier life-table es-
test result or who had a cytological re- calculated using a binomial estimate. A timate in the stratum with positive test
sult of low-grade squamous intraepithe- stratified analysis by HIV serostatus was results for HPV DNA or VIA and the stra-
lial lesion or greater at enrollment were preplanned. The efficacy of each screen- tum with negative test results for HPV
rereviewed by the same pathologist at and-treat approach was quantified as the DNA or VIA, weighting each stratum-
Columbia University. If the second re- percentage difference in CIN 2⫹ attrib- specific estimate by the proportion in
view did not result in the same assess- utable to the approach (disease preva- each stratum at randomization. The 95%
ment as the first review, slides were re- lence in the delayed evaluation [con- CIs were calculated using the stratum-
viewed by another pathologist for a final trol] group minus that in the treatment specific SEs from the Kaplan-Meier life-
diagnosis (concordance on 2 of 3 re- group divided by that in the delayed table estimate.22
views). Among the 611 women for evaluation group). The cumulative The safety analyses compared the oc-
whom biopsies were blindly reviewed, prevalence of CIN 2⫹ by 12 months in currence of specific outcomes between
the reviews were concordant in 491 each group was calculated as a weighted- groups and among those who did and did
(97%) of 506 originally classified as not
having CIN 2⫹ and 100 (95%) of 105
originally classified as having CIN 2⫹. Table 1. Sociodemographic Characteristics and Risk Factors for Cervical Disease at
The coefficient agreement between the Enrollment*
2 reviews was 0.89.19 In 6 discordant Delayed Evaluation
HPV DNA Group VIA Group (Control) Group
cases there remained a discrepancy af- (n = 2163) (n = 2227) (n = 2165)
ter the third independent review that was Age, mean (SD), y 43.3 (6.9) 43.3 (7.2) 43.4 (7.3)
resolved in conference. Age, y
35-39 818 (37.8) 862 (38.7) 866 (40.0)
Statistical Analysis 40-49 924 (42.7) 935 (42.0) 870 (40.2)
For power calculations, the preva- 50-65 422 (19.5) 430 (19.3) 429 (19.8)
lence of CIN 2⫹ in the population was Positive test result
Human papillomavirus† 474 (21.9) 483 (21.7) 446 (20.6)
estimated to be 3%.20,21 Based on 80%
Visual inspection with acetic acid 467 (21.6) 492 (22.1) 500 (23.1)
power with a 1-sided ␣ of .05 indicat-
Cytology
ing significance and using a Bonfer- LSIL on Papanicolaou test 134 (6.2) 158 (7.1) 134 (6.2)
roni correction for 3 pairwise compari- Chlamydia trachomatis and 117 (5.4) 118 (5.3) 104 (4.8)
sons and 1-tail testing, it was calculated Neisseria gonorrhoeae‡
that 1664 participants per group were Trichomonas vaginalis 236 (10.9) 245 (11.0) 221 (10.2)
needed to detect a reduction of greater Human immunodeficiency virus 268 (12.4) 252 (11.3) 264 (12.2)
than 50% in CIN 2⫹ at 6 months in Moderate to severe vaginal discharge 500 (23.1) 517 (23.2) 498 (23.0)
treatment groups compared with the Treated for cervicitis or vulvovaginitis 554 (25.6) 546 (24.5) 546 (25.2)
delayed evaluation group. One-tail test- Married 1097 (50.7) 1116 (50.1) 1104 (51.0)
ing was used because there is little bio- Age ⬍16 y at first sexual intercourse 731 (33.8) 777 (34.9) 738 (34.1)
logical basis to expect the interven- ⱖ5 Lifetime sex partners 740 (34.2) 753 (33.8) 743 (34.3)
ⱖ2 Sex partners during previous month 30 (1.4) 36 (1.6) 28 (1.3)
tions to increase disease relative to the
Current smoker 160 (7.4) 183 (8.2) 165 (7.6)
delayed evaluation group. This meant
No. of live births
screening 7200 women, assuming that None 76 (3.5) 73 (3.3) 82 (3.8)
70% would be eligible for the study and 1-4 1395 (64.5) 1441 (64.7) 1431 (66.1)
would be followed up at 6 months. Sta- ⱖ5 692 (32.0) 713 (32.0) 652 (30.1)
tistical power to evaluate complica- Education
tions of therapy varied with the ex- No school 203 (9.4) 218 (9.8) 197 (9.1)
pected prevalence of the end point. For Some primary school 813 (37.6) 831 (37.3) 799 (36.9)
HIV seroconversion, the trial had suf- Some high school 956 (44.2) 1022 (45.9) 989 (45.7)
ficient power to detect an increase of High school graduate 188 (8.7) 154 (6.9) 180 (8.3)
more than 2-fold in seroconversion Currently employed 575 (26.6) 537 (24.1) 520 (24.0)
across groups at 6 months, assuming Current contraceptive use
Injectable 318 (14.7) 379 (17.0) 325 (15.0)
a 1.5% seroconversion rate in the de-
Oral 32 (1.5) 51 (2.3) 43 (2.0)
layed evaluation group.
Abbreviations: HPV, human papillomavirus; LSIL, low-grade squamous intraepithelial lesion; VIA, visual inspection with
The prevalence of CIN 2⫹ detected by acetic acid.
*Values are expressed as number (percentage) unless otherwise indicated. P⬎.05 for comparisons across all 3 groups.
6 months in each of the 3 groups was †Identified by using Hybrid Capture 2 (Digene Corp, Gaithersburg, Md).
compared between the groups using 2 ‡Test results were not available until several weeks after randomization. More than 60% of these women were asymp-
tomatic and were not treated prior to randomization using the syndromic approach.15
tests (2-sided); 95% confidence inter-
©2005 American Medical Association. All rights reserved. (Reprinted) JAMA, November 2, 2005—Vol 294, No. 17 2175
Downloaded From: http://jama.jamanetwork.com/ by a New York Medical College User on 10/09/2015
CERVICAL CANCER PREVENTION IN LOW-RESOURCE SETTINGS
not undergo cryotherapy within a group. December 2002. Of these, 6555 (99%) nancy (n=3), delay due to bleeding or
Comparisons were made using 2 tests. returned 2 to 6 days later for random- infection and subsequently lost to fol-
SAS statistical software version 8.0 (SAS ization. There were no significant dif- low-up (n = 6), clinician error (n = 5),
Institute Inc, Cary, NC) was used. ferences in sociodemographic charac- and ineligibility (n = 4). Of 949 cryo-
teristics or risk factors for CIN between therapy procedures, 877 (92%) were
RESULTS groups at enrollment (TABLE 1). performed on the day of randomiza-
Participant Profile Of 2163 women in the HPV DNA tion. Cryotherapy for 28 women in the
and Protocol Adherence group, 467 (22%) underwent cryo- HPV DNA group and 44 in the VIA
A total of 7088 women were evalu- therapy. Of 2227 women in the VIA group (P=.07) was delayed due to in-
ated; 6637 (94%) met the eligibility cri- group, 482 (22%) underwent cryo- fection (n = 37), bleeding (n = 9), and
teria and underwent a complete exami- therapy. Cryotherapy was not per- other reasons (n=26). Of women un-
nation between June 2000 and formed in 18 women due to preg- dergoing cryotherapy, 136 (29%) in the
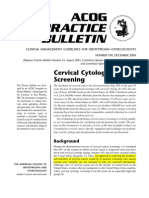
Figure 1. Distribution of Participants
7088 Women Initially Evaluated
451 Ineligible for Study
46 Suspicious for Cancer∗
31 Lesion Related∗
374 Unsuitable for Cryotherapy
6637 Eligible for Enrollment and Underwent
HPV DNA and VIA Testing
82 Did Not Return for Randomization
6555 Randomized
2163 Assigned to Receive Cryotherapy 2227 Assigned to Receive Cryotherapy 2165 Assigned to Delayed Evaluation
if HPV DNA Test Result Positive if VIA Test Result Positive
RESULTS OF INITIAL
SCREENING
473 HPV+ 309 VIA+ 1381 VIA– 492 VIA+ 314 HPV+ 1421 VIA– 781 VIA+ 1384 VIA–
and and and and or and
HPV– HPV– VIA– HPV– HPV+ HPV–
465 Underwent 1 Underwent 1 Underwent 482 Underwent
Cryotherapy Cryotherapy† Cryotherapy† Cryotherapy
1 Excluded‡ 1 Excluded‡
COLPOSCOPY
AT 6 MO
391 269 1219 424 260 1245 652 1207
13 Cases of 0 Cases of 2 Cases of 11 Cases of 31 Cases of 1 Case of 64 Cases of 2 Cases of
CIN 2+ CIN 2+ CIN 2+ CIN 2+ CIN 2+ CIN 2+ CIN 2+ CIN 2+
449 Selected § 475 Selected § 470 Selected §
COLPOSCOPY
AT 12 MO
324 222 351 371 200 379 500 361
9 Cases of 1 Case of 0 Cases of 1 Case of 9 Cases of 1 Case of 25 Cases of 2 Cases of
CIN 2+ CIN 2+ CIN 2+ CIN 2+ CIN 2+ CIN 2+ CIN 2+ CIN 2+
1879 Included in Analysis 1929 Included in Analysis 1859 Included in Analysis
of 6-mo Outcomes of 6-mo Outcomes of 6-mo Outcomes
897 Included in Analysis 950 Included in Analysis 861 Included in Analysis
of 12-mo Outcomes of 12-mo Outcomes of 12-mo Outcomes
CIN 2⫹ indicates high-grade cervical intraepithelial neoplasia and cancer; HPV, human papillomavirus; VIA, visual inspection with acetic acid.
*Considered ineligible for enrollment because VIA showed either a cervical mass or an acetowhite lesion inappropriate for cryotherapy.
†Received cryotherapy in error.
‡Cancer detected based on postrandomization assessment of cervical photographs and cytology.
§A subset of women who had negative test results for both VIA and HPV DNA were selected for 12-month follow-up.
2176 JAMA, November 2, 2005—Vol 294, No. 17 (Reprinted) ©2005 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by a New York Medical College User on 10/09/2015
CERVICAL CANCER PREVENTION IN LOW-RESOURCE SETTINGS
HPV DNA group and 143 (30%) in the delayed evaluation group. No signifi- Clinical trials of therapies for CIN
VIA group received antibiotic or anti- cant differences in the effect of either have typically followed up women for
fungal medication at the initial screen- screen-and-treat approach were ob- 12 months or longer. Therefore, all
ing for cervicitis or vulvovaginitis. served between the 3 clinical sites.
If CIN 3⫹ (CIN 3 and cancer) was Table 2. Follow-up Rates at 6 Months
Impact of Screen-and-Treat used as the study end point at 6 months, No. (%) of P
Approach at 6 and 12 Months a significant effect was seen in the HPV Participants Value
Six-month outcome data were ob- DNA group (P⬍.001) but not in the Randomization group
HPV DNA 2163 (86.9)
tained in 5667 women (86% of those VIA group (P = .11). If CIN 1⫹ (all
VIA 2227 (86.6) .60
randomized; FIGURE 1). Follow-up rates grades of CIN and cancer) was used as Delayed evaluation 2165 (85.9)
did not significantly differ between the study end point, the magnitude of (control)
groups (P=.60) or between those who the effect in the HPV DNA group was Cryotherapy
did or did not undergo cryotherapy less but remained significant (P⬍.001); Received 949 (85.6)
.39
(P=.39). The interval between enroll- no significant effect was observed in the Did not receive 5606 (86.6)
ment and the 6-month follow-up visit VIA group (P =.36) (FIGURE 2). Baseline Results
was also similar between groups (mean To investigate whether participants Papanicolaou test
ⱖLSIL 5920 (86.5)
[SD],188 [49] days for the HPV DNA lost to follow-up may have biased our .15
⬍LSIL 412 (83.9)
group; 188 [48] days for the VIA group; findings, we calculated what the ex- HPV DNA test
and 190 [55] days for the delayed evalu- pected effect of the 2 screen-and-treat in- Positive 1402 (83.2)
⬍.001
ation group). There were significant but terventions would have been if all Negative 5150 (87.3)
small differences in baseline HPV and women who had cytology results of low- VIA test
HIV status but not in other character- grade squamous intraepithelial lesion or Positive 1459 (85.1)
.09
Negative 5096 (86.8)
istics (TABLE 2). greater at enrollment and who were lost
HIV test
Compared with the delayed evalua- to follow-up (23 in the HPV DNA group, Positive 782 (83.6)
tion group, the prevalence of biopsy- 21 in the VIA group, and 20 in the de- .01
Negative 5760 (86.8)
confirmed CIN 2⫹ at 6 months was sig- layed evaluation group) had returned Sociodemographic Characteristics
nificantly less in both the HPV DNA and had CIN 2⫹ at 6 months, regard- Age, y
(P⬍.001) and VIA groups (P = .02). At less of whether they had received cryo- 35-39 2544 (85.9)
6 months, CIN 2⫹ was diagnosed in therapy (ie, the intervention com- 40-49 2729 (88.1) .002
0.80% (95% CI, 0.40%-1.20%) of the pletely failed among those lost to follow- 50-65 1282 (84.2)
women in the HPV DNA group and up). Under these assumptions the Status
Married 3317 (85.8)
2.23% (95% CI, 1.57%-2.89%) in the prevalence of CIN 2⫹ in the HPV DNA .14
Unmarried 3238 (87.1)
VIA group compared with 3.55% (95% group would have been 1.76%; VIA
Age at first sexual
CI, 2.71%-4.39%) in the delayed evalu- group, 2.88%; and delayed evaluation intercourse
ation group. Thus, the screen-and- group, 3.97%. Compared with the de- ⬍16 y 2246 (86.2)
.66
treat approach using HPV DNA test- layed evaluation group, there would ⱖ16 y 4309 (86.6)
ing was associated with a 77% lower have been a 56% reduction in the preva- No. of lifetime
sex partners
prevalence of CIN 2⫹ than in the de- lence of CIN 2⫹ in the HPV DNA group ⱖ5 2233 (87.4)
.12
layed evaluation group at 6 months, and a 27% reduction in the VIA group. ⬍5 4322 (86.0)
whereas the screen-and-treat ap- We also investigated whether the No. of live births
proach using VIA was associated with lower prevalence of CIN 2⫹ at 6 months None 232 (87.5)
a 37% lower prevalence (TABLE 3). in the screen-and-treat groups was due 1-4 4267 (87.0) .10
The prevalence of CIN 2⫹ in the HPV to changes in sexual behavior as a func- ⱖ5 2056 (85.1)
Education
DNA group at 6 months remained sig- tion of participating in the study or No school 620 (83.7)
nificantly lower than that in the de- knowledge of HIV status. This was done Some primary school 2444 (86.8)
layed evaluation group if the analysis was by comparing the prevalence of CIN 2⫹ .20
Some high school 2968 (86.6)
confined to HIV-seronegative women at 6 months among women in the HPV High school graduate 523 (87.4)
alone, but the difference associated with DNA group who had positive test re- Current contraceptive use
the VIA-based strategy did not. Among sults at enrollment and received cryo- None 5340 (86.0)
women HIV-seronegative at randomiza- therapy with that of women in the de- Injectable 1022 (88.6)
.05
tion (n=5001), CIN 2⫹ was diagnosed layed evaluation group who had HPV Oral 124 (83.9)
in 0.85% (95% CI, 0.40%-1.29%) in the but who did not receive cryotherapy. Other* 69 (92.8)
Abbreviations: HIV, human immunodeficiency virus; HPV,
HPV DNA group compared with 2.11% When stratified by sexual activity and human papillomavirus; LSIL, low-grade squamous intrae-
(95% CI, 1.42%-2.79%) in the VIA group condom use, similar effects of treat- pithelial lesion; VIA; visual inspection with acetic acid.
*Implantable intrauterine devices and condoms.
and 2.75% (95% CI, 1.96%-3.54%) in the ment were observed in all strata.
©2005 American Medical Association. All rights reserved. (Reprinted) JAMA, November 2, 2005—Vol 294, No. 17 2177
Downloaded From: http://jama.jamanetwork.com/ by a New York Medical College User on 10/09/2015
CERVICAL CANCER PREVENTION IN LOW-RESOURCE SETTINGS
women who had positive test results for This translates into 1 case of CIN 2⫹ suspicious for cancer. Twenty-four
HPV DNA or VIA at enrollment, as well being averted for every 25 women en- women returned for evaluation and 2
as a subset of women who had nega- rolled in the HPV DNA group and 1 cases of invasive cancer were identi-
tive test results for HPV DNA and VIA, case being averted for every 40 women fied (both in the VIA group). One
were scheduled for a repeat colpos- enrolled in the VIA group. woman had not received cryotherapy
copy at 12 months. Because CIN 2⫹ because the cancer was in the endocer-
was rarely detected in women who had Complications of Screen-and-Treat vical canal and not visible, the other
negative test results for both HPV DNA Approaches woman had received cryotherapy.
and VIA, this approach allowed us to Many women reported pain or light- There were no differences in HIV-
model the impact of screen-and-treat headedness during the procedure and seroconversion rates 6 months after ran-
approaches at 12 months (Figure 1). most had abnormal vaginal discharge af- domization: 1.06% (95% CI, 0.59%-
Data were obtained from 2708 women terward (TABLE 4). Some had abdomi- 1.53%) in the HPV DNA group; 0.99%
(74% of those scheduled to be exam- nal pain or bleeding in the month after (95% CI, 0.52%-1.46%) in the VIA
ined) and the cumulative prevalence of the procedure, which frequently re- group; and 1.17% (95% CI, 0.66%-
CIN 2⫹ by 12 months in both screen- sulted in consultation with a clinician. 1.68%) in the delayed evaluation group.
and-treat groups continued to be lower One serious adverse event occurred 2 This was also true 12 months after ran-
than in the delayed evaluation group. weeks after cryotherapy. An HIV- domization: 1.76% (95% CI, 0.99%-
In the HPV DNA group, 1.42% (95% positive woman developed severe cervi- 2.53%) in the HPV DNA group; 1.90%
CI, 0.87%-1.97%) had CIN 2⫹ by 12 cal bleeding requiring hospitalization. (95% CI, 1.12%-2.68%) in the VIA
months compared with 2.91% (95% CI, Twenty-seven women were re- group; and 1.95% (95% CI, 1.14%-
2.12%-3.69%) in the VIA group and called some weeks after randomiza- 2.76%) in the delayed evaluation group.
5.41% (95% CI, 4.32%-6.50%) in the tion because their cervical cytology or Approximately half of the women who
delayed evaluation group (Table 3). photograph obtained at screening was underwent cryotherapy had sexual in-
tercourse within 1 month of the pro-
Table 3. Pathological Diagnoses of Cervical Intraepithelial Neoplasia cedure and about 60% of those women
Delayed Evaluation
used condoms (Table 4).
HPV DNA Group VIA Group (Control) Group
Cumulative Prevalence at 6 or 12 mo After Randomization Differential Performance
CIN 2⫹ of HPV DNA and VIA
Total No. 25 54 93 Screen-and-Treat Approaches
% (95% CI)* 1.42 (0.87-1.97) 2.91 (2.12-3.69) 5.41 (4.32-6.50) The efficacy of the screen-and-treat ap-
At 6 mo After Randomization proach depends on both the sensitivity
Evaluated, No. 1879 1929 1859 of the screening test as well as the effi-
CIN 1 45 58 44 cacy of the treatment. The reasons for the
Neoplasia in endocervical curettage 4 5 5 lower prevalence of CIN 2⫹ in the HPV
CIN 2 4 20 33 DNA group compared with the VIA
CIN 3 7 18 27 group were investigated by comparing
Cancer 0 0 1 specific subsets of women within groups
CIN 2⫹ (TABLE 5). Among HPV-positive women
Total No. 15 43 66
% (95% CI) 0.80 (0.40-1.20) 2.23 (1.57-2.89) 3.55 (2.71-4.39)
at enrollment, there was a 74% differ-
ence in cumulative prevalence of CIN 2⫹
At 12 mo After Randomization†
by 12 months in the HPV DNA group
Evaluated, No. 897 950 861
compared with the delayed evaluation
CIN 1 21 27 25
group. Among women with positive VIA
CIN 2 7 8 18
CIN 3 2 3 8
test results at enrollment, there was a
Cancer 1 0 1
78% difference between the VIA group
CIN 2⫹
and the delayed evaluation group. There-
Total No. 10 11 27 fore, the efficacy of cryotherapy was simi-
Abbreviations: CI, confidence interval; CIN, cervical intraepithelial neoplasia; HPV, human papillomavirus; VIA, visual lar in the HPV DNA and VIA groups. The
inspection with acetic acid.
*Calculated as a weighted average of the stratum-specific Kaplan-Meier estimates of the cumulative proportions with lower prevalence of CIN 2⫹ in the HPV
CIN 2⫹ by 12 months per 100 women. DNA group compared with the VIA
†According to the study design, only women who were free of CIN 2⫹ at 6 months, who had positive test results for VIA
or HPV DNA testing at baseline, and a proportionate sampling of women who had negative test results for VIA and HPV group was attributable to initial HPV
DNA at baseline were eligible for 12-month follow-up. Of 1218 women in the HPV DNA group, 897 (74%) underwent
assessment; 950 (77%) of 1237 women in the VIA group; and 861 (73%) of 1187 women in the delayed evaluation DNA testing correctly identifying more
(control) group. The number of mean (SD) days between enrollment and the 12-month follow-up visit were similar among women with CIN 2⫹ at enrollment. This
the groups (HPV DNA group: 385 [48]; VIA group: 388 [51]; delayed evaluation (control) group: 387 [49]).
interpretation is further supported by the
2178 JAMA, November 2, 2005—Vol 294, No. 17 (Reprinted) ©2005 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by a New York Medical College User on 10/09/2015
CERVICAL CANCER PREVENTION IN LOW-RESOURCE SETTINGS
findings among women in the delayed found a low rate of significant compli- countries.25,26 The favorable results ob-
evaluation group. At enrollment, 84 cations and a high rate of participant sat- tained in the current trial suggest that
(90%) of the 93 women subsequently isfaction.9 Although we observed a sig- this perception may be wrong. A screen-
identified with CIN 2⫹ by 12 months nificant impact on the prevalence of and-treat approach lacks many of the
had positive HPV DNA test results CIN 2⫹ with 2 screen-and-treat ap- drawbacks of cytology-based screen-
whereas only 51 (55%) had positive VIA proaches, the magnitude of the impact ing programs. Screening and cryo-
test results. that such programs will have on cervi- therapy can be carried out by mid-level
cal cancer can only be established nurses in a primary care setting. Cytol-
COMMENT through long-term prospective studies. ogy laboratories, which are difficult to
This trial demonstrates that screen- There is considerable interest in ad- sustain and are often of poor quality in
and-treat approaches to cervical can- dressing inequalities in global health.24 low-resource settings, are not needed.7
cer prevention, which overcome many Interest has been focused predomi- With visual screening methods, the en-
of the limitations inherent in tradi- nantly on infectious diseases that are tire program can be administered in 1
tional cytology-based screening pro- considered more easily remedied than visit. As a result, a screen-and-treat ap-
grams, are both safe and efficacious. The many other conditions. Even though cer- proach should be considerably less ex-
HPV DNA–based screen-and-treat vical cancer is the leading cause of can- pensive and easier to implement than
group had up to a 77% lower preva- cer-related death in women in many de- traditional cytology-based screening pro-
lence of CIN 2⫹ compared with the de- veloping countries, cervical cancer grams. We previously evaluated the cost-
layed evaluation group at 6 months and screening is often perceived as being too effectiveness of screen-and-treat strate-
a substantial difference was main- difficult to implement or sustain to be gies if conducted in South Africa.10 Both
tained at 12 months. The VIA-based included in the package of services being 1- and 2-visit strategies using HPV DNA
screen-and-treat approach also had a made available for the world’s poorest or VIA were not only highly attractive
significant, but lesser, impact on CIN
2⫹. Our results underestimate the full
Figure 2. Biopsy-Confirmed Cervical Intraepithelial Neoplasia at 6 and 12 Months
effect that would be obtained in a
screening program because an addi- 6-mo Postrandomization
tional 23 cancer cases and 15 cases of CIN 1+ CIN 2+ CIN 3+
10
CIN 2⫹ were identified during screen-
ing among the 482 women who were 8
ineligible for enrollment into the trial
Cases, %
and referred for further evaluation. The 6
differential in performance of the VIA- 4
based approach compared with the HPV
DNA-based approach is due to the iden- 2
tification of fewer cases of CIN 2⫹ by 0
VIA rather than a differential efficacy HPV DNA- VIA- Delayed HPV DNA- VIA- Delayed HPV DNA- VIA- Delayed
Based Based Evaluation Based Based Evaluation Based Based Evaluation
of cryotherapy. This is consistent with (Control) (Control) (Control)
Screen and Treat Screen and Treat Screen and Treat
a recent evaluation of the perfor-
mance of VIA in 11 different cross-
sectional clinical studies that reported 12-mo Postrandomization
a pooled sensitivity of 76.8% for CIN CIN 1+ CIN 2+ CIN 3+
10
2⫹.23 In contrast, a sensitivity of greater
than 90% has been reported by most 8
large screening trials evaluating HPV
Cases, %
6
DNA testing.12
The risk-to-benefit ratio of the screen- 4
and-treat approaches appear to be highly
favorable. There was only a single seri- 2
ous complication that occurred in an im- 0
munosuppressed HIV-positive patient HPV DNA- VIA- Delayed HPV DNA- VIA- Delayed HPV DNA- VIA- Delayed
Based Based Evaluation Based Based Evaluation Based Based Evaluation
and 99% of participants stated they (Control) (Control) (Control)
Screen and Treat Screen and Treat Screen and Treat
would recommend this type of screen-
ing program to friends and family. A re- Error bars indicate 95% confidence intervals. CIN 1⫹ indicates all grades of cervical intraepithelial neoplasia
cent demonstration project from Thai- and cancer. CIN 2⫹ indicates CIN 2, CIN 3, and cancer. CIN 3⫹ indicates CIN 3 and cancer. HPV indicates
human papillomavirus; VIA, visual inspection with acetic acid.
land of a screen-and-treat approach also
©2005 American Medical Association. All rights reserved. (Reprinted) JAMA, November 2, 2005—Vol 294, No. 17 2179
Downloaded From: http://jama.jamanetwork.com/ by a New York Medical College User on 10/09/2015
CERVICAL CANCER PREVENTION IN LOW-RESOURCE SETTINGS
Table 4. Complications of Cryotherapy*
HPV DNA Group VIA Group Delayed Evaluation
(Control) Group;
Cryotherapy No Cryotherapy Cryotherapy No Cryotherapy No Cryotherapy
(n = 467) (n = 1696) (n = 482) (n = 1745) (n = 2165)
Pain, light-headedness, or other complaint 168 (36) 171 (36)
Within 1 mo
Unscheduled visit† 39 (9) 6 (0.4)‡ 53 (11) 9 (0.5)‡ 14 (0.7)
Hospital admission 1 (0.2) 3 (0.2) 1 (0.2) 4 (0.2) 4 (0.2)
Participants followed up at 1 mo 449 (96) 1646 (97) 470 (98) 1695 (97) 2096 (97)
New and troubling symptoms† 120 (27) 160 (10)‡ 119 (25) 162 (10)‡ 223 (11)
Consulted clinician 93 (21) 286 (17) 108 (23) 307 (18)‡ 401 (19)
Vaginal discharge† 353 (79) 429 (26)‡ 389 (83) 401 (24)‡ 558 (27)
Abnormal bleeding 64 (14) 108 (7)‡ 66 (14) 105 (6)‡ 142 (7)
Abdominal pain 144 (32) 340 (21)‡ 138 (29) 353 (21)‡ 460 (22)
Sex since last visit†§ 216 (48) 1044 (63)‡ 249 (53.0) 1090 (64)‡ 1341 (64)
Used male or female condoms most of 121 (56) 176 (17)‡ 149 (60) 170 (16)‡ 236 (18)
the time or always†
Would recommend program to their friends 448 (99.9) 1644 (99.9) 470 (100) 1693 (99.9) 2092 (99.8)
and relatives
Prior to 6 mo
Cervical cancer 㛳 0 0 1 1 0
Abbreviations: HPV, human papillomavirus; VIA, visual inspection with acetic acid.
*Values are expressed as number (percentage).
†P⬍.05 for comparisons across the 3 groups.
‡P⬍.05 for comparisons of women receiving cryotherapy and those not receiving cryotherapy.
§After treatment, women were instructed to abstain from vaginal intercourse, douching, or using intravaginal products for 4 weeks and given condoms to use if sexually active.
㛳Two cancers were missed on initial screening but were later detected prior to the 6-month study visit based on review of enrollment cytology and photographs.
sures that any effect of participating in
Table 5. Cumulative Probability of CIN 2⫹ by 12 Months
the trial are shared across all groups; (2)
CIN 2⫹ by 12 mo that it targeted women aged 35 years
Randomization Group No. of Participants % (95% CI)* or older, which is the optimal age to ini-
HPV DNA (n = 2163) tiate cervical cancer screening in low-
Cryotherapy 22 5.86 (3.47-8.25) resource settings2,4; and (3) that all par-
No cryotherapy 3 0.31 (0-0.69) ticipants underwent colposcopy and
VIA (n = 2227)
Cryotherapy 12 2.73 (1.20-4.26)
histological sampling at 6 months with
No cryotherapy 42 3.74 (2.49-4.99)
blinded review of all results making as-
Delayed evaluation (control) (n = 2165) certainment bias unlikely.
No cryotherapy 93 3.55 (2.71-4.39) The study also has several potential
HPV limitations. One limitation is the length
Positive 84 23.00 (18.60-27.40)
of follow-up for the primary end point.
Negative 9 1.10 (0.33-1.87)
To measure the impact of screen-and-
VIA
Positive 51 12.50 (9.28-15.70) treat approaches it was important to have
Negative 42 4.20 (2.79-5.61) a delayed evaluation group. However, fol-
Abbreviations: CIN 2⫹, high-grade cervical intraepithelial neoplasia and cancer; HPV, human papillomavirus; VIA, vi- low-up of this delayed evaluation group
sual inspection with acetic acid. for longer than 6 months without treat-
*Calculated as the stratum-specific Kaplan-Meier estimates of the cumulative proportions with CIN2⫹ by 12 months
per 100 women. ing women with CIN 2⫹ was unaccept-
able. Another limitation is our power for
detecting increases in HIV seroconver-
compared with traditional cytology- scale public health intervention projects sions after treatment. Although the find-
based approaches, but also had cost- to better define the operational aspects ing of no excess of HIV seroconver-
effectiveness ratios comparable with of these programs. Such studies also sions in the HPV DNA and VIA groups
well-accepted health interventions, such should evaluate reductions in cervical is reassuring, the study is underpow-
as childhood vaccines. Now that the cancer through long-term monitoring of ered to detect small increases and larger
safety and efficacy of screen-and-treat treated populations. trials are need to more fully investigate
programs have been demonstrated, the The key strengths of the trial are (1) the impact of cryotherapy on HIV trans-
next step should be to conduct large- the randomized design, which en- mission. We also did not conduct the
2180 JAMA, November 2, 2005—Vol 294, No. 17 (Reprinted) ©2005 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by a New York Medical College User on 10/09/2015
CERVICAL CANCER PREVENTION IN LOW-RESOURCE SETTINGS
screen-and-treat approaches in a single sults of 2 alternative screening tests to Analysis and interpretation of data: Denny, Kuhn,
Wright.
visit. Instead, women returned several cytology, HPV DNA testing and VIA, Drafting of the manuscript: Denny, Kuhn, Pollack,
days after initial screening for treat- is safe and has a significant impact on Wright.
Critical revision of the manuscript for important in-
ment. Although we obtained high rates the prevalence of CIN 2⫹ among tellectual content: DeSouza, Dupree, Wright.
of follow-up, lower follow-up might oc- women participating in such a pro- Statistical analysis: Kuhn, Wright.
cur in a real-world service delivery set- gram. In low-resource settings, screen- Obtained funding: Pollack, Wright.
Administrative, technical, or material support: Denny,
ting. This would reduce the efficacy of and-treat approaches may be able to re- DeSouza, Wright.
the HPV DNA–based strategy com- duce the risk of a common and easily Study supervision: Wright.
Financial Disclosures: None reported.
pared with the VIA-based strategy, which preventable cancer in women. Funding/Support: This study was funded by the Bill
can be administered in a single visit. and Melinda Gates Foundation through a grant to the
Moreover, the study was neither pow- Author Contributions: Dr Wright had full access to all Alliance for Cervical Cancer Prevention, the Cancer
of the data in the study and takes responsibility for Association of South Africa, and the Department of
ered nor designed to detect differences the integrity of the data and the accuracy of the data National Health, South Africa.
in cancer rates. analysis. Role of the Sponsor: The funding organizations played
Study concept and design: Denny, Kuhn, Pollack, no role in the design and conduct of the study or data
This trial has shown that screening Wright. analysis, interpretation of the data, or preparation, re-
and treating women based on the re- Acquisition of data: Denny, DeSouza, Dupree, Wright. view, or approval of the manuscript.
REFERENCES
1. Parkin DM. Global cancer statistics in the year 2000. 10. Goldie SJ, Kuhn L, Denny L, Pollack A, Wright TC. ous lesions of the cervix. In: Kurman RJ, ed. Blaus-
Lancet Oncol. 2001;2:533-543. Policy analysis of cervical cancer screening tein’s Pathology of the Female Genital Tract. 5th ed.
2. Goldie SJ, Grima D, Kohli M, et al. A comprehensive strategies in low-resource settings: clinical benefits New York, NY: Springer-Verlag; 2002:253-354.
natural history model of HPV infection and cervical can- and cost-effectiveness. JAMA. 2001;285:3107-3115. 19. Kundel HL, Polansky M. Measurement of
cer to estimate the clinical impact of a prophylactic HPV- 11. Cox JT. Management of cervical intraepithelial observer agreement. Radiology. 2003;228:303-
16/18 vaccine. Int J Cancer. 2003;106:896-904. neoplasia. Lancet. 1999;353:857-859. 308.
3. Mandelblatt JS, Lawrence WF, Gaffikin L, et al. Costs 12. Wright TC Jr, Schiffman M, Solomon D, et al. In- 20. Denny L, Kuhn L, Pollack A, Wainwright H, Wright
and benefits of different strategies to screen for cer- terim guidance for the use of human papillomavirus TC Jr. Evaluation of alternative methods of cervical can-
vical cancer in less-developed countries. J Natl Can- DNA testing as an adjunct to cervical cytology for cer screening for resource-poor settings. Cancer. 2000;
cer Inst. 2002;94:1469-1483. screening. Obstet Gynecol. 2004;103:304-309. 89:826-833.
4. Ferlay J, Parkin D, Pisani D. GLOBOCAN: Cancer 13. Wright TC Jr. Chapter 10: cervical cancer screen- 21. Wright TC Jr, Denny L, Kuhn L, Pollack A, Lorincz
Incidence and Mortality Worldwide. Lyon, France: ing using visualization techniques. J Natl Cancer Inst A. HPV DNA testing of self-collected vaginal samples
International Agency for Research on Cancer; 1998. Monogr. 2003;31:66-71. compared with cytologic screening to detect cervical
5. Miller AB. Cervical Cancer Screening Pro- 14. Denny L, Kuhn L, Pollack A, Wright TC Jr. Direct cancer. JAMA. 2000;283:81-86.
grammes: Managerial Guidelines. Geneva, Switzer- visual inspection for cervical cancer screening: an analy- 22. Greenland S. Applications of stratified analysis
land: World Health Organization; 1992. sis of factors influencing test performance. Cancer. methods. In: Rothman KJ, Greenland S, eds. Modern
6. Ferenczy A. Screening techniques for cervical 2002;94:1699-1707. Epidemiology. 2nd ed. Philadelphia, Pa: Lippincott-
cancer: the next century. Int J Gynecol Cancer. 1996; 15. Syndromic case management of sexually trans- Raven; 1998:286-287.
2:14-21. mitted diseases: a guide for decision makers, health 23. Sankaranarayanan R, Basu P, Wesley RS, et al. Ac-
7. Richart RM. Screening: the next century. Cancer. care workers, and communicators. Presented at: World curacy of visual screening for cervical neoplasia: re-
1995;76:1919-1927. Health Organization Conference; January 24, 2005; sults from an IARC multicentre study in India and Africa.
8. Wright TC Jr, Cox JT, Massad LS, Twiggs LB, Wilkin- New York, NY. Int J Cancer. 2004;110:907-913.
son EJ. 2001 consensus guidelines for the manage- 16. Sellors JW, Jeronimo J, Sankaranarayanan R, et al. 24. Jha P, Mills A, Hanson K, et al. Improving the health
ment of women with cervical cytological abnormalities. Assessment of the cervix after acetic acid wash: inter- of the global poor. Science. 2002;295:2036-2039.
JAMA. 2002;287:2120-2129. rater agreement using photographs. Obstet Gynecol. 25. Rohan TE, Burk RD, Franco EL. Toward a reduc-
9. Gaffikin L, Blumenthal PD, Emerson M, Lim- 2002;99:635-640. tion of the global burden of cervical cancer. Am J Ob-
paphayom K. Safety, acceptability, and feasibility of 17. Ferris D, Cox T, Wright C, O’Connor D. Modern stet Gynecol. 2003;189:S37-S39.
a single-visit approach to cervical-cancer prevention Colposcopy. Hagerstown, Md: American Society of 26. Monsonego J, Bosch FX, Coursaget P, et al. Cer-
in rural Thailand: a demonstration project. Lancet. 2003; Colposcopy and Cervical Pathology; 2005. vical cancer control, priorities and new directions. Int
361:814-820. 18. Wright TC, Ferenczy AF, Kurman RJ. Precancer- J Cancer. 2004;108:329-333.
©2005 American Medical Association. All rights reserved. (Reprinted) JAMA, November 2, 2005—Vol 294, No. 17 2181
Downloaded From: http://jama.jamanetwork.com/ by a New York Medical College User on 10/09/2015
You might also like
- MSQH 5th Edition Standard 06 - Patient and Family Rights-Jan 2017 PDFDocument31 pagesMSQH 5th Edition Standard 06 - Patient and Family Rights-Jan 2017 PDFGarFieLd macHeLoNo ratings yet
- Issuance of Sick Leave Certificate Policy Final - UAEDocument12 pagesIssuance of Sick Leave Certificate Policy Final - UAEmarks2much100% (2)
- Stratethon Case PDFDocument3 pagesStratethon Case PDFRajat YadavNo ratings yet
- TextbookReferenceList MLA 2017Document3 pagesTextbookReferenceList MLA 2017APNo ratings yet
- Assist withambulation- Assist withactivities ofdaily living- To promotehealing- To promoteindependenceDocument2 pagesAssist withambulation- Assist withactivities ofdaily living- To promotehealing- To promoteindependenceDanielJosephLimNo ratings yet
- Culturally Competent Health CareDocument22 pagesCulturally Competent Health CareFrancia ToledanoNo ratings yet
- 329-Article Text-1733-1-10-20211207Document10 pages329-Article Text-1733-1-10-20211207antaresNo ratings yet
- Updates in Cervical Cytology: 90 Years of ProgressDocument11 pagesUpdates in Cervical Cytology: 90 Years of Progressmohamaed abbasNo ratings yet
- Effect of Cervicitis On Visual Inspection With Acetic AcidDocument5 pagesEffect of Cervicitis On Visual Inspection With Acetic AcidmonicamoniccNo ratings yet
- Cervical Screening Essentials GuideDocument7 pagesCervical Screening Essentials Guidedoc moNo ratings yet
- qt5rc2c2s6 NosplashDocument7 pagesqt5rc2c2s6 Nosplashn2763288No ratings yet
- Colposcopy, Cervical Screening, and HPV: A Guide to Prevention and ManagementDocument155 pagesColposcopy, Cervical Screening, and HPV: A Guide to Prevention and ManagementAnnca RoXanna100% (1)
- Green Journal ROMADocument9 pagesGreen Journal ROMAinvestorpatentNo ratings yet
- ACCP Cxca Screening 2011Document8 pagesACCP Cxca Screening 2011Lizeth López LeónNo ratings yet
- 19 - Benefits of Cervical Cancer Screening by Liquid-BasedDocument5 pages19 - Benefits of Cervical Cancer Screening by Liquid-BasedRenan RodriguesNo ratings yet
- Evidence-Based Cervical Cancer Screening for Low-Resource SettingsDocument6 pagesEvidence-Based Cervical Cancer Screening for Low-Resource Settingschica_asNo ratings yet
- PIIS2213398422000902Document7 pagesPIIS2213398422000902Manas BhatiaNo ratings yet
- New England Journal Medicine: The ofDocument10 pagesNew England Journal Medicine: The ofIrena McLaughlinNo ratings yet
- Cervical Cancer Screening With Human Papillomavirus DNA and Cytology in JapanDocument7 pagesCervical Cancer Screening With Human Papillomavirus DNA and Cytology in Japandella kharisma putriNo ratings yet
- Journal ClubDocument60 pagesJournal ClubSataroopa SirigiriNo ratings yet
- Mustafa 2016Document7 pagesMustafa 2016ejigsonNo ratings yet
- Murphy 2008Document8 pagesMurphy 2008Ajup SafarudinNo ratings yet
- Jurnal Onko RiaDocument13 pagesJurnal Onko RiaMuzdatul KhairiahNo ratings yet
- Risk of Ovarian Cancer Algorithm (ROCA) Using Serial CA 125Document9 pagesRisk of Ovarian Cancer Algorithm (ROCA) Using Serial CA 125primadian atnaryanNo ratings yet
- Waggoner 2003Document9 pagesWaggoner 2003behanges71No ratings yet
- HPV Persistent RCTDocument7 pagesHPV Persistent RCTericNo ratings yet
- Performance and Diagnostic Accuracy of A Urine-Based Human Papillomavirus Assay in A Referral PopulationDocument7 pagesPerformance and Diagnostic Accuracy of A Urine-Based Human Papillomavirus Assay in A Referral PopulationJose de PapadopoulosNo ratings yet
- Cervical Conization and The Risk of Preterm DeliveryDocument11 pagesCervical Conization and The Risk of Preterm DeliveryGelo ConcepcionNo ratings yet
- Comparison of Ultrasound and Mammography For Early DiagnosisDocument8 pagesComparison of Ultrasound and Mammography For Early Diagnosishdh1224No ratings yet
- 1-s2.0-S2667005421000053Document8 pages1-s2.0-S2667005421000053Cirugia SolcaNo ratings yet
- CA A Cancer J Clinicians - January February 1998 - Cady - Evaluation of Common Breast Problems Guidance For Primary CareDocument15 pagesCA A Cancer J Clinicians - January February 1998 - Cady - Evaluation of Common Breast Problems Guidance For Primary CareNelson William UsnayoNo ratings yet
- For Personal Use. Only Reproduce With Permission From The LancetDocument10 pagesFor Personal Use. Only Reproduce With Permission From The Lancetzahrah rasyidaNo ratings yet
- CA CerviksDocument6 pagesCA CerviksAzizah NadaNo ratings yet
- SynopsisDocument15 pagesSynopsisnajmulNo ratings yet
- Screening for cervical cancer overviewDocument8 pagesScreening for cervical cancer overviewNike Angela PatriciaNo ratings yet
- Study of Fine Needle Aspiration Cytology of Breast Lump: Correlation of Cytologically Malignant Cases With Their Histological FindingsDocument5 pagesStudy of Fine Needle Aspiration Cytology of Breast Lump: Correlation of Cytologically Malignant Cases With Their Histological FindingsArvind Vashi AroraNo ratings yet
- Artigo Sobre CancerDocument10 pagesArtigo Sobre CancerSérgio Anick da Silva Brito SegundoNo ratings yet
- Cervical Cytology in Women With Abnormal Cervix.: Dr. Veena Rahatgaonkar, Dr. Savita MehendaleDocument4 pagesCervical Cytology in Women With Abnormal Cervix.: Dr. Veena Rahatgaonkar, Dr. Savita MehendaleIOSR Journal of PharmacyNo ratings yet
- Effective Screening10Document4 pagesEffective Screening10ponekNo ratings yet
- HealthLinx Limited PaperDocument10 pagesHealthLinx Limited PapermaikagmNo ratings yet
- Walsh 2005Document7 pagesWalsh 2005Catalin SavinNo ratings yet
- HPV DNA Testing in Cervical Cancer Screening: Results From Women in A High-Risk Province of Costa RicaDocument7 pagesHPV DNA Testing in Cervical Cancer Screening: Results From Women in A High-Risk Province of Costa RicapathologyguruNo ratings yet
- A Retrospective Study Into ShortDocument3 pagesA Retrospective Study Into Shortjanushan05No ratings yet
- Cervical Citology ScreeningDocument12 pagesCervical Citology ScreeningJosé María LauricellaNo ratings yet
- ASCCP Management Guidelines - August 2014 PDFDocument24 pagesASCCP Management Guidelines - August 2014 PDFAnita BlazevskaNo ratings yet
- 1911-Article Text-3239-1-10-20181114Document5 pages1911-Article Text-3239-1-10-20181114drumerNo ratings yet
- Breast CA ScreeningDocument8 pagesBreast CA Screeningchristelm_1No ratings yet
- ACOG 109 Cervical Cytology ScreeningDocument12 pagesACOG 109 Cervical Cytology ScreeningNatalya FlorezNo ratings yet
- nejm乳腺癌Document8 pagesnejm乳腺癌shentujin1997No ratings yet
- Accuracy of Human Papillomavirus Testing On Self Collected Versus Clinician Collected Samples A Meta Analysis PDFDocument12 pagesAccuracy of Human Papillomavirus Testing On Self Collected Versus Clinician Collected Samples A Meta Analysis PDFmarkinfonsecaNo ratings yet
- Nejmoa 2207586Document15 pagesNejmoa 2207586Mirabela CretuNo ratings yet
- Cervical pessary reduces preterm birth in twin pregnancies with short cervixDocument8 pagesCervical pessary reduces preterm birth in twin pregnancies with short cervixjj_cani91No ratings yet
- tmpF425 TMPDocument8 pagestmpF425 TMPFrontiersNo ratings yet
- Proof: Abstracts / Gynecologic Oncology 137 (2015) 591 - 599 598Document1 pageProof: Abstracts / Gynecologic Oncology 137 (2015) 591 - 599 598AripinSyarifudinNo ratings yet
- Follow-Up After Treatment For Cervical Intraepithelial NeoplasiaDocument2 pagesFollow-Up After Treatment For Cervical Intraepithelial NeoplasiaVu Nhat KhangNo ratings yet
- Effective Screening23Document10 pagesEffective Screening23ponekNo ratings yet
- Meijers Heijboer2001Document6 pagesMeijers Heijboer2001Market PlusNo ratings yet
- Trends in Delayed Breast Cancer Diagnosis After ReDocument9 pagesTrends in Delayed Breast Cancer Diagnosis After ReeugeniaNo ratings yet
- Miller Et Al, EEUU 2015Document6 pagesMiller Et Al, EEUU 2015alexsr36No ratings yet
- Thesis Statement On Cervical CancerDocument6 pagesThesis Statement On Cervical Cancerbkx3abyc100% (2)
- Cervical Cancer Screening PDFDocument14 pagesCervical Cancer Screening PDFfahmiNo ratings yet
- Surgery For Cervical Cancer Consensus & ControversiesDocument9 pagesSurgery For Cervical Cancer Consensus & ControversiesmilenahugueninNo ratings yet
- Atypical Breast Proliferative Lesions and Benign Breast DiseaseFrom EverandAtypical Breast Proliferative Lesions and Benign Breast DiseaseFarin AmersiNo ratings yet
- Breast Cancer in Young WomenFrom EverandBreast Cancer in Young WomenOreste GentiliniNo ratings yet
- Lower Genital Tract Precancer: Colposcopy, Pathology and TreatmentFrom EverandLower Genital Tract Precancer: Colposcopy, Pathology and TreatmentNo ratings yet
- Complementary Therapies in MedicineDocument4 pagesComplementary Therapies in MedicineSaddam FuadNo ratings yet
- HHS Public Access: Cognitive Decline and Dementia in Diabetes: Mechanisms and Clinical ImplicationsDocument27 pagesHHS Public Access: Cognitive Decline and Dementia in Diabetes: Mechanisms and Clinical ImplicationsSaddam FuadNo ratings yet
- Intrauterine Fetal TransfusionsDocument10 pagesIntrauterine Fetal TransfusionsSaddam FuadNo ratings yet
- Hypertension and The Risk of Dementia: Cristina SierraDocument7 pagesHypertension and The Risk of Dementia: Cristina SierraSaddam FuadNo ratings yet
- HHS Public Access: Cognitive Decline and Dementia in Diabetes: Mechanisms and Clinical ImplicationsDocument27 pagesHHS Public Access: Cognitive Decline and Dementia in Diabetes: Mechanisms and Clinical ImplicationsSaddam FuadNo ratings yet
- Viapublishedarticle 11 April 2017Document7 pagesViapublishedarticle 11 April 2017Saddam FuadNo ratings yet
- Zhang 2014Document29 pagesZhang 2014Saddam FuadNo ratings yet
- 3 13Document6 pages3 13Muhammad AzkaNo ratings yet
- Breech 5 PDFDocument2 pagesBreech 5 PDFSaddam FuadNo ratings yet
- PAR in Hemostasis 5Document8 pagesPAR in Hemostasis 5Saddam FuadNo ratings yet
- Reviews: Pre-Eclampsia Part 2: Prediction, Prevention and ManagementDocument10 pagesReviews: Pre-Eclampsia Part 2: Prediction, Prevention and Managementdaeng caturNo ratings yet
- Roles of Coagulation Proteases and Pars (Protease-Activated Receptors) in Mouse Models of Inflammatory DiseasesDocument12 pagesRoles of Coagulation Proteases and Pars (Protease-Activated Receptors) in Mouse Models of Inflammatory DiseasesSaddam FuadNo ratings yet
- Thrombin 10 PDFDocument5 pagesThrombin 10 PDFSaddam FuadNo ratings yet
- Impact of Haemostatic Mechanisms On Pathophysiology of Preeclampsia - 2017 - Thrombosis Research PDFDocument5 pagesImpact of Haemostatic Mechanisms On Pathophysiology of Preeclampsia - 2017 - Thrombosis Research PDFfujimeisterNo ratings yet
- Lucena2019 PDFDocument7 pagesLucena2019 PDFSaddam FuadNo ratings yet
- Full-DikonversiDocument9 pagesFull-DikonversiSaddam FuadNo ratings yet
- 5 DikonversiDocument14 pages5 DikonversiSaddam FuadNo ratings yet
- Egan2017 DikonversiDocument15 pagesEgan2017 DikonversiSaddam FuadNo ratings yet
- Egan 2017Document9 pagesEgan 2017Saddam FuadNo ratings yet
- Lucena2019 PDFDocument7 pagesLucena2019 PDFSaddam FuadNo ratings yet
- 5 DikonversiDocument9 pages5 DikonversiSaddam FuadNo ratings yet
- Lockwood2011 DikonversiDocument8 pagesLockwood2011 DikonversiSaddam FuadNo ratings yet
- Aev374 DikonversiDocument14 pagesAev374 DikonversiSaddam FuadNo ratings yet
- Paediatrica IndonesianaDocument8 pagesPaediatrica IndonesianaAnna ClarkNo ratings yet
- General Physical Examination FormDocument4 pagesGeneral Physical Examination Formecint.trmNo ratings yet
- Outline To A Geriatric Medicine Inpatient ConsultationDocument5 pagesOutline To A Geriatric Medicine Inpatient ConsultationEllieNo ratings yet
- Monoclonal Antibody AvailabilityDocument2 pagesMonoclonal Antibody AvailabilityAnonymous GF8PPILW5No ratings yet
- Bethlehem Abhaya Bhavan: Mar Elias College, KottappadyDocument26 pagesBethlehem Abhaya Bhavan: Mar Elias College, KottappadySHARAN SASINo ratings yet
- Wa0005.Document2 pagesWa0005.schauhal69No ratings yet
- Introduction To PharmacotherapeuticsDocument49 pagesIntroduction To PharmacotherapeuticsChandraprakash JadhavNo ratings yet
- The Other Diabetes - LADA, or Type 1Document3 pagesThe Other Diabetes - LADA, or Type 1rey_fremyNo ratings yet
- Law and OrderDocument37 pagesLaw and OrderJOHN CARLO YADAONo ratings yet
- Recovery Room Transfer SheetDocument1 pageRecovery Room Transfer SheetDr. Sumit Kumbhar0% (1)
- IM Case ReportDocument5 pagesIM Case ReportGurungSurajNo ratings yet
- Oral Healthcare For The Pre-School ChildrenDocument43 pagesOral Healthcare For The Pre-School ChildrenMohd Syazuwan Mohd JamilNo ratings yet
- Dian Medisa, Hady Anshory, Putri Litapriani, Rezky Fajriyati MDocument9 pagesDian Medisa, Hady Anshory, Putri Litapriani, Rezky Fajriyati MNada LathifahNo ratings yet
- Module 1 Community Health NursingDocument12 pagesModule 1 Community Health NursingZanesville Lymont L. SubidoNo ratings yet
- BNSL-043 Block-1 PDFDocument136 pagesBNSL-043 Block-1 PDFbhoopesh100% (3)
- Biomecánica Del Cierre de Espacios Mediante La Aplicación de Los Sistemas de La Técnica MBTDocument5 pagesBiomecánica Del Cierre de Espacios Mediante La Aplicación de Los Sistemas de La Técnica MBTAmelia ChuriónNo ratings yet
- JURNALDocument64 pagesJURNALSaleh AlsadiNo ratings yet
- Acute Appendicitis of The Appendiceal StumpDocument3 pagesAcute Appendicitis of The Appendiceal StumpXavier JarrínNo ratings yet
- Temple Foot and Ankle Institute Diabetic Foot Cheat SheetDocument2 pagesTemple Foot and Ankle Institute Diabetic Foot Cheat SheetAkash ShahNo ratings yet
- The Process of ConceptionDocument62 pagesThe Process of ConceptionKaren Ivy BacsainNo ratings yet
- Assessment of satisfaction among complete denture wearersDocument7 pagesAssessment of satisfaction among complete denture wearersVinod ViswanathanNo ratings yet
- Lutman 2015Document11 pagesLutman 2015Moisés AarónNo ratings yet
- Emirates MedicDocument3 pagesEmirates Medicvivalavida148No ratings yet
- InfertilitasDocument6 pagesInfertilitasmasdipoNo ratings yet
- Current Trends in Nursing AdministrationDocument50 pagesCurrent Trends in Nursing AdministrationGeorge Michael LimNo ratings yet