You might also like
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Manage Personal Work Priorities and Professional DevelopmentDocument5 pagesManage Personal Work Priorities and Professional Developmentgurpreet dhillonNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- PD19 - Assignment 3 - Career Exploration: Interviewee and ObjectivesDocument3 pagesPD19 - Assignment 3 - Career Exploration: Interviewee and ObjectivesggyygesyNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Assignment: Personality DevelopmentDocument7 pagesAssignment: Personality Developmentcharanjit kaurNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Leadership and Student Development TheoryDocument16 pagesLeadership and Student Development TheoryEric RuelleNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Lesson 7 - Entrepreneurial-LeadershipDocument6 pagesLesson 7 - Entrepreneurial-LeadershipMarc Loui RiveroNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Homosexualty and The Christian - Mark A YarhouseDocument34 pagesHomosexualty and The Christian - Mark A YarhouseEduardo100% (2)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Đề Ks Tiên Du 1 - Lớp 10 (4 Mã)Document16 pagesĐề Ks Tiên Du 1 - Lớp 10 (4 Mã)Nguyễn PhươngNo ratings yet
- Making The Team 5th Edition Leigh Thompson Test Bank 1Document6 pagesMaking The Team 5th Edition Leigh Thompson Test Bank 1claire100% (56)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Developmental Model of Intercultural SensitivityDocument26 pagesDevelopmental Model of Intercultural Sensitivitymary engNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Understand Women Better Digital Ebook OxvbnpDocument114 pagesUnderstand Women Better Digital Ebook Oxvbnpbutterflybee247No ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Functional Group Communication TheoryDocument5 pagesFunctional Group Communication TheoryAndreeaFugaruNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Vocabulary Instruction: Wake Robin Elementary August 13, 2010Document15 pagesVocabulary Instruction: Wake Robin Elementary August 13, 2010kingsley4No ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
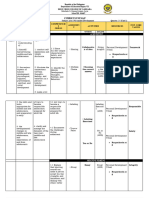
- Grade 11 Per Dev Curriculum Map Unit 1Document4 pagesGrade 11 Per Dev Curriculum Map Unit 1Christel Joy De San PedroNo ratings yet
- Impact of Homework Assignment On Students' Learning: ArticleDocument20 pagesImpact of Homework Assignment On Students' Learning: ArticleDilara ÇivicioğluNo ratings yet
- Resume Updated May 2017Document3 pagesResume Updated May 2017api-361492094No ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Social Psychology OficialDocument28 pagesSocial Psychology OficialMichelle SophiaNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- ACR 2022 Preliminary ProgramDocument5 pagesACR 2022 Preliminary ProgramPete BristolNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Educ 5210 Written Assignment Unit 3Document4 pagesEduc 5210 Written Assignment Unit 3Tejumade MusahNo ratings yet
- Forensic Psychiatry-2: LT Col Sandeep Bansal Dept of Forensic Medicine & ToxicologyDocument54 pagesForensic Psychiatry-2: LT Col Sandeep Bansal Dept of Forensic Medicine & ToxicologySandeep BansalNo ratings yet
- BrochureDocument2 pagesBrochureapi-277611497No ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Adversity Quotient: Paul G. Stoltz, PHDDocument14 pagesAdversity Quotient: Paul G. Stoltz, PHDjaja c.No ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Assignment 5Document3 pagesAssignment 5Muhammad Ali100% (1)
- Total Old Final Paper Mgt501Document78 pagesTotal Old Final Paper Mgt501Syed Faisal Bukhari0% (1)
- Understanding Cross-Cultural Management: Part ThreeDocument20 pagesUnderstanding Cross-Cultural Management: Part ThreeSanjana GaneshNo ratings yet
- Rubric S For Art AppreciationDocument7 pagesRubric S For Art AppreciationshindigzsariNo ratings yet
- Self-Control and Grit: Related But Separable Determinants of SuccessDocument8 pagesSelf-Control and Grit: Related But Separable Determinants of SuccessDhea RantyNo ratings yet
- Frofed 3 FullDocument30 pagesFrofed 3 FullRoxas Marry GraceNo ratings yet
- Capstone Project Final DraftDocument6 pagesCapstone Project Final Draftapi-551049953No ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Ge6075 Scad MSM PDFDocument89 pagesGe6075 Scad MSM PDFlogamaniNo ratings yet
- Research Methalogy of Project FileDocument15 pagesResearch Methalogy of Project FileAbhishek ChoudharyNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)