You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (843)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Cabin Crew ManualDocument626 pagesCabin Crew ManualBilly Eres93% (29)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Motivation Statement Talent Scouting UI Revised 1Document2 pagesMotivation Statement Talent Scouting UI Revised 1Dennis Pranata100% (2)
- Hamlet Act 2 2 Part 5Document2 pagesHamlet Act 2 2 Part 5api-240934338No ratings yet
- SM7 Ch05 DistributionDocument36 pagesSM7 Ch05 DistributionMayank SharmaNo ratings yet
- LABREL 6th WEEKDocument54 pagesLABREL 6th WEEKSometimes goodNo ratings yet
- Dilation - FormalDocument14 pagesDilation - Formalapi-355095027No ratings yet
- Mehndi Zaveri (For Debo)Document2 pagesMehndi Zaveri (For Debo)vipin HNo ratings yet
- Succession Planning Case Study: © The Talent Company Ltd. 2013Document1 pageSuccession Planning Case Study: © The Talent Company Ltd. 2013Rekha SainiNo ratings yet
- Design and Fabrication of Rocker Bogie Mechanism Geosurvey RoverDocument7 pagesDesign and Fabrication of Rocker Bogie Mechanism Geosurvey RovershivaNo ratings yet
- Crossing Functional LinesDocument7 pagesCrossing Functional LinesmanmeetassignmentNo ratings yet
- 05 Barriers To Communication UNIT 4Document15 pages05 Barriers To Communication UNIT 4Arun PrasadNo ratings yet
- CSTP 2 Bermudez 1210Document9 pagesCSTP 2 Bermudez 1210Brenda BermudezNo ratings yet
- Investigation and Prosecution)Document8 pagesInvestigation and Prosecution)Baishnavi ShahNo ratings yet
- Human Resource Management Performance Evaluation ProcessDocument3 pagesHuman Resource Management Performance Evaluation ProcessJohn Michael MejillanoNo ratings yet
- Sustainable-Responsible Tourism Discourse - Towards Responsustable' TourismDocument11 pagesSustainable-Responsible Tourism Discourse - Towards Responsustable' TourismamalNo ratings yet
- Intro To Marketing Primer 158Document158 pagesIntro To Marketing Primer 158fchavarria7No ratings yet
- Rup Vs ScrumDocument9 pagesRup Vs ScrumMehdi AmiriNo ratings yet
- Certification of ComplianceDocument1 pageCertification of ComplianceSanFabian Pangasinan Bfp RegionOneNo ratings yet
- Writing Task 1Document34 pagesWriting Task 1Nguyên BảoNo ratings yet
- Huntingfield Pony & Riding Club Inc PreDocument4 pagesHuntingfield Pony & Riding Club Inc Preapi-26187582No ratings yet
- Versant English Placement Test Practice Materials: 1. Predicting ContentDocument18 pagesVersant English Placement Test Practice Materials: 1. Predicting ContentMelike Erdem100% (1)
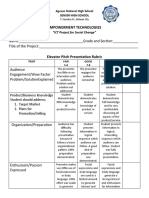
- Elevator Pitch Rubrics (ICT For Social Chnage)Document2 pagesElevator Pitch Rubrics (ICT For Social Chnage)Dran OteroNo ratings yet
- Accomplishment Report of DEWORMING ORIENTATIONDocument3 pagesAccomplishment Report of DEWORMING ORIENTATIONGeraldin Joy Dela Cruz100% (1)
- Energy Modelling Guidelines (British Columbia) PDFDocument42 pagesEnergy Modelling Guidelines (British Columbia) PDFSchreiber_DiesesNo ratings yet
- Sales and Distribution Management: Mba II Year I SemesterDocument35 pagesSales and Distribution Management: Mba II Year I SemesterY ARUN KUMARNo ratings yet
- ME-6703-Computer Integrated Manufacturing: Unit-IDocument8 pagesME-6703-Computer Integrated Manufacturing: Unit-IJayakrishnaNo ratings yet
- Salmorin Daniel Emmanuel Venturanza, Aklan State UniversityDocument5 pagesSalmorin Daniel Emmanuel Venturanza, Aklan State UniversityRenwen LataNo ratings yet
- Cover PageDocument9 pagesCover PageFania Brace AnnNo ratings yet
- 12 WI FormworkDocument9 pages12 WI FormworkSafdar AliNo ratings yet
- Carter Case 1: Q. Make A List of Five Specific HR Problems You Think Carter Cleaning Will Have To Grapple WithDocument2 pagesCarter Case 1: Q. Make A List of Five Specific HR Problems You Think Carter Cleaning Will Have To Grapple WithNitesh Mehla100% (1)