You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Modifications To A 3d-Printed Temporal Bone Model For Augmented Stapes Fixation Surgery TeachingDocument7 pagesModifications To A 3d-Printed Temporal Bone Model For Augmented Stapes Fixation Surgery TeachingAdarsh GhoshNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Three-Dimensional Assessment of The Temporal Bone and Mandible Deformations in Patients With Congenital Aural AtresiaDocument3 pagesThree-Dimensional Assessment of The Temporal Bone and Mandible Deformations in Patients With Congenital Aural AtresiaAdarsh GhoshNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Pancreatic Duct TextureDocument9 pagesPancreatic Duct TextureAdarsh GhoshNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Radiol 2019182354Document9 pagesRadiol 2019182354Adarsh GhoshNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Dural Opening/Removal For Combined Petrosal Approach: Technical NoteDocument5 pagesDural Opening/Removal For Combined Petrosal Approach: Technical NoteWilson Quispe AlanocaNo ratings yet
- Personal Development Module 7Document51 pagesPersonal Development Module 7Allinatsoc Reverof Nylia75% (4)
- McKenzie LumbarDocument51 pagesMcKenzie LumbarRouqia HamedNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Pfeiffer 2003Document10 pagesPfeiffer 2003maria eugenia gonzalezNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Asymmetrical Hearing Loss: Jessica PrasadDocument6 pagesAsymmetrical Hearing Loss: Jessica PrasadSujaya ChattopadhyayNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Neuro - ICPDocument24 pagesNeuro - ICPcseNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Bhramari PranayamaDocument6 pagesBhramari PranayamaDASI Susanto100% (1)
- Labs Final NaDocument5 pagesLabs Final NaKenRodulfReyesVillaruelNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Diabetic Neuropathy PDFDocument10 pagesDiabetic Neuropathy PDFMellody YudhashintaNo ratings yet
- Colour Vision - NajwaDocument52 pagesColour Vision - NajwaNajwa MansuriNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Neurofilament Light Chain Gaetani2019Document12 pagesNeurofilament Light Chain Gaetani2019eastareaNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Numbers: Name NH ALDocument23 pagesNumbers: Name NH ALRuang IlmuNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Co Ordination NotesDocument57 pagesCo Ordination Notesbipin jainNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Anatomy of The Eye WorksheetDocument1 pageAnatomy of The Eye WorksheetIrfan ArifNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
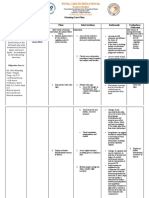
- Nursing Care Plan: by The Wife During InterviewDocument3 pagesNursing Care Plan: by The Wife During InterviewJayson SamonteNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Optic Neuritis - Continuum Noviembre 2019Document29 pagesOptic Neuritis - Continuum Noviembre 2019María Isabel Medina de BedoutNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Chapter 29 The Nervous SystemDocument64 pagesChapter 29 The Nervous SystemAugustus Czar De LeonNo ratings yet
- Anxiety GAD ACSAP 2017 StudentDocument18 pagesAnxiety GAD ACSAP 2017 StudentRenaldi KristianNo ratings yet
- Ho 22-1 & 22-2Document2 pagesHo 22-1 & 22-2Sierra SeabraNo ratings yet
- Diagnostic Criteria For Posttraumatic Stress Disorder: Table 5.7Document1 pageDiagnostic Criteria For Posttraumatic Stress Disorder: Table 5.7Marial JavierNo ratings yet
- Book Reading FetomaternalDocument27 pagesBook Reading FetomaternalpipitNo ratings yet
- Piracetam and Piracetam Like Drugs From Basic.4Document26 pagesPiracetam and Piracetam Like Drugs From Basic.4jsoriano6No ratings yet
- Learning Objectives of Neuroanatomy For Undergraduate Medicine: A Delphi ProcessDocument10 pagesLearning Objectives of Neuroanatomy For Undergraduate Medicine: A Delphi ProcessNOVALIA ROZA -No ratings yet
- The Neurological Exam: Mental Status ExaminationDocument13 pagesThe Neurological Exam: Mental Status ExaminationShitaljit IromNo ratings yet
- Bipolar PowerpointDocument10 pagesBipolar PowerpointRAYMIND MIRANDANo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The EctodermDocument30 pagesThe EctodermRey Bonnin Gonzaga NaparanNo ratings yet
- Perceptual Pleasure and The Brain by Irving Biederman & Edward VesselDocument8 pagesPerceptual Pleasure and The Brain by Irving Biederman & Edward VesselAmiraNo ratings yet
- Brown Sequard SindromDocument6 pagesBrown Sequard Sindromida maryaniNo ratings yet
- J.A. Gray's Reinforcement Sensitivity Theory (RST) of PersonalityDocument18 pagesJ.A. Gray's Reinforcement Sensitivity Theory (RST) of PersonalityZoran RapaicNo ratings yet
- OET Writing Letter SampleDocument2 pagesOET Writing Letter Sampledrdk10% (1)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)