You might also like
- How Banks Create MoneyDocument28 pagesHow Banks Create MoneyMathew Beniga Gaco100% (1)
- OBLICON Super ReviewerDocument110 pagesOBLICON Super ReviewerStefan Salvator81% (16)
- Incompetent Cervix Case Analysis Subgroup 2Document44 pagesIncompetent Cervix Case Analysis Subgroup 2bunso padillaNo ratings yet
- The Process Flowchart at Arnold Palmer HospitalDocument3 pagesThe Process Flowchart at Arnold Palmer HospitalherrajohnNo ratings yet
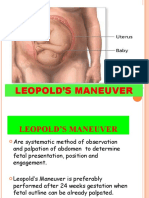
- Leopolds and FetalDocument7 pagesLeopolds and Fetaltyche100% (1)
- Bubble He AssessmentDocument9 pagesBubble He AssessmentMaryjoy RegaspiNo ratings yet
- Diabetes in Pregnancy: Supervisor: DR Rathimalar By: DR Ashwini Arumugam & DR Laily MokhtarDocument21 pagesDiabetes in Pregnancy: Supervisor: DR Rathimalar By: DR Ashwini Arumugam & DR Laily MokhtarHarleyquinn96 DrNo ratings yet
- Corporation Law Case DigestDocument488 pagesCorporation Law Case DigestKaizer Dave93% (43)
- Leopold's ManeuverDocument22 pagesLeopold's ManeuverArlene Cerdeña Salceda100% (1)
- Problems With The PassengerDocument65 pagesProblems With The Passengermark Orpilla100% (1)
- Client With High-RiskDocument170 pagesClient With High-RiskLongyapon Sheena Stephanie100% (2)
- Partograph: Jillian A. Bejoc, MSN, RNDocument44 pagesPartograph: Jillian A. Bejoc, MSN, RNJiezl Abellano AfinidadNo ratings yet
- Nursing Care of The Client With High-Risk Labor & DeliveryDocument10 pagesNursing Care of The Client With High-Risk Labor & DeliveryWilbert CabanbanNo ratings yet
- Midterm Notes On NCM 109 EditedDocument10 pagesMidterm Notes On NCM 109 EditedJohn Fred100% (2)
- Essential Intrapartum AND Newborn Care By: Heidi C. Cabanatan, RNDocument20 pagesEssential Intrapartum AND Newborn Care By: Heidi C. Cabanatan, RNThrecia RotaNo ratings yet
- Delivery Room RequirementsDocument12 pagesDelivery Room RequirementsHannah Ros Quitorio IINo ratings yet
- Incompetent CervixDocument29 pagesIncompetent CervixCyrelle Jen TorresNo ratings yet
- Incompetent CervixDocument4 pagesIncompetent CervixCharm Arroyo100% (1)
- Gestational AgeDocument6 pagesGestational AgemhuniswellNo ratings yet
- Intrapartal ComplicationsDocument5 pagesIntrapartal ComplicationsJeremiah JustoNo ratings yet
- Components of LaborDocument5 pagesComponents of LaborJeraldine Lindo100% (4)
- Maternal Quiz 2Document24 pagesMaternal Quiz 2Aaron ConstantinoNo ratings yet
- Theories of Labor OnsetDocument7 pagesTheories of Labor OnsetBogaloid100% (6)
- Roles and Responsibility As A Nurse in Delivery RoomDocument6 pagesRoles and Responsibility As A Nurse in Delivery RoomMay 마이100% (8)
- Complications During Labor and Delivery - HardDocument19 pagesComplications During Labor and Delivery - Hardkrizele ann santosNo ratings yet
- High Risk Pregnancy Review QuestionsDocument59 pagesHigh Risk Pregnancy Review Questionsmitted100% (1)
- Einc ReviewerDocument4 pagesEinc ReviewerEricson Candelaria0% (1)
- PROBLEMS of THE PASSAGEWAY and PsycheDocument1 pagePROBLEMS of THE PASSAGEWAY and PsycheAirishNo ratings yet
- Complications With The Power of LaborDocument8 pagesComplications With The Power of LaborEdrea Aquino MendezNo ratings yet
- Hydatidiform MoleDocument2 pagesHydatidiform MoleDaniele Katrina Pimentel100% (3)
- Obstetric Sample Questions With RationaleDocument31 pagesObstetric Sample Questions With RationaleTomzki Cornelio50% (2)
- Prelim NCM 109 Lecture HandoutsDocument21 pagesPrelim NCM 109 Lecture HandoutsLillabin71% (7)
- MCN QuizDocument6 pagesMCN QuizMÖna Macaranas100% (5)
- Bubbleshe Assessment: BREASTS 1. Palpate Both Breasts ForDocument3 pagesBubbleshe Assessment: BREASTS 1. Palpate Both Breasts Forallyssa joyNo ratings yet
- Prolonged LabourDocument47 pagesProlonged LabourBharat ThapaNo ratings yet
- Chapter 21: Nursing Care of A Family Experiencing A Sudden Pregnancy ComplicationDocument9 pagesChapter 21: Nursing Care of A Family Experiencing A Sudden Pregnancy ComplicationAlyssaGrandeMontimor100% (1)
- Concept of Unitive and Procreative HealthDocument5 pagesConcept of Unitive and Procreative HealthDONITA DALUMPINESNo ratings yet
- Assisting and Handling Normal Delivery - Return DemoDocument3 pagesAssisting and Handling Normal Delivery - Return Demornrmmanphd100% (1)
- Notes On Obstetrics: Normal Labor (Theories of Labor Onset)Document22 pagesNotes On Obstetrics: Normal Labor (Theories of Labor Onset)Jobelle Acena100% (1)
- 9 Labor and DeliveryDocument6 pages9 Labor and DeliveryUri Perez MontedeRamosNo ratings yet
- Iii. Textbook Discussion A. Definition: Predisposing Factors Precipitating FactorsDocument3 pagesIii. Textbook Discussion A. Definition: Predisposing Factors Precipitating FactorsVianne Arcenio100% (1)
- Nursing Care of The Postpartum ClientDocument13 pagesNursing Care of The Postpartum ClientLyca Mae AurelioNo ratings yet
- Uterine RuptureDocument19 pagesUterine RuptureAna Denise Quinajon0% (1)
- Rizal ReflectionDocument6 pagesRizal ReflectionMathew Beniga Gaco100% (5)
- Problems of The PassengerDocument9 pagesProblems of The PassengerDanah Grace SanchezNo ratings yet
- Labor Midterm Case DigestsDocument183 pagesLabor Midterm Case Digestschacile100% (2)
- Navigation-2: (Terrestrial and Coastal Navigation-2)Document3 pagesNavigation-2: (Terrestrial and Coastal Navigation-2)Mathew Beniga Gaco50% (2)
- Passageway and Power Lesson 2: Problems With The PassagewayDocument3 pagesPassageway and Power Lesson 2: Problems With The PassagewayFatmah Sarah CornellNo ratings yet
- CPD PathophysiologyDocument3 pagesCPD PathophysiologyTeanne Bathan100% (1)
- Internal Examination: Prepared By: Lester D. Bongabong BSN Ii - BDocument9 pagesInternal Examination: Prepared By: Lester D. Bongabong BSN Ii - BJustine Cagatan100% (1)
- Problems With The PowersDocument5 pagesProblems With The PowersAlexander Ruiz Queddeng100% (1)
- NCM 109N: Frameworks For Maternal & Child Health NursingDocument37 pagesNCM 109N: Frameworks For Maternal & Child Health NursingZudota100% (1)
- Physical Assessment of Normal Pregnant ClientDocument24 pagesPhysical Assessment of Normal Pregnant ClientGhilah MaeNo ratings yet
- Intrapartal - Theories of LaborDocument21 pagesIntrapartal - Theories of LaborJan Oliver YaresNo ratings yet
- Discharge Planning FinalDocument5 pagesDischarge Planning FinalRose AnnNo ratings yet
- CASE ANALYSIS Ectopic Pregnancy Part 1Document10 pagesCASE ANALYSIS Ectopic Pregnancy Part 1Diane Celine SantianoNo ratings yet
- Intrapartum QuestionsDocument24 pagesIntrapartum QuestionsAnonymous ZduHBgNo ratings yet
- Normal Spontaneous Delivery NSD (EINC)Document2 pagesNormal Spontaneous Delivery NSD (EINC)Mhel MGNo ratings yet
- The PartographDocument45 pagesThe PartographKimsha ConcepcionNo ratings yet
- InstrumentsDocument7 pagesInstrumentsOllet Athive NatacabNo ratings yet
- The Woman Who Develops Complications During Labor and BirthDocument55 pagesThe Woman Who Develops Complications During Labor and BirthVincent Maralit MaterialNo ratings yet
- Abnormal LaborDocument10 pagesAbnormal LaborZechariah NicholasNo ratings yet
- CPD, Dystocia, Fetal Distress OutputDocument8 pagesCPD, Dystocia, Fetal Distress OutputJohn Dave AbranNo ratings yet
- Case Management For LTCS For Non-Reassure Fetal StatutsDocument3 pagesCase Management For LTCS For Non-Reassure Fetal StatutsSarah Ann Jamilla FaciolanNo ratings yet
- Types of Fetal DystociaDocument3 pagesTypes of Fetal DystociaDella FerginaNo ratings yet
- Birth InjuriesDocument9 pagesBirth InjuriesshailaNo ratings yet
- Definition: Related Diagnostic TestsDocument8 pagesDefinition: Related Diagnostic TestsQuinn Xylon VillanuevaNo ratings yet
- Prolonged LabourDocument12 pagesProlonged Labourhacker ammerNo ratings yet
- Saint Joseph Institute of Technology: Bio-DataDocument1 pageSaint Joseph Institute of Technology: Bio-DataMathew Beniga GacoNo ratings yet
- Labasan Vs LacuestaDocument2 pagesLabasan Vs LacuestaMathew Beniga GacoNo ratings yet
- Art. 114. Treason.: ElementsDocument3 pagesArt. 114. Treason.: ElementsMathew Beniga GacoNo ratings yet
- Saint Joseph Institute of TechnologyDocument1 pageSaint Joseph Institute of TechnologyMathew Beniga GacoNo ratings yet
- English Important in SeamanDocument1 pageEnglish Important in SeamanMathew Beniga GacoNo ratings yet
- Chamber of Real Estate and Builders Associations, Inc., v. The Hon. Executive Secretary Alberto Romulo, Et AlDocument6 pagesChamber of Real Estate and Builders Associations, Inc., v. The Hon. Executive Secretary Alberto Romulo, Et AlMathew Beniga GacoNo ratings yet
- English Proficiency Test (Ept)Document3 pagesEnglish Proficiency Test (Ept)Mathew Beniga GacoNo ratings yet
- Cayetano Vs MonsodDocument31 pagesCayetano Vs MonsodMathew Beniga GacoNo ratings yet
- Computer 1: Computer Application and NetworkingDocument32 pagesComputer 1: Computer Application and NetworkingMathew Beniga GacoNo ratings yet
- El Nino and La NinaDocument9 pagesEl Nino and La NinaMathew Beniga GacoNo ratings yet
- Geographic Coordinate: Latitude - Is ADocument2 pagesGeographic Coordinate: Latitude - Is AMathew Beniga GacoNo ratings yet
- The River's Merchants Wife: A Letter Li Tai PoDocument8 pagesThe River's Merchants Wife: A Letter Li Tai PoMathew Beniga GacoNo ratings yet
- B.A TabulationsDocument13 pagesB.A TabulationsMathew Beniga GacoNo ratings yet
- Money and BankingDocument21 pagesMoney and BankingMathew Beniga GacoNo ratings yet
- Sample FormatDocument128 pagesSample FormatMathew Beniga Gaco100% (1)
- CR Poli Obs 11-05-18 EditDocument133 pagesCR Poli Obs 11-05-18 EditRyan IlhamNo ratings yet
- Problems With The PassageDocument13 pagesProblems With The PassageMaria Theresa BuscasNo ratings yet
- Breech 17Document27 pagesBreech 17Trevor Uratel100% (1)
- Latihan Soal Chapter XVDocument15 pagesLatihan Soal Chapter XVDEWI WULANDARI KONTJE100% (1)
- Maternity Magazine 2012 - 2013 PDFDocument212 pagesMaternity Magazine 2012 - 2013 PDFMaria Carolina LowenNo ratings yet
- LRDR ProceduresDocument67 pagesLRDR ProceduresJustJ ThingsNo ratings yet
- Silabus KDK Dengan MingguDocument24 pagesSilabus KDK Dengan MingguIin Prima FitriahNo ratings yet
- Minimal Stimulation IVF Vs Conventional IVFDocument8 pagesMinimal Stimulation IVF Vs Conventional IVFpolygoneNo ratings yet
- Physiology of Lactation: Prepared By: Fy MSC NursingDocument32 pagesPhysiology of Lactation: Prepared By: Fy MSC NursingSùjâl PätídàrNo ratings yet
- Fraternal TwinsDocument4 pagesFraternal TwinsjovinerNo ratings yet
- International Journal of Health Sciences and ResearchDocument7 pagesInternational Journal of Health Sciences and ResearchTabrani. ZANo ratings yet
- Birth and Emergency Plan: Learning Objectives: at The End of This Procedure, Students Are Expected ToDocument3 pagesBirth and Emergency Plan: Learning Objectives: at The End of This Procedure, Students Are Expected ToArjay EllaNo ratings yet
- Asuhan Kebidanan Pada NyD Usia Kehamilan 37 MingguDocument8 pagesAsuhan Kebidanan Pada NyD Usia Kehamilan 37 MingguNur NilaNo ratings yet
- (Patho OB) Dystocia Due To Abnormalities in Power and Passage-Dr. Ahyong-Reyes (Bernabe)Document5 pages(Patho OB) Dystocia Due To Abnormalities in Power and Passage-Dr. Ahyong-Reyes (Bernabe)Shia LevyNo ratings yet
- Normal LabourDocument55 pagesNormal LabourSalshabilNo ratings yet
- Individual Maternal and Child Health Case Study: Saint Mary's UniversityDocument5 pagesIndividual Maternal and Child Health Case Study: Saint Mary's UniversityCarelle Faith Serrano AsuncionNo ratings yet
- Surat Penugasan KlinisDocument13 pagesSurat Penugasan KlinisSischa Afriyani PasaribuNo ratings yet
- Intrauterine Fetal Demise: Care in The Aftermath, and BeyondDocument5 pagesIntrauterine Fetal Demise: Care in The Aftermath, and BeyondPinanggih ReviNo ratings yet
- 47 Review Article - Sushmitha Ramona KarkadaDocument4 pages47 Review Article - Sushmitha Ramona KarkadaAnjali Rahul AjmeriNo ratings yet
- Breastfeeding and Complementary FeedingDocument20 pagesBreastfeeding and Complementary FeedingJohn Christian LasalitaNo ratings yet
- SurrogacyDocument16 pagesSurrogacyBhavna FirozNo ratings yet
- ESSAY TOPIC NITA FinalDocument3 pagesESSAY TOPIC NITA FinalwideriNo ratings yet
- WHO Partograph Study Lancet 1994Document6 pagesWHO Partograph Study Lancet 1994Dewi PradnyaNo ratings yet
- PC-BSC-N 1st YearDocument6 pagesPC-BSC-N 1st YearrithushivaNo ratings yet
- Tanggal JAM Nama Umur PembiayaanDocument53 pagesTanggal JAM Nama Umur PembiayaanEdward SuryadiNo ratings yet
- Mode of Delivery and Persistence of Pelvic Girdle Syndrome 6 Months PostpartumDocument20 pagesMode of Delivery and Persistence of Pelvic Girdle Syndrome 6 Months PostpartumDanil ArmandNo ratings yet
- Sistem Pengurusan Kualiti: Jadual Pengajaran TerperinciDocument3 pagesSistem Pengurusan Kualiti: Jadual Pengajaran TerperinciNurul IrhamnaNo ratings yet
- Partograph EditedDocument54 pagesPartograph EditedNathaniel PulidoNo ratings yet