You might also like
- Community Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCommunity Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- 5 Nursing Diagnoses and Interventions for HypertensionDocument7 pages5 Nursing Diagnoses and Interventions for Hypertensionmelerine16No ratings yet
- Cardiac Rehab After CABGDocument31 pagesCardiac Rehab After CABGShefali SharmaNo ratings yet
- Ineffective Breathing Pattern Related To Acute Pain As Evidence by Increased RespirationDocument6 pagesIneffective Breathing Pattern Related To Acute Pain As Evidence by Increased RespirationCamille T. SanchezNo ratings yet
- Case StudyDocument34 pagesCase StudyBSNNursing101No ratings yet
- Impaired Tissue PerfusionDocument2 pagesImpaired Tissue PerfusionLyka Mae Imbat - PacnisNo ratings yet
- NCPDocument15 pagesNCPCamille PinedaNo ratings yet
- Managing Diabetes and RisksDocument8 pagesManaging Diabetes and RisksChristopher LontocNo ratings yet
- Nursing Care Plan EportfolioDocument14 pagesNursing Care Plan Eportfolioapi-279212367No ratings yet
- Nursing Care PlanDocument14 pagesNursing Care PlanVin Landicho100% (1)
- Nursing Care Plan FinalDocument16 pagesNursing Care Plan FinalErickson OcialNo ratings yet
- Nursing Care Plan WeeblyDocument8 pagesNursing Care Plan Weeblyapi-277498943No ratings yet
- Hypertension Nursing Care PlanDocument2 pagesHypertension Nursing Care PlanCj LowryNo ratings yet
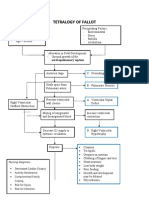
- Tetralogy of Fallot Pathophysiology & Risk FactorsDocument1 pageTetralogy of Fallot Pathophysiology & Risk FactorsEiztirfNo ratings yet
- Case Stydy Angina PectorisDocument46 pagesCase Stydy Angina PectorissharenNo ratings yet
- Decreased Cardiac OutputDocument4 pagesDecreased Cardiac OutputAdnan Khan100% (1)
- DM & DI ExamsDocument11 pagesDM & DI ExamsTomzki CornelioNo ratings yet
- St. Anthony's College Nursing Department Patient Care Plan for S.LDocument2 pagesSt. Anthony's College Nursing Department Patient Care Plan for S.LAirme Raz AlejandroNo ratings yet
- PD Case Study: 68yo FemaleDocument9 pagesPD Case Study: 68yo FemaleMary Rose Ponte FernandezNo ratings yet
- Assessment Nursing Diagnosis Planning Interventions EvaluationsDocument4 pagesAssessment Nursing Diagnosis Planning Interventions EvaluationsAjay SupanNo ratings yet
- CP Intestinal Obstruction Nursing Care PlanDocument7 pagesCP Intestinal Obstruction Nursing Care PlanShiella Heart MalanaNo ratings yet
- Hypovolemic Shock Concept MapDocument1 pageHypovolemic Shock Concept MapJM AsentistaNo ratings yet
- Upper Gastro Intestinal BleedingDocument11 pagesUpper Gastro Intestinal BleedingSyima MnnNo ratings yet
- Nursing Care Plan for Hypertension ManagementDocument5 pagesNursing Care Plan for Hypertension Managementbhavana100% (1)
- Meddical Care Study Part 1Document48 pagesMeddical Care Study Part 1christyNo ratings yet
- Intracranial HemorrhageDocument41 pagesIntracranial Hemorrhagedoctormussieaberra100% (1)
- NCP Blood Glucose Imbalance 4thDocument2 pagesNCP Blood Glucose Imbalance 4thRainier IbarretaNo ratings yet
- Cardiac MonitorDocument5 pagesCardiac MonitorhumbertolgeNo ratings yet
- Nursing Care PlanDocument6 pagesNursing Care Planesteffie21No ratings yet
- NCP GbsDocument2 pagesNCP GbsJaylord VerazonNo ratings yet
- PericarditisDocument45 pagesPericarditisBrenda WardshoneNo ratings yet
- Nursing Care PlanDocument4 pagesNursing Care PlanJobelyn TunayNo ratings yet
- NCP Meningitis Sure NaniDocument2 pagesNCP Meningitis Sure NaniARISNo ratings yet
- Medication ThalassemiaDocument3 pagesMedication ThalassemiaDivya ToppoNo ratings yet
- Care for Thoracic Aortic AneurysmDocument67 pagesCare for Thoracic Aortic AneurysmJonathan DiazNo ratings yet
- Nursing Care Plan for Pre-operative AnxietyDocument1 pageNursing Care Plan for Pre-operative AnxietyVoid LessNo ratings yet
- Hypertension Nursing Care PlanDocument3 pagesHypertension Nursing Care PlanAsylla PajijiNo ratings yet
- Acute Respiratory Distress SyndromeDocument40 pagesAcute Respiratory Distress SyndromeDavid Seroney100% (1)
- Chest Pain Care PlanDocument2 pagesChest Pain Care Planapi-545292605No ratings yet
- Diabetic KetoacidosisDocument41 pagesDiabetic KetoacidosisdenekeNo ratings yet
- Scientific Explanation of Expected Outcomes and InterventionsDocument4 pagesScientific Explanation of Expected Outcomes and InterventionsGensen Cu RoxasNo ratings yet
- Acute Renal Failure Nursing Care PlanDocument15 pagesAcute Renal Failure Nursing Care PlanRanusha AnushaNo ratings yet
- Managing Fever in a Child with PoliomyelitisDocument4 pagesManaging Fever in a Child with PoliomyelitisMonica RamboyongNo ratings yet
- Cardiac Tamponade 2Document23 pagesCardiac Tamponade 2Jethro Floyd QuintoNo ratings yet
- Incomplete Spinal Cord Injury Nursing CareDocument6 pagesIncomplete Spinal Cord Injury Nursing CareTherese MargaretNo ratings yet
- Case CHFDocument10 pagesCase CHFAgnes Erlita Distriani Patade50% (2)
- Congestive Cardiac FailureDocument49 pagesCongestive Cardiac FailureHampson MalekanoNo ratings yet
- Decreased Cardiac Output FinalDocument2 pagesDecreased Cardiac Output FinalSandraDeeNo ratings yet
- Manage Bronchiectasis Nursing Care PlanDocument5 pagesManage Bronchiectasis Nursing Care PlanPaola Marie VenusNo ratings yet
- BibliographyDocument10 pagesBibliographySourav Kumar PatraNo ratings yet
- HyperthermiaDocument2 pagesHyperthermiaLeolene Grace BautistaNo ratings yet
- NCP2 - DengueDocument4 pagesNCP2 - DengueSummer SuarezNo ratings yet
- Tetralogy of Fallot Nursing Diagnosis and ManagementDocument2 pagesTetralogy of Fallot Nursing Diagnosis and ManagementKarl KiwisNo ratings yet
- Rufino, Leslie Kriztel S. BSN 3-2 Group 1Document6 pagesRufino, Leslie Kriztel S. BSN 3-2 Group 1Deinielle Magdangal RomeroNo ratings yet
- Nursing Care Plan for Fluid Volume DeficitDocument9 pagesNursing Care Plan for Fluid Volume DeficitYesha Mae MartinNo ratings yet
- Nursing Diagnosis For Coronary Artery Disease - Acute PainDocument2 pagesNursing Diagnosis For Coronary Artery Disease - Acute PainAngie Mandeoya100% (1)
- Caring for TB Patients Using Orem's TheoryDocument13 pagesCaring for TB Patients Using Orem's TheoryRazel Kinette AzotesNo ratings yet
- Medical Diagnosis: Bronchial Asthma Impaired Gas ExchangeDocument2 pagesMedical Diagnosis: Bronchial Asthma Impaired Gas ExchangeAndrea Chua BuadoNo ratings yet
- Reynaud's DiseaseDocument13 pagesReynaud's Diseasezebzeb STEMANo ratings yet
- CHF Simulation PreparationDocument5 pagesCHF Simulation Preparation5Dragoon5No ratings yet
- Concept of MGTDocument5 pagesConcept of MGTmerin sunilNo ratings yet
- Faculty WelfareDocument6 pagesFaculty Welfaremerin sunilNo ratings yet
- Evaluation of PersonnelDocument7 pagesEvaluation of Personnelmerin sunil100% (2)
- Future Direction of NursingDocument4 pagesFuture Direction of Nursingmerin sunil100% (1)
- DisciplineDocument11 pagesDisciplineAnusha Verghese100% (5)
- Communication VIDocument7 pagesCommunication VImerin sunilNo ratings yet
- Cost Accounting & Effectiveness For Nursing PracticeDocument6 pagesCost Accounting & Effectiveness For Nursing Practicemerin sunilNo ratings yet
- Nursing Staff Estimation TechniquesDocument16 pagesNursing Staff Estimation Techniquesmerin sunil100% (4)
- DisciplineDocument11 pagesDisciplineAnusha Verghese100% (5)
- Gambling Addiction Among Adolescents 2375 4494 1000e121Document2 pagesGambling Addiction Among Adolescents 2375 4494 1000e121merin sunilNo ratings yet
- Combined NotesDocument373 pagesCombined Notesmerin sunil0% (1)
- Buget For School of NSGDocument6 pagesBuget For School of NSGmerin sunilNo ratings yet
- Health Administration at The Centre and State LevelDocument22 pagesHealth Administration at The Centre and State Levelmerin sunilNo ratings yet
- Intro NeurologyDocument64 pagesIntro Neurologymerin sunilNo ratings yet
- Recommendations For Inpatient Psychiatric Treatment For Suicidal Adolescents 1522 4821 1000290 PDFDocument2 pagesRecommendations For Inpatient Psychiatric Treatment For Suicidal Adolescents 1522 4821 1000290 PDFmerin sunilNo ratings yet
- Substance AbuseDocument45 pagesSubstance AbuseKimberly Anne SP Padilla100% (1)
- Intervention Approaches For Children With Autism Spectrum Disorder Asd and Attention Hyperactivity Disorder Adhd Review of Researc 2375 4494 1000369Document6 pagesIntervention Approaches For Children With Autism Spectrum Disorder Asd and Attention Hyperactivity Disorder Adhd Review of Researc 2375 4494 1000369merin sunil100% (1)
- Heart FailureDocument29 pagesHeart Failuremerin sunilNo ratings yet
- A Descriptive Study To Assess The Level of Internet Addiction Among Adolescents A Case Study of High Schools in Mangalore 2375 4494 1000378Document9 pagesA Descriptive Study To Assess The Level of Internet Addiction Among Adolescents A Case Study of High Schools in Mangalore 2375 4494 1000378merin sunilNo ratings yet
- Disaster Mental Health and Crisis Interventions 1522 4821 17 E179Document1 pageDisaster Mental Health and Crisis Interventions 1522 4821 17 E179merin sunilNo ratings yet
- J Lucas KoberdaDocument30 pagesJ Lucas Koberdamerin sunilNo ratings yet
- Recommendations For Inpatient Psychiatric Treatment For Suicidal Adolescents 1522 4821 1000290 PDFDocument2 pagesRecommendations For Inpatient Psychiatric Treatment For Suicidal Adolescents 1522 4821 1000290 PDFmerin sunilNo ratings yet
- Seminar ON: Cardiomyopat HYDocument43 pagesSeminar ON: Cardiomyopat HYmerin sunilNo ratings yet
- Quality Assurance in Nursing SeminarDocument29 pagesQuality Assurance in Nursing Seminarmerin sunilNo ratings yet
- Seminar ON Cardiopulmonary Resuscitation: Submitted To Submitted byDocument18 pagesSeminar ON Cardiopulmonary Resuscitation: Submitted To Submitted bymerin sunilNo ratings yet
- Quick Start Guide for SanDisk SecureAccessDocument21 pagesQuick Start Guide for SanDisk SecureAccessbijan034567No ratings yet
- RESPIRATORY FAILUREnewDocument26 pagesRESPIRATORY FAILUREnewmerin sunilNo ratings yet
- Appendix F Section A-Demographic Variables InstructionsDocument12 pagesAppendix F Section A-Demographic Variables Instructionsmerin sunilNo ratings yet
- Appendix eDocument1 pageAppendix emerin sunilNo ratings yet
- Appendix H Content On Mental HygieneDocument25 pagesAppendix H Content On Mental Hygienemerin sunilNo ratings yet
- CORDERO Performance Task 5Document1 pageCORDERO Performance Task 5Maria Hilda Vicio AragonNo ratings yet
- Uterine Rupture and Cervical TearDocument16 pagesUterine Rupture and Cervical Tearsangita patil0% (1)
- Eric Thorhauer CVDocument7 pagesEric Thorhauer CVapi-251923314No ratings yet
- МартDocument55 pagesМартLuisAngelPonceTorresNo ratings yet
- Teeth EssayDocument3 pagesTeeth EssayKazeNo ratings yet
- Hiv AidsDocument472 pagesHiv AidsDevendrapratapdpNo ratings yet
- Procedural Sedation in The ED: - Myths and MethodsDocument37 pagesProcedural Sedation in The ED: - Myths and MethodsSteven RossNo ratings yet
- Annotated Bibliography of Obstetrics & Gynaecology ResourcesDocument4 pagesAnnotated Bibliography of Obstetrics & Gynaecology ResourcesKaku ManishaNo ratings yet
- American Journal of Emergency MedicineDocument7 pagesAmerican Journal of Emergency MedicineVirgi AgustiaNo ratings yet
- Group 1Document41 pagesGroup 1SELEMAYE ZENEBENo ratings yet
- Admit List PG 2nd Counselling 2013Document113 pagesAdmit List PG 2nd Counselling 2013gautambobNo ratings yet
- Data PersonilDocument74 pagesData Personilpanji_208No ratings yet
- Journal Heptojugular RefluxDocument5 pagesJournal Heptojugular RefluxFarhan RezaNo ratings yet
- Nclex New Lastest 1Document240 pagesNclex New Lastest 1Nadim KhalidNo ratings yet
- Clinical Study of Otomycosis: Fungal Ear Infection Causes, Symptoms & TreatmentDocument16 pagesClinical Study of Otomycosis: Fungal Ear Infection Causes, Symptoms & TreatmentMcraeNo ratings yet
- Assessing The Relationship Between Anxiety Levels and Panic Attacks Among The Youth in ShimlaDocument52 pagesAssessing The Relationship Between Anxiety Levels and Panic Attacks Among The Youth in ShimlaAni RudhNo ratings yet
- By Dr. Nouran Abou Khedr: Xeroderma PigmentosumDocument6 pagesBy Dr. Nouran Abou Khedr: Xeroderma PigmentosumBahaa ShaabanNo ratings yet
- Frequency Specific MicrocurrentDocument2 pagesFrequency Specific MicrocurrentAngela Pagliuso50% (2)
- Understanding Pheochromocytoma: Etiology, Diagnosis and TreatmentDocument1 pageUnderstanding Pheochromocytoma: Etiology, Diagnosis and TreatmentJulie-Thuy Nguyen100% (1)
- Shigella SPP, Vibrio SPPDocument6 pagesShigella SPP, Vibrio SPPtomal7811islamNo ratings yet
- Diabetic Medicine - 2022 - Dhatariya - The Management of Diabetic Ketoacidosis in Adults An Updated Guideline From TheDocument20 pagesDiabetic Medicine - 2022 - Dhatariya - The Management of Diabetic Ketoacidosis in Adults An Updated Guideline From Thenguyenngocanh9798No ratings yet
- Preeclampsia SFlt-1-PlGF Ratio - Pocket CardDocument2 pagesPreeclampsia SFlt-1-PlGF Ratio - Pocket CardRajeev PareekNo ratings yet
- Bulbena CAbretalCNPS2016 PDFDocument11 pagesBulbena CAbretalCNPS2016 PDFLucero Corrales HuamánNo ratings yet
- DR Eva Detko Why You Can T Have A Healthy Gut Without Good Vagus FunctionDocument16 pagesDR Eva Detko Why You Can T Have A Healthy Gut Without Good Vagus Functioncharanmann9165100% (1)
- Escherichia ColiDocument31 pagesEscherichia ColiLizzie Fizzie100% (1)
- The Child With A Fluid and Electrolyte Alteration: Body Water Is Located in Two Major CompartmentsDocument19 pagesThe Child With A Fluid and Electrolyte Alteration: Body Water Is Located in Two Major CompartmentsAyeza DuaNo ratings yet
- OBA Medical QuestionsDocument9 pagesOBA Medical QuestionsishafaraNo ratings yet
- NURS 6521N Final Exam Question and Answers Feb 2020 (100/100)Document19 pagesNURS 6521N Final Exam Question and Answers Feb 2020 (100/100)Judy Durkin0% (1)
- Hemorrhoidectomy: Prepared By: Kristine Anne M. Lacorte BSN Iii-CDocument13 pagesHemorrhoidectomy: Prepared By: Kristine Anne M. Lacorte BSN Iii-CRita Honrade HernandezNo ratings yet
- 29 - Toronto Notes 2011 - Urology PDFDocument44 pages29 - Toronto Notes 2011 - Urology PDFDewa Gede Reza Sanjaya0% (1)