You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- ECG QuizDocument3 pagesECG QuizRonnie LimNo ratings yet
- Strategies, Techniques, Approaches To Critical Thinking A Clinical Reasoning Workbook For Nurses, 5e by Sandra Luz Martinez de Castillo EdD RN PDFDocument287 pagesStrategies, Techniques, Approaches To Critical Thinking A Clinical Reasoning Workbook For Nurses, 5e by Sandra Luz Martinez de Castillo EdD RN PDFJ1525% (8)
- NAC Protocol PrintableDocument21 pagesNAC Protocol Printablemaadyyy123100% (1)
- Nervous SystemDocument40 pagesNervous SystemNabeel Uddin100% (1)
- HKDSE Biology Part 3 Health & DiseasesDocument17 pagesHKDSE Biology Part 3 Health & DiseasesTSZ YAN CHEUNGNo ratings yet
- Lung Cancer (Nursing Care)Document5 pagesLung Cancer (Nursing Care)heiyuNo ratings yet
- Blood Transfusion Protocols in NeonatesDocument12 pagesBlood Transfusion Protocols in NeonatesSupriya M A SuppiNo ratings yet
- Elvis Presley PPM Article 44 55 - A Case of Disabling Head TraumaDocument14 pagesElvis Presley PPM Article 44 55 - A Case of Disabling Head TraumaJustin100% (1)
- Blood TypingDocument34 pagesBlood Typingaurezea100% (1)
- Retinal Vascular Diseas E: Christine Anne D. EspejaDocument25 pagesRetinal Vascular Diseas E: Christine Anne D. EspejaPaolo QuezonNo ratings yet
- Behçet DiseaseDocument17 pagesBehçet DiseasePaolo QuezonNo ratings yet
- Multifetal GestationDocument22 pagesMultifetal GestationPaolo QuezonNo ratings yet
- Ovulation and Menstration: Hormone ActionDocument4 pagesOvulation and Menstration: Hormone ActionPaolo QuezonNo ratings yet
- Polycystic Ovarian SyndromeDocument2 pagesPolycystic Ovarian SyndromePaolo QuezonNo ratings yet
- ABO Blood GroupingsDocument11 pagesABO Blood GroupingsPaolo QuezonNo ratings yet
- Prevalence and Associated Risk Factors of Urinary Tract Infections in Pregnant Women Admitted On Maternity Ward in Jinja Regional Referral HospitalDocument10 pagesPrevalence and Associated Risk Factors of Urinary Tract Infections in Pregnant Women Admitted On Maternity Ward in Jinja Regional Referral HospitalKIU PUBLICATION AND EXTENSIONNo ratings yet
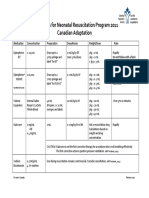
- Medications For Neonatal Resuscitation Program 2011 Canadian AdaptationDocument1 pageMedications For Neonatal Resuscitation Program 2011 Canadian AdaptationrubymayNo ratings yet
- Large CystDocument4 pagesLarge CystKin DacikinukNo ratings yet
- Discharge InstructionDocument3 pagesDischarge Instructionolive oilNo ratings yet
- Journal 9Document15 pagesJournal 9Muhammad FaisalNo ratings yet
- Anthropometrics Measurement 1 1Document7 pagesAnthropometrics Measurement 1 1Quencee CalaycayNo ratings yet
- Chapter 24 (Digestive System) Chapter 24 (Digestive System)Document30 pagesChapter 24 (Digestive System) Chapter 24 (Digestive System)Pranali BasuNo ratings yet
- CR 110520Document14 pagesCR 110520genellemaarteNo ratings yet
- Hand HygieneDocument11 pagesHand HygieneAllan M Murray-doNo ratings yet
- LAS HEALTH 6 Q4 Wk5 Cherlyn. RonquilloDocument4 pagesLAS HEALTH 6 Q4 Wk5 Cherlyn. RonquilloANGELINA RAMBOYONGNo ratings yet
- Arachnoid Cyst: From Wikipedia, The Free EncyclopediaDocument11 pagesArachnoid Cyst: From Wikipedia, The Free EncyclopediaOsama Bin RizwanNo ratings yet
- P LCR Parameter Platelet Large Cell Ratio Medical Laboratories PDFDocument3 pagesP LCR Parameter Platelet Large Cell Ratio Medical Laboratories PDFluxsura8217No ratings yet
- Program Studi Bimbingan Dan Konseling IKIP Siliwangi: Sitifatimah432@ikipsiliwangi - Ac.idDocument11 pagesProgram Studi Bimbingan Dan Konseling IKIP Siliwangi: Sitifatimah432@ikipsiliwangi - Ac.idHazimatus Sa'diyahNo ratings yet
- VA Hospital ChargesDocument11 pagesVA Hospital ChargesAnna MooreNo ratings yet
- Womens Self-Management of AsthmaDocument24 pagesWomens Self-Management of AsthmaCenter for Managing Chronic DiseaseNo ratings yet
- Barriers To Exclusive Breastfeeding Among Urban Mothers: Original ArticleDocument5 pagesBarriers To Exclusive Breastfeeding Among Urban Mothers: Original ArticleEno RLNo ratings yet
- Dexmedetomidine FAQDocument16 pagesDexmedetomidine FAQRoxana SurliuNo ratings yet
- Carpal TunnelDocument1 pageCarpal TunnelKadek Rudita YasaNo ratings yet
- Assessment of Pediatric Dental Guidelines in The post-COVID 19 PeriodDocument14 pagesAssessment of Pediatric Dental Guidelines in The post-COVID 19 PeriodCha AlegriaNo ratings yet
- Blood Vessels QuestionsDocument7 pagesBlood Vessels QuestionsT-Jay Ellis-DaleNo ratings yet
- Hospital Diet and Oral Nutritional Supplements (Sip Feeds)Document16 pagesHospital Diet and Oral Nutritional Supplements (Sip Feeds)Patrick nyawiraNo ratings yet