You might also like
- Medical Appeal 3Document3 pagesMedical Appeal 3George French100% (2)
- Estate of Gerardo Gutierrez vs. PublixDocument12 pagesEstate of Gerardo Gutierrez vs. PublixPeterBurkeNo ratings yet
- Consensus Recommendations For The Management of Constipation in Patients With Advanced, Progressive IllnessDocument13 pagesConsensus Recommendations For The Management of Constipation in Patients With Advanced, Progressive IllnessRahmida Rahmy100% (1)
- Clinical Nutrition: ESPEN GuidelineDocument18 pagesClinical Nutrition: ESPEN GuidelineMariana RodriguesNo ratings yet
- ASPEN NutritionDocument18 pagesASPEN Nutritionsilvio da costa guerreiroNo ratings yet
- Pain ManagementDocument55 pagesPain ManagementJahangaiz KhanNo ratings yet
- EASL Clinical Practice Guidelines for the Management of Hepatocellular CarcinomaDocument55 pagesEASL Clinical Practice Guidelines for the Management of Hepatocellular CarcinomaAgam ChekmatNo ratings yet
- Acidosis MetabólicaDocument17 pagesAcidosis MetabólicaYuri CamachoNo ratings yet
- Blake Et Al 2011 Clinical Practice Guidelines and Recommendations On Peritoneal Dialysis Adequacy 2011Document22 pagesBlake Et Al 2011 Clinical Practice Guidelines and Recommendations On Peritoneal Dialysis Adequacy 2011Gema CanalesNo ratings yet
- Manejo EstreñimientolarkinDocument12 pagesManejo EstreñimientolarkinJaimeNo ratings yet
- Adequcy of HDDocument22 pagesAdequcy of HDzulfiqarNo ratings yet
- Consensus Guidelines For Enhanced Recovery After GastrectomyDocument21 pagesConsensus Guidelines For Enhanced Recovery After GastrectomyEloy BurdaNo ratings yet
- Bruix Et Al 2005 HepatologyDocument29 pagesBruix Et Al 2005 Hepatologymow 3bbasNo ratings yet
- 1 Cutting Edge InformationDocument5 pages1 Cutting Edge InformationJuanCk7No ratings yet
- Guidelines For The Choice of Intravenous Fluids For Vascular FillingDocument10 pagesGuidelines For The Choice of Intravenous Fluids For Vascular FillingAntonio RamirezNo ratings yet
- Guidelines For Perioperative Care For Pancreaticoduodenectomy WJSDocument19 pagesGuidelines For Perioperative Care For Pancreaticoduodenectomy WJSFelipe BerbertNo ratings yet
- Guideline Adekuasi ISPD 2020Document10 pagesGuideline Adekuasi ISPD 2020Laurencia ViolettaNo ratings yet
- Berger-Monitoreo Nutricional en UCI-2018Document10 pagesBerger-Monitoreo Nutricional en UCI-2018Brayan AuntaNo ratings yet
- RespDocument2 pagesRespNicolaeDincaNo ratings yet
- Management of The Major Complications of Cirrhosis BeyondDocument12 pagesManagement of The Major Complications of Cirrhosis BeyondBryan TorresNo ratings yet
- European Society of Neurogastroenterology and Motility Guidelines On Functional Constipation in AdultsDocument33 pagesEuropean Society of Neurogastroenterology and Motility Guidelines On Functional Constipation in AdultsOuerdia HATEMNo ratings yet
- International Society For Peritoneal Dialysis Practice Recommendations: Prescribing High-Quality Goal-Directed Peritoneal DialysisDocument10 pagesInternational Society For Peritoneal Dialysis Practice Recommendations: Prescribing High-Quality Goal-Directed Peritoneal DialysisMade Dedy KusnawanNo ratings yet
- European ConstipationDocument33 pagesEuropean ConstipationambulatNo ratings yet
- WJH 8 1075Document13 pagesWJH 8 1075Rengganis PutriNo ratings yet
- Masonetal - alimentPharmacolTher20052191135 43Document9 pagesMasonetal - alimentPharmacolTher20052191135 43Riefka Ananda ZulfaNo ratings yet
- Gallstone Pancreatitis Management ChallengesDocument6 pagesGallstone Pancreatitis Management ChallengeskartikapuspitNo ratings yet
- Point-Of-Care Gastric Ultrasound and Aspiration Risk Assessment - A Narrative Review PDFDocument12 pagesPoint-Of-Care Gastric Ultrasound and Aspiration Risk Assessment - A Narrative Review PDFJohana FuentesNo ratings yet
- Consensus Guidelines For The Management of Chronic Pelvic PainDocument41 pagesConsensus Guidelines For The Management of Chronic Pelvic PaindubblewalkerNo ratings yet
- Acupuncture For Constipation in Patients With Stroke: Protocol of A Systematic Review and Meta-AnalysisDocument5 pagesAcupuncture For Constipation in Patients With Stroke: Protocol of A Systematic Review and Meta-AnalysisYUTRILIANo ratings yet
- Management of The Critically Ill Patient With Severe Acute Pancreatitis SCCM ATS 2004Document13 pagesManagement of The Critically Ill Patient With Severe Acute Pancreatitis SCCM ATS 2004Alexis May UcNo ratings yet
- Perioperative Care in Elective Colonic Surgery ERASDocument18 pagesPerioperative Care in Elective Colonic Surgery ERASBeatriz MDNo ratings yet
- Appraisal: And-Youth-5-17Document1 pageAppraisal: And-Youth-5-17tuio2002No ratings yet
- Rochwerg2020 Article TheRoleForHighFlowNasalCannulaDocument12 pagesRochwerg2020 Article TheRoleForHighFlowNasalCannulaminiypuntoNo ratings yet
- Guidelines for Managing Intra-Abdominal InfectionsDocument14 pagesGuidelines for Managing Intra-Abdominal InfectionsNguyễn Mạnh CườngNo ratings yet
- Endoscopic Management of Common Bile Duct Stones: European Society of Gastrointestinal Endoscopy (ESGE) GuidelineDocument64 pagesEndoscopic Management of Common Bile Duct Stones: European Society of Gastrointestinal Endoscopy (ESGE) GuidelineIrina GîrleanuNo ratings yet
- PR DR Coana - IntanArdylaMDocument140 pagesPR DR Coana - IntanArdylaMAnnisa Tria FadillaNo ratings yet
- 2 ESPEN-ESPGHAN-ECFS Guidelines On Nutrition Care For Infants Children and Adults With Cystic FibrosisDocument21 pages2 ESPEN-ESPGHAN-ECFS Guidelines On Nutrition Care For Infants Children and Adults With Cystic FibrosisAmany SalamaNo ratings yet
- Guia Canadience Uso de Mallas VaginalesDocument13 pagesGuia Canadience Uso de Mallas VaginalesGiuliana Cuadros PeñalozaNo ratings yet
- ESWL For CholelithiasisDocument25 pagesESWL For CholelithiasisKhildaZakiyyahSa'adahNo ratings yet
- Initial Evaluation and Referral Guidelines For Management of Pelvic Ovarian MassesDocument6 pagesInitial Evaluation and Referral Guidelines For Management of Pelvic Ovarian Massesjhon heriansyahNo ratings yet
- Constipation For CancerDocument15 pagesConstipation For Cancerpalomazul007No ratings yet
- Pancreatitis GuidelineDocument26 pagesPancreatitis GuidelineShalltear BloodfallenNo ratings yet
- Acupoint Catgut Embedding Therapy For FunctionalDocument5 pagesAcupoint Catgut Embedding Therapy For FunctionalJuan Pablo MejíaNo ratings yet
- 1 - Manejo de ColangitisDocument29 pages1 - Manejo de ColangitisMarielos RodriguezNo ratings yet
- GASTRO REVIEWS: CHRONIC CONSTIPATIONDocument18 pagesGASTRO REVIEWS: CHRONIC CONSTIPATIONZul najmiNo ratings yet
- Clinical Practice Recommendations For The Management of Bowel ObstructionDocument11 pagesClinical Practice Recommendations For The Management of Bowel ObstructionThiago GomesNo ratings yet
- DCR 2016 Constipation, Evaluation and Management ofDocument14 pagesDCR 2016 Constipation, Evaluation and Management ofrisewfNo ratings yet
- European Society For Vascular Surgery (ESVS) 2019 Clinical Practice Guidelines On The Management of Abdominal Aorto-Iliac Artery AneurysmDocument75 pagesEuropean Society For Vascular Surgery (ESVS) 2019 Clinical Practice Guidelines On The Management of Abdominal Aorto-Iliac Artery AneurysmNazliah SyarbinNo ratings yet
- Clinical NutritionDocument12 pagesClinical NutritionBagus Candra BuanaNo ratings yet
- Nutrition in Pancreatic Surg ISGPS 2018Document14 pagesNutrition in Pancreatic Surg ISGPS 2018Dr Ankit SharmaNo ratings yet
- Tokyo Guidelines Establish Diagnostic Criteria for Acute Cholangitis and CholecystitisDocument4 pagesTokyo Guidelines Establish Diagnostic Criteria for Acute Cholangitis and CholecystitisEduardo Martinez AvilaNo ratings yet
- Early Management of Severe Abdominal - 2020 - Anaesthesia Critical Care - Pain MDocument9 pagesEarly Management of Severe Abdominal - 2020 - Anaesthesia Critical Care - Pain MRicardoNo ratings yet
- Guidelines For Laparoscopic Peritoneal Dialysis Access SurgeryDocument28 pagesGuidelines For Laparoscopic Peritoneal Dialysis Access SurgeryIgnatia Rosalia KiranaNo ratings yet
- Bjs 11429Document10 pagesBjs 11429Pablo García HumérezNo ratings yet
- Lectura 3 - Algoritmo de Movilización Temprana.Document18 pagesLectura 3 - Algoritmo de Movilización Temprana.PilarSolanoPalominoNo ratings yet
- J Parenter Enteral Nutr - 2022 - Barhorst - Implementation of A Best Practice Guideline Early Enteral Nutrition in ADocument5 pagesJ Parenter Enteral Nutr - 2022 - Barhorst - Implementation of A Best Practice Guideline Early Enteral Nutrition in AROBERTO CARLOS BLANQUICETT CORTINANo ratings yet
- Philippine Clinical Practice Guidelines For The Management of Gout 2008Document7 pagesPhilippine Clinical Practice Guidelines For The Management of Gout 2008JedNo ratings yet
- Meta AnalysisDocument6 pagesMeta AnalysisGemala AdillawatyNo ratings yet
- Consenso Italiano PA SeveraDocument70 pagesConsenso Italiano PA SeveraFabrizzio BardalesNo ratings yet
- Top Trials in Gastroenterology & HepatologyFrom EverandTop Trials in Gastroenterology & HepatologyRating: 4.5 out of 5 stars4.5/5 (7)
- Management of Peritoneal Metastases- Cytoreductive Surgery, HIPEC and BeyondFrom EverandManagement of Peritoneal Metastases- Cytoreductive Surgery, HIPEC and BeyondAditi BhattNo ratings yet
- Cme SG Guidelines BPHDocument8 pagesCme SG Guidelines BPHTonny ChenNo ratings yet
- ATA Guidelines for Diagnosis and Management of HyperthyroidismDocument79 pagesATA Guidelines for Diagnosis and Management of Hyperthyroidismmod_naiveNo ratings yet
- Consenso Europeo Tep 2014Document48 pagesConsenso Europeo Tep 2014lbritez7No ratings yet
- Cme SG Guidelines BPHDocument8 pagesCme SG Guidelines BPHTonny ChenNo ratings yet
- Antithrombotic Therapy For VTE Disease CHEST Guideline Feb 2016Document38 pagesAntithrombotic Therapy For VTE Disease CHEST Guideline Feb 2016Effy AngeLi LomocsoNo ratings yet
- Umbral TerapéuticoDocument9 pagesUmbral Terapéuticolbritez7No ratings yet
- Conjuntivitis AlérgicaDocument13 pagesConjuntivitis Alérgicalbritez7No ratings yet
- DROGADICCIÓNDocument7 pagesDROGADICCIÓNlbritez7No ratings yet
- Gold 2018Document142 pagesGold 2018histoginoNo ratings yet
- Interstitial Pna AutoimmuneDocument12 pagesInterstitial Pna AutoimmuneFranco PacelloNo ratings yet
- HDB GuíaDocument11 pagesHDB Guíalbritez7No ratings yet
- Fibrosis PulmonarDocument58 pagesFibrosis Pulmonarlbritez7No ratings yet
- HipotiroidimoDocument82 pagesHipotiroidimodroswaldo88No ratings yet
- Guias de Manejo Inicial de La Pancreatitis AGA 2018Document6 pagesGuias de Manejo Inicial de La Pancreatitis AGA 2018Vivi AlburezNo ratings yet
- Pancreatitis Aguda Guías ClínicasDocument1 pagePancreatitis Aguda Guías Clínicaslbritez7No ratings yet
- Apendicitis AgudaDocument17 pagesApendicitis Agudalbritez7No ratings yet
- Pancreatitis Aguda Atlanta 2012Document10 pagesPancreatitis Aguda Atlanta 2012lbritez7No ratings yet
- Acute AbdomenDocument36 pagesAcute AbdomenDayita Quishpe100% (1)
- DISFAGIA ConcensoDocument9 pagesDISFAGIA Concensolbritez7No ratings yet
- Clinical Course Discussion: Oregon Health & Science University, Portland, OregonDocument1 pageClinical Course Discussion: Oregon Health & Science University, Portland, OregonperjadanutNo ratings yet
- Podcast Script "Hustle Culture" OPENING: Haiii I'am Hidayah Malika and Welcome To Speak Up' PodcastDocument3 pagesPodcast Script "Hustle Culture" OPENING: Haiii I'am Hidayah Malika and Welcome To Speak Up' PodcastMas'adatul HidayahNo ratings yet
- Discharge PlanDocument2 pagesDischarge PlanHannah ChiuNo ratings yet
- Special Edition E-80 4Document2 pagesSpecial Edition E-80 4Ankit AgarwalNo ratings yet
- Acute Common Carotid Artery Bifurcation ThrombusDocument2 pagesAcute Common Carotid Artery Bifurcation ThrombusChavdarNo ratings yet
- Surgical SeiveDocument28 pagesSurgical SeiveSumeet PratapNo ratings yet
- FNCPDocument4 pagesFNCPJonalyn Tumanguil100% (2)
- Session 10. Review of Centric Records RECORDSDocument25 pagesSession 10. Review of Centric Records RECORDSbaraa.abdulrahman.23No ratings yet
- The Psychodynamic Diagnostic Manual An Effort To Compensate For The Limitations of Descriptive Psychiatric Diagnosis (Mcwilliams2011)Document12 pagesThe Psychodynamic Diagnostic Manual An Effort To Compensate For The Limitations of Descriptive Psychiatric Diagnosis (Mcwilliams2011)Anastasiya PlohihNo ratings yet
- English: Quarter 4 - Module 1: Using Appropriate Grammatical Signals or Expressions To Each Pattern of Idea DevelopmentDocument33 pagesEnglish: Quarter 4 - Module 1: Using Appropriate Grammatical Signals or Expressions To Each Pattern of Idea DevelopmentShiela Tecson Gamayon40% (5)
- KBA Dyslipidemia 2023 Oct 31 TueDocument36 pagesKBA Dyslipidemia 2023 Oct 31 TueKamran B AliNo ratings yet
- Boala CeliacaDocument4 pagesBoala CeliacaCristina TudorNo ratings yet
- 1 - Which Factors Do Provoke Binge Eating An Exploratory Study in Eating Disorder Patients PDFDocument6 pages1 - Which Factors Do Provoke Binge Eating An Exploratory Study in Eating Disorder Patients PDFLaura CasadoNo ratings yet
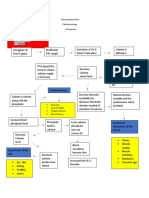
- Hypoparathyroidism PathophysiologyDocument1 pageHypoparathyroidism PathophysiologymaricarNo ratings yet
- Mark Anthony A. Tom, M.D. First Year Internal Medicine Resident Davao Doctors HospitalDocument55 pagesMark Anthony A. Tom, M.D. First Year Internal Medicine Resident Davao Doctors HospitalMark Anthony TomNo ratings yet
- Cram Reviewer MusculoskeletalDocument32 pagesCram Reviewer MusculoskeletalGwynthselle SalazarNo ratings yet
- CariesCare-International Consensus-Manuscript BDJ-corrected 12062019Document13 pagesCariesCare-International Consensus-Manuscript BDJ-corrected 12062019pocket4love4yeahNo ratings yet
- PASCUAL, Jhigo V. REYES, Al Sebastian C. MEDINA, Chris Daniel J. PUSING, Daniel Joseph V. Documentation and Report Humss 11-3 Physical ScienceDocument2 pagesPASCUAL, Jhigo V. REYES, Al Sebastian C. MEDINA, Chris Daniel J. PUSING, Daniel Joseph V. Documentation and Report Humss 11-3 Physical ScienceJhigo Villar Franco PascualNo ratings yet
- Rizal To Paris To GermanyDocument48 pagesRizal To Paris To Germanybenj panganibanNo ratings yet
- Report Public Dialogue Nanotech HealthcareDocument90 pagesReport Public Dialogue Nanotech HealthcareGemerlyn VallesNo ratings yet
- Clobazam As First Add On What Is The Evidence and Experience - Final Deck - 14 Feb 2023Document51 pagesClobazam As First Add On What Is The Evidence and Experience - Final Deck - 14 Feb 2023veerraju tvNo ratings yet
- Reproductive ToxicologyDocument31 pagesReproductive ToxicologyfianceeleeNo ratings yet
- Professional Foundation Level Acupressure Training CourseDocument94 pagesProfessional Foundation Level Acupressure Training CourseLuis Del Valle TorregrosaNo ratings yet
- Baby Thesis RevisedDocument20 pagesBaby Thesis RevisedSanjoe Angelo ManaloNo ratings yet
- Cardiovascular SystemDocument26 pagesCardiovascular SystemRismawatiNo ratings yet
- Achigan-DakoTchokponhoueNDanikouetal 2015Document13 pagesAchigan-DakoTchokponhoueNDanikouetal 2015Juan Pablo Hernandez PaezNo ratings yet
- Addressing Barriers, Stigma and Discrimination Surrounding HIV and Viral HepatitisDocument17 pagesAddressing Barriers, Stigma and Discrimination Surrounding HIV and Viral HepatitisAlemayehu KebedeNo ratings yet
- Risk factors of diabetic retinopathy and vision threatening diabetic retinopathy and vision threatening diabetic retinopaty based on diabetic retinopathy screening program in greater bandung, west java.astriDocument14 pagesRisk factors of diabetic retinopathy and vision threatening diabetic retinopathy and vision threatening diabetic retinopaty based on diabetic retinopathy screening program in greater bandung, west java.astriSi PuputNo ratings yet