You might also like
- Extend XT - Folleto ComercialDocument6 pagesExtend XT - Folleto ComercialMuhamadZuhdiAlWaliNo ratings yet
- Venti Logic LS Venti Logic Plus: Now With MPV Available!Document6 pagesVenti Logic LS Venti Logic Plus: Now With MPV Available!Michael LevitNo ratings yet
- Emax 2 Plus System: User'S ManualDocument60 pagesEmax 2 Plus System: User'S ManualSerkan ÖztürkNo ratings yet
- VP5005 Instruction ManualDocument23 pagesVP5005 Instruction Manualjosuemax30% (2)
- Edan ManualDocument14 pagesEdan ManualTony Nava100% (1)
- Scio Four Family Gas Measurement ModulesDocument6 pagesScio Four Family Gas Measurement Moduleschuong hoNo ratings yet
- Philips Heartstart XL Plus Defibrillator ManualDocument235 pagesPhilips Heartstart XL Plus Defibrillator ManualvikasNo ratings yet
- Carescape R860: Participant GuideDocument142 pagesCarescape R860: Participant GuideМаксим МатяшNo ratings yet
- As/As-V Sealcut: Pouchmaking Machine For The Automatic Production of Flat and Gusseted PouchesDocument6 pagesAs/As-V Sealcut: Pouchmaking Machine For The Automatic Production of Flat and Gusseted PouchesillaNo ratings yet
- Philips - HeartStart XL - User TrainingDocument106 pagesPhilips - HeartStart XL - User TrainingabuNo ratings yet
- Injectomat Tiva AgiliaDocument2 pagesInjectomat Tiva AgiliaswamyNo ratings yet
- Lullaby Bro e PDFDocument4 pagesLullaby Bro e PDFBradda Derru Nesta MarleyNo ratings yet
- Manual Clv-U40Document4 pagesManual Clv-U40Ingrid SanchezNo ratings yet
- IfU Perseus A500 SW 1.1n EN US 9054110Document272 pagesIfU Perseus A500 SW 1.1n EN US 9054110Ruban RajNo ratings yet
- Uzumcu ESuDocument14 pagesUzumcu ESuRizkiana Samarind0% (1)
- Flight 60T Turbine Operating ManualDocument128 pagesFlight 60T Turbine Operating Manualtravieso112No ratings yet
- Saadat (M)Document319 pagesSaadat (M)Erghy Loverzt Sangpencuri Hati100% (1)
- Fukuda UF7700Document2 pagesFukuda UF7700docmonster100% (2)
- DS5000 2014Document2 pagesDS5000 2014Nhật LongNo ratings yet
- Aisys CS2 Spec SheetDocument5 pagesAisys CS2 Spec SheetCarlos IbaNo ratings yet
- CarescapeB650 Ver 1 Service Manual PDFDocument204 pagesCarescapeB650 Ver 1 Service Manual PDFcarolus2009No ratings yet
- GE Dash 3000,4000 V4 Monitor - User ManualDocument478 pagesGE Dash 3000,4000 V4 Monitor - User ManualLogicLife50% (2)
- Suction Pump FAZZINI F-30 - Service ManualDocument10 pagesSuction Pump FAZZINI F-30 - Service ManualAnonymous qmNwOUtUd100% (1)
- Wolf HD Endocam - User ManualDocument56 pagesWolf HD Endocam - User ManualAhmed 771000303No ratings yet
- Heinen & Löwenstein Leoni Baby Ventilator - Service ManualDocument16 pagesHeinen & Löwenstein Leoni Baby Ventilator - Service ManualAbraham Segovia MartinezNo ratings yet
- Intensive Care Ventilator MV200: Safety - Reliability - ComfortDocument7 pagesIntensive Care Ventilator MV200: Safety - Reliability - ComfortFathur ArRahmanNo ratings yet
- Alaris GP Service ManualDocument84 pagesAlaris GP Service ManualKittiwat Wongsuwan100% (1)
- NKV-330 enDocument12 pagesNKV-330 enmauricioNo ratings yet
- Beneheart R12 Operator's Manual V2.0 enDocument98 pagesBeneheart R12 Operator's Manual V2.0 enRahul Bag100% (4)
- Aitecs 2016 Syringe Pump - Service ManualDocument4 pagesAitecs 2016 Syringe Pump - Service ManualBruno Gonçalves Lima GomesNo ratings yet
- MRX Software Version 7 Instructions For UseDocument326 pagesMRX Software Version 7 Instructions For UseGavin TexeirraNo ratings yet
- Perfusor compact service manual overviewDocument39 pagesPerfusor compact service manual overviewDiep NguyentuanNo ratings yet
- SynoVent E3&E5 - Service Training-Medium - V1.0 - EN PDFDocument88 pagesSynoVent E3&E5 - Service Training-Medium - V1.0 - EN PDFJose Ivan Carvajal Cortizos0% (1)
- Service Manual Perfusor CompactDocument84 pagesService Manual Perfusor CompactDaniel Martinez CollazoNo ratings yet
- Evita 2 DuraDocument277 pagesEvita 2 DuraJorgeNo ratings yet
- BBraun Perfusor Compact SDocument16 pagesBBraun Perfusor Compact SsiromexNo ratings yet
- Manual Book Printer Warna Volution GE Sony UP 25MDDocument30 pagesManual Book Printer Warna Volution GE Sony UP 25MDmariscaNo ratings yet
- Acutronic Fabian Ventilator Service ManualDocument1 pageAcutronic Fabian Ventilator Service ManualIsmael Pérez Ruiz0% (1)
- DT 400S 300S DT 200S 150S CatalogueDocument4 pagesDT 400S 300S DT 200S 150S CatalogueOanh Xuxi0% (1)
- Manual (Eng) Monitor Mediana Ym1000Document103 pagesManual (Eng) Monitor Mediana Ym1000miguelNo ratings yet
- HAMILTON-G5 Ventilation Unit GuideDocument15 pagesHAMILTON-G5 Ventilation Unit GuideHeroki WidyaNo ratings yet
- Primedec Defibrillator Operating Manual PDFDocument56 pagesPrimedec Defibrillator Operating Manual PDFJuan Carlos GoyzuetaNo ratings yet
- Nova en Autoclave Tuttnauer PDFDocument12 pagesNova en Autoclave Tuttnauer PDFerikaNo ratings yet
- PM 9000 Express Service Manual 3 2 PDFDocument109 pagesPM 9000 Express Service Manual 3 2 PDFBetancur AlejandroNo ratings yet
- Draeger Infinity VistaDocument280 pagesDraeger Infinity VistaДмитрий ЧеNo ratings yet
- SERVO-s Ventilator System Service ManualDocument113 pagesSERVO-s Ventilator System Service ManualKaran JejurkarNo ratings yet
- Suction Unit Hospivac User ManualDocument10 pagesSuction Unit Hospivac User Manualcarlos tumimed casoNo ratings yet
- Drager Primus - InstructionsDocument282 pagesDrager Primus - InstructionsDiana InfanteNo ratings yet
- Newport Nmi E500Document3 pagesNewport Nmi E500Raj KumarNo ratings yet
- Aeon7200: Anesthesia MachineDocument2 pagesAeon7200: Anesthesia MachinePedro Nel Cifuentes RodriguezNo ratings yet
- CAREFUSION VENTILADOR Vela BrochureDocument5 pagesCAREFUSION VENTILADOR Vela BrochureArturo JuarezNo ratings yet
- Injectomat MC Agilia DataSheetDocument2 pagesInjectomat MC Agilia DataSheetanper81No ratings yet
- Drager Babytherm 8004 8010 Error ListDocument31 pagesDrager Babytherm 8004 8010 Error Listbioserviceltda2022100% (1)
- MIR Spirolab II - Service ManualDocument33 pagesMIR Spirolab II - Service ManualAugusto VieiraNo ratings yet
- Penlon Prima SP Anaesthesia Machine - User ManualDocument140 pagesPenlon Prima SP Anaesthesia Machine - User ManualKatyaNo ratings yet
- Service Manual Infusomat Space PDFDocument130 pagesService Manual Infusomat Space PDFpanxonegro100% (1)
- Brochure - Elisa 300 800-LM (2018) (E)Document32 pagesBrochure - Elisa 300 800-LM (2018) (E)Ngoc Nhanh HuynhNo ratings yet
- Elisa 300 - 800Document40 pagesElisa 300 - 800junaid ahmadNo ratings yet
- Elisa 300: Intensive Care VentilationDocument9 pagesElisa 300: Intensive Care VentilationReginaldo CaesarNo ratings yet
- CR Service Manual: Computed Radiography SystemDocument75 pagesCR Service Manual: Computed Radiography SystemMohsin LatifNo ratings yet
- Service Bulletin 30Document12 pagesService Bulletin 30ArielCristianUrquizoCallauNo ratings yet
- Kodak 101/102 Service ManualDocument20 pagesKodak 101/102 Service ManualAlfonso Niño100% (1)
- Multi VibratorDocument9 pagesMulti VibratormwaniaabediNo ratings yet
- PENTAX Ultrasound Endoscopes Reprocessing GuideDocument1 pagePENTAX Ultrasound Endoscopes Reprocessing GuideArielCristianUrquizoCallauNo ratings yet
- Novel TechniqueDocument7 pagesNovel TechniqueItaaAminotoNo ratings yet
- Drug Study (Pe)Document15 pagesDrug Study (Pe)Jobelle AcenaNo ratings yet
- GrammarDocument10 pagesGrammarRidhan RahmahNo ratings yet
- 206841Document1 page206841VinceOnikaa PerryGermanottaNo ratings yet
- MSI Privacy Policy - EnglishDocument11 pagesMSI Privacy Policy - Englishojik31No ratings yet
- Selina Concise Physics Class 8 ICSE SolutionsDocument37 pagesSelina Concise Physics Class 8 ICSE SolutionsAditya100% (1)
- Feasibility and CONOPSDocument64 pagesFeasibility and CONOPSGhaziAnwarNo ratings yet
- Ebook - Return-to-Gentleness by Anthony M McCrovitzDocument192 pagesEbook - Return-to-Gentleness by Anthony M McCrovitzSónia CarvalhoNo ratings yet
- Work Written: Student - I - Gabriela BocănețDocument14 pagesWork Written: Student - I - Gabriela BocănețEscu NykuNo ratings yet
- Conditionals MixedDocument2 pagesConditionals MixedAurelia Mihaela SoleaNo ratings yet
- D 5764 - 97a R02 RDU3NJQ - PDFDocument5 pagesD 5764 - 97a R02 RDU3NJQ - PDFRufo CascoNo ratings yet
- American Ceramic: SocietyDocument8 pagesAmerican Ceramic: SocietyPhi TiêuNo ratings yet
- Restrict Group Access in QV 9 Using ADDocument7 pagesRestrict Group Access in QV 9 Using ADBea BoocNo ratings yet
- Establishment of Measurement Objectives: PGT 202E Basic Educational Measurement and EvaluationDocument38 pagesEstablishment of Measurement Objectives: PGT 202E Basic Educational Measurement and EvaluationmaslianaNo ratings yet
- Part 5&6.cronbach Alpha and Sample Size ComputationDocument8 pagesPart 5&6.cronbach Alpha and Sample Size ComputationHazel AnnNo ratings yet
- Comparative ResearchDocument22 pagesComparative Researchtshiringtmg7No ratings yet
- Case Application (New Pay Plan) Alizay Waheed Kayani 24347Document2 pagesCase Application (New Pay Plan) Alizay Waheed Kayani 24347Alizay KayaniNo ratings yet
- Labor JurisdictionDocument37 pagesLabor JurisdictionChoystel Mae Artigas100% (1)
- UntitledDocument23 pagesUntitledjaanharafNo ratings yet
- English Proficiency TrainingDocument21 pagesEnglish Proficiency TrainingDayang GNo ratings yet
- Significant Figures and Unit Conversion Practice ProblemsDocument17 pagesSignificant Figures and Unit Conversion Practice ProblemsMichael Damian100% (3)
- Punjab govt grants EOL to doctors for postgraduate trainingDocument2 pagesPunjab govt grants EOL to doctors for postgraduate trainingMasroor HassanNo ratings yet
- Legal Counselling defined in broad and narrow sensesDocument5 pagesLegal Counselling defined in broad and narrow sensesRegie Rey AgustinNo ratings yet
- Paragraph WritingDocument22 pagesParagraph WritingarvindranganathanNo ratings yet
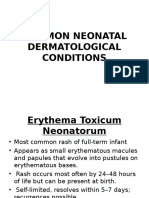
- Common Neonatal Dermatological ConditionsDocument27 pagesCommon Neonatal Dermatological ConditionsArslan SiddiquiNo ratings yet
- AFM Shark-EN 60 - 2017-05-21 - FinalDocument104 pagesAFM Shark-EN 60 - 2017-05-21 - FinalLance Montgomery BoyleNo ratings yet
- Syllabus - English (AU)Document5 pagesSyllabus - English (AU)Manasvi MehtaNo ratings yet
- Past-Simple-Regular-Verbs - WORD (Falta)Document21 pagesPast-Simple-Regular-Verbs - WORD (Falta)jeinNo ratings yet
- Spectral Correlation of OFDM SignalsDocument6 pagesSpectral Correlation of OFDM Signalsazebshaikh3927No ratings yet
- Lol Wellness Principles For Dynamic LivingDocument171 pagesLol Wellness Principles For Dynamic LivingTumwine Kahweza ProsperNo ratings yet
- DNV-OSS-305 Rules For Certification and Verification of Diving Systems October2011Document85 pagesDNV-OSS-305 Rules For Certification and Verification of Diving Systems October2011Rumi Kai RekaNo ratings yet