You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- SX3000 Manual de Servicio PDFDocument198 pagesSX3000 Manual de Servicio PDFJorge Bellido100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
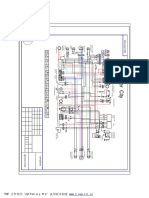
- Cpi Oliver City EldiagramDocument1 pageCpi Oliver City EldiagramHenry BraunNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- New Microsoft Office Word DocumentDocument9 pagesNew Microsoft Office Word DocumentGaurav JaiswalNo ratings yet
- Energy Audits in Thermal Power StationDocument62 pagesEnergy Audits in Thermal Power Stationfiroj_khan995% (22)
- Near Field Communication Based College CanteenDocument5 pagesNear Field Communication Based College CanteenJunaid M FaisalNo ratings yet
- A 20 Year Old Man Suffered From A Spinal Cord Injury at The C2 To C3 Level As The Result of A Motorcycle AccidentDocument4 pagesA 20 Year Old Man Suffered From A Spinal Cord Injury at The C2 To C3 Level As The Result of A Motorcycle AccidentqingwenNo ratings yet
- Octavius Tea OfflineDocument7 pagesOctavius Tea Offlineapi-323468541No ratings yet
- Guico - Shrimp Dissection (Exp 4)Document8 pagesGuico - Shrimp Dissection (Exp 4)aeprintsNo ratings yet
- Unit 4 Notes GDJPDocument2 pagesUnit 4 Notes GDJPAnanth VelNo ratings yet
- Nasib Ahmad Faqirzada Resume CVDocument4 pagesNasib Ahmad Faqirzada Resume CVNasib Ahmad FaqirzadaNo ratings yet
- Use of Nonaqueous Solvents in Parenteral ProductsDocument11 pagesUse of Nonaqueous Solvents in Parenteral ProductsMustafa ShahinNo ratings yet
- Jurnal EntropionDocument7 pagesJurnal EntropionOgiesilaenNo ratings yet
- A Control System of DC Motor Speed - Systematic ReviewDocument19 pagesA Control System of DC Motor Speed - Systematic ReviewCanizares1000No ratings yet
- PMLS 2 Midterm 1Document14 pagesPMLS 2 Midterm 1ematias230000001830No ratings yet
- Concrete Construction Article PDF - Quality Control in Concrete ConstructionDocument3 pagesConcrete Construction Article PDF - Quality Control in Concrete ConstructionJeremiah ObiacoroNo ratings yet
- Sto. Niño Academy of Bamban, Inc.: The Roar Learning Guide SeriesDocument3 pagesSto. Niño Academy of Bamban, Inc.: The Roar Learning Guide SeriesJerome Neil DayritNo ratings yet
- Being and Nothingness The Look SartreDocument3 pagesBeing and Nothingness The Look Sartremaximomore50% (4)
- PTV810 Service ManualDocument567 pagesPTV810 Service Manualbr41nNo ratings yet
- Internal Combustion Engine Layout and ConfigurationDocument11 pagesInternal Combustion Engine Layout and ConfigurationKathija SumanNo ratings yet
- CVDocument1 pageCVSiddharth ChauhanNo ratings yet
- Evap-Lt 60 KV CG ShimaDocument439 pagesEvap-Lt 60 KV CG ShimaDax CasraNo ratings yet
- FNN111 Nutrition Chapter 1 NOTES The Role of Nutrition in Our HealthDocument5 pagesFNN111 Nutrition Chapter 1 NOTES The Role of Nutrition in Our HealthRina JungNo ratings yet
- The Phantom of The OperaDocument272 pagesThe Phantom of The OperaJames Andrew CurtisNo ratings yet
- Triveni Kala Sangam India International Center Case StudyDocument1 pageTriveni Kala Sangam India International Center Case StudyHamzah AbdullahNo ratings yet
- GearsDocument246 pagesGearsVinayak AryanNo ratings yet
- Electrix TweakerDocument1 pageElectrix TweakerUSER58679No ratings yet
- E. Common MineralsDocument19 pagesE. Common MineralsWilma Marquez HabocNo ratings yet
- Carbon CycleDocument12 pagesCarbon CyclePorco dioNo ratings yet
- Grade 6 - Worksheet - Mid Term ExamDocument3 pagesGrade 6 - Worksheet - Mid Term ExamSharmila Kumari RNo ratings yet
- PR Sava Intensa Uhp 26102009 English F Upd Tcm2382-72613Document3 pagesPR Sava Intensa Uhp 26102009 English F Upd Tcm2382-72613mac1677No ratings yet