You might also like
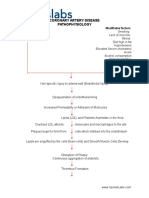
- Coronary Artery Disease PathophysiologyDocument3 pagesCoronary Artery Disease Pathophysiologynursing concept maps50% (4)
- Iron Deficiency Anemia Schematic DiagramDocument2 pagesIron Deficiency Anemia Schematic DiagramCyrus De Asis83% (12)
- NCP GunshotDocument13 pagesNCP GunshotMichael John F. Natividad0% (1)
- Nursing Care Plan-EpilepsyDocument24 pagesNursing Care Plan-Epilepsyamit80% (10)
- CASE PRESENTATION ON DEPRESSIONDocument15 pagesCASE PRESENTATION ON DEPRESSIONManisha SamsonNo ratings yet
- CASE Study ENCEPHALITISDocument29 pagesCASE Study ENCEPHALITISMeena Koushal67% (3)
- Case Presentation HIVDocument28 pagesCase Presentation HIVAnonymous 0C4OZmR100% (4)
- Typhoid Fever Case StudyDocument10 pagesTyphoid Fever Case StudyArchana Sahu100% (3)
- Nursing Care Planpulmonary TuberculosisDocument20 pagesNursing Care Planpulmonary Tuberculosisgandhialpit100% (5)
- CASE STUDY MeningitisDocument19 pagesCASE STUDY Meningitissonal aranha100% (3)
- Case Presentation Pleural EffusionDocument30 pagesCase Presentation Pleural EffusionSarita100% (2)
- Manibabhula Nursing College, Bardoli: Subject: Medical Surgical Nursing Topic: Case Study OnDocument18 pagesManibabhula Nursing College, Bardoli: Subject: Medical Surgical Nursing Topic: Case Study Onmeghana100% (4)
- History Collection and Physical Examination Kardex Nurses NotesDocument41 pagesHistory Collection and Physical Examination Kardex Nurses Notessubi86% (7)
- Case Study Nephrotic SyndromeDocument26 pagesCase Study Nephrotic SyndromeDimpal Choudhary0% (2)
- Procedure On Chest PhysiotherapyDocument13 pagesProcedure On Chest PhysiotherapyDimpal ChoudharyNo ratings yet
- Fluid & Electrolytes and Acid Base BalanceDocument108 pagesFluid & Electrolytes and Acid Base Balanceapi-3701489100% (12)
- Identification DataDocument22 pagesIdentification DataDimpal Choudhary100% (1)
- History Collection and Physical Examination Kardex Nurses Notes PDFDocument53 pagesHistory Collection and Physical Examination Kardex Nurses Notes PDFSalma SultanaNo ratings yet
- Dhanwantari College of Nursing: Care Plan On: Nephrotic SyndromeDocument19 pagesDhanwantari College of Nursing: Care Plan On: Nephrotic SyndromeGayatri MudliyarNo ratings yet
- Appendicitis Nursing Care GuideDocument32 pagesAppendicitis Nursing Care GuideUday Kumar100% (1)
- Otitis Media - CSDocument14 pagesOtitis Media - CSMASII100% (3)
- Case Presentation TofDocument33 pagesCase Presentation TofISLAMIC KNOWLEDGE BASED ON TRULY HADIS100% (1)
- Nursing Care PlanDocument14 pagesNursing Care Plananimesh panda100% (3)
- Failure To Thrive.Document14 pagesFailure To Thrive.Gayatri MudliyarNo ratings yet
- 1.case Presentation CHDDocument23 pages1.case Presentation CHDDHARM MEENA0% (1)
- A Case Presentation On PneumoniaDocument74 pagesA Case Presentation On PneumoniaYengkhom YoshiNo ratings yet
- Pneumonia Careplan MedDocument17 pagesPneumonia Careplan MedGayatri MudliyarNo ratings yet
- Nursing Care Plan for ELBW Baby with RDSDocument21 pagesNursing Care Plan for ELBW Baby with RDSMeena KoushalNo ratings yet
- Identification Data of PatientDocument8 pagesIdentification Data of Patientanimesh panda50% (2)
- A Case Presentation On MeningitisDocument29 pagesA Case Presentation On MeningitisNeeta0% (1)
- CARE PLAN On HyponatremiaDocument35 pagesCARE PLAN On Hyponatremia2020 MSc bhuvaneswari 05No ratings yet
- Child with Nephritic Syndrome Care PlanDocument22 pagesChild with Nephritic Syndrome Care Planamit50% (2)
- Case Study On AppendicitisDocument21 pagesCase Study On Appendicitisshweta singh100% (1)
- Care Plan On Nephrotic SyndromeDocument31 pagesCare Plan On Nephrotic Syndromepriyanka bhavsar100% (1)
- Case Study PneumoniaDocument12 pagesCase Study PneumoniaFretzie Mae RamasNo ratings yet
- Case Presentation On Wilms TumorDocument25 pagesCase Presentation On Wilms TumorDeepika100% (1)
- Case Study On Cerebral PalsyDocument37 pagesCase Study On Cerebral PalsyISLAMIC KNOWLEDGE BASED ON TRULY HADIS60% (5)
- Case Study - OTITIS MEDIADocument9 pagesCase Study - OTITIS MEDIAHasing Amado100% (1)
- 03 NCP 5 Pulmonary Tuberculosis LalitDocument17 pages03 NCP 5 Pulmonary Tuberculosis Lalitamit100% (2)
- Typhoid Case PresentationDocument17 pagesTyphoid Case PresentationAbdulMazidZabir0% (1)
- 2.A Ndera CaseDocument14 pages2.A Ndera CaseNsengimana Eric MaxigyNo ratings yet
- Patient Identification and Care PlanDocument8 pagesPatient Identification and Care Plananimesh panda100% (3)
- Understanding Intestinal Obstruction in ChildrenDocument36 pagesUnderstanding Intestinal Obstruction in ChildrenMamta Parmar100% (1)
- Nursing Care Plan for Obsessive Compulsive DisorderDocument26 pagesNursing Care Plan for Obsessive Compulsive Disorderkiran mahal100% (7)
- Care Plan On Pneumonia: Submitted ToDocument18 pagesCare Plan On Pneumonia: Submitted ToSarEdu Inst100% (3)
- Jaundice Case Study Nursing ManagementDocument30 pagesJaundice Case Study Nursing Managementkamini ChoudharyNo ratings yet
- Case Study On Jaundice-1Document30 pagesCase Study On Jaundice-1kamini Choudhary100% (5)
- Health Assessment Peptic UlcerDocument13 pagesHealth Assessment Peptic UlcerHimani PatelNo ratings yet
- Case Presentation TofDocument32 pagesCase Presentation TofISLAMIC KNOWLEDGE BASED ON TRULY HADIS100% (2)
- Case Presentation On GbsDocument23 pagesCase Presentation On GbsRucHi ShArmaNo ratings yet
- 03 NCP 1 Viral HepatitisDocument17 pages03 NCP 1 Viral Hepatitisamit100% (2)
- Diarrhea Case PresentationDocument20 pagesDiarrhea Case Presentationriya singh100% (8)
- Case Presentation Acute Abdomen PediatricDocument17 pagesCase Presentation Acute Abdomen PediatricDevina TandiasNo ratings yet
- Bronchopneumonia Case PresentationDocument17 pagesBronchopneumonia Case Presentationgandhialpit100% (1)
- Case Report MeningitisDocument69 pagesCase Report MeningitisBelinda Orline100% (1)
- 2.e.case Ctudy On BPADDocument9 pages2.e.case Ctudy On BPADManisa Parida100% (1)
- NURSING Care Plan On MiDocument20 pagesNURSING Care Plan On MiSanvar Mal Soni100% (1)
- Case Presentation 3 DR Oscar Laryngitis TBDocument33 pagesCase Presentation 3 DR Oscar Laryngitis TBmarajuu50% (2)
- Case Presentatio Insomnia 1Document49 pagesCase Presentatio Insomnia 1kiran mahal100% (1)
- Epilepsy Care PlanDocument57 pagesEpilepsy Care PlanNilesh Jain83% (6)
- Case Presentation On Coronary Artery Disease - 090908Document54 pagesCase Presentation On Coronary Artery Disease - 090908Parth Vasave100% (3)
- Case Study BronchiolitisDocument15 pagesCase Study Bronchiolitisanimesh panda0% (1)
- Patient Medical ReportDocument20 pagesPatient Medical ReportDimpal ChoudharyNo ratings yet
- PSS3: Malnutrition - Protein Energy Malnutrition (Kwashiorkor and Marasmus)Document26 pagesPSS3: Malnutrition - Protein Energy Malnutrition (Kwashiorkor and Marasmus)anon_67984147No ratings yet
- Wilsons Case StudyDocument35 pagesWilsons Case StudyNoor HashmeeNo ratings yet
- Pathophysiology of COPDDocument1 pagePathophysiology of COPDDimpal ChoudharyNo ratings yet
- Blood PressureDocument1 pageBlood PressureDimpal ChoudharyNo ratings yet
- Pulmonary FibrosisDocument4 pagesPulmonary FibrosisDimpal Choudhary100% (2)
- Pathophysiology of Pleural EffusionDocument1 pagePathophysiology of Pleural EffusionDimpal ChoudharyNo ratings yet
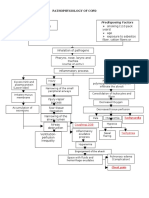
- Pathophysiology of PneumoniaDocument4 pagesPathophysiology of PneumoniaDimpal ChoudharyNo ratings yet
- Cystic FibrosisDocument23 pagesCystic Fibrosisclarytah0% (1)
- Peripheral Artery Disease: Nikhil Vaishnav M.Sc. (Nursing)Document70 pagesPeripheral Artery Disease: Nikhil Vaishnav M.Sc. (Nursing)Dimpal ChoudharyNo ratings yet
- Von Willebrand DiseaseDocument4 pagesVon Willebrand DiseaseDimpal ChoudharyNo ratings yet
- Nursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDocument5 pagesNursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDimpal Choudhary100% (1)
- Procedure On Lumber PunctureDocument8 pagesProcedure On Lumber PunctureDimpal ChoudharyNo ratings yet
- Understanding disastersDocument4 pagesUnderstanding disastersDimpal ChoudharyNo ratings yet
- Nursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDocument4 pagesNursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDimpal ChoudharyNo ratings yet
- Lumber Puncture ProcedureDocument8 pagesLumber Puncture ProcedureDimpal ChoudharyNo ratings yet
- Nursing History, Education and OrganizationDocument59 pagesNursing History, Education and OrganizationHamza Yazid50% (2)
- Acute and Repeated Exposure To Chemotherapeutic Agents Is Especially DangerousDocument1 pageAcute and Repeated Exposure To Chemotherapeutic Agents Is Especially DangerousDimpal ChoudharyNo ratings yet
- Abdominal PainDocument5 pagesAbdominal PainDimpal ChoudharyNo ratings yet
- Von Willebrand DiseaseDocument4 pagesVon Willebrand DiseaseDimpal ChoudharyNo ratings yet
- Congenital Heart DiseaseDocument82 pagesCongenital Heart DiseaseDimpal ChoudharyNo ratings yet
- NeurotransmiterDocument5 pagesNeurotransmiterDimpal ChoudharyNo ratings yet
- Uninodular Goitre: One Thyroid Nodule Can Be Either Inactive, or Active (Toxic)Document6 pagesUninodular Goitre: One Thyroid Nodule Can Be Either Inactive, or Active (Toxic)Dimpal ChoudharyNo ratings yet
- Atrial Septal DefectDocument4 pagesAtrial Septal DefectDimpal ChoudharyNo ratings yet
- ABSTRACTDocument1 pageABSTRACTDimpal ChoudharyNo ratings yet
- Hemophilia Type ADocument4 pagesHemophilia Type ADimpal ChoudharyNo ratings yet
- Procedure On ThoracentesisDocument11 pagesProcedure On ThoracentesisDimpal ChoudharyNo ratings yet
- Exploring the Procedure of Panel DiscussionDocument19 pagesExploring the Procedure of Panel DiscussionDimpal ChoudharyNo ratings yet
- FutureisticDocument48 pagesFutureisticDimpal ChoudharyNo ratings yet
- Bladder IrrigationDocument5 pagesBladder IrrigationDimpal ChoudharyNo ratings yet
- Continue: Sharma Mohan Textbook of Tuberculosis PDFDocument2 pagesContinue: Sharma Mohan Textbook of Tuberculosis PDFAbdul JalilNo ratings yet
- Ecmocard StudiesDocument34 pagesEcmocard StudiesMonica KuhonNo ratings yet
- Annex 1 Part 8Document4 pagesAnnex 1 Part 8Melinda Anggita SetiyadiNo ratings yet
- HysterectomyDocument9 pagesHysterectomyEva Yunita IINo ratings yet
- Final ReseachDocument67 pagesFinal ReseachKetheesaran LingamNo ratings yet
- Path Anat Part 1Document184 pagesPath Anat Part 1Javier Saad100% (1)
- Antibiotc Made Easy PDFDocument12 pagesAntibiotc Made Easy PDFAmjad_2020100% (1)
- Zoology AscriseDocument12 pagesZoology AscrisepappunaagraajNo ratings yet
- Ucu Iii Post Test July 4 2023 RatioDocument74 pagesUcu Iii Post Test July 4 2023 RatioVince C. MatamisNo ratings yet
- Ri Juli 2019Document29 pagesRi Juli 2019WahyuNo ratings yet
- Cardiac Catheterization: Why It's DoneDocument3 pagesCardiac Catheterization: Why It's DoneRania S. HamdanNo ratings yet
- Typhoid FeverDocument4 pagesTyphoid FeverBernice GyapongNo ratings yet
- Contact Tracing Form San LuisDocument3 pagesContact Tracing Form San LuisPoblacion 04 San LuisNo ratings yet
- For All (Uhs, Ke, Nums, Etc) : Chapter 1: Anatomy of EarDocument17 pagesFor All (Uhs, Ke, Nums, Etc) : Chapter 1: Anatomy of EarSohail Abbas KhanNo ratings yet
- Arya Vaidya Sala KottakkaDocument2 pagesArya Vaidya Sala KottakkaL RNo ratings yet
- Smovement Disorder After StrokeDocument39 pagesSmovement Disorder After StrokeDaniel SetiawanNo ratings yet
- DR Mercola - FDA Says Misinformation Is A Top KillerDocument7 pagesDR Mercola - FDA Says Misinformation Is A Top Killerguy777No ratings yet
- Food and Safety TrainingDocument3 pagesFood and Safety TrainingkenzieNo ratings yet
- Articulo Manejo Paciente IrcDocument8 pagesArticulo Manejo Paciente IrcJUAN FONSECANo ratings yet
- Limfoma Maligna FinalDocument50 pagesLimfoma Maligna FinalAulia Ayu PuspitaNo ratings yet
- Breast Cancer Screening and Early Diagnosis Action Plan 2021 2025Document64 pagesBreast Cancer Screening and Early Diagnosis Action Plan 2021 2025Universal FamilyNo ratings yet
- Guidelines for competency-based paediatric trainingDocument18 pagesGuidelines for competency-based paediatric trainingMohammed ameen mohammed AljabriNo ratings yet
- CSFDocument5 pagesCSFjalan_zNo ratings yet
- Human Karyotyping Lab Identifies Genetic DisordersDocument7 pagesHuman Karyotyping Lab Identifies Genetic DisordersEditorialranged CartoonistoplaneNo ratings yet
- Module 3 ReviDocument35 pagesModule 3 ReviJohn Van Dave TaturoNo ratings yet
- Management of Globus Hystericusand Role of AntidepressantsDocument5 pagesManagement of Globus Hystericusand Role of AntidepressantsIJAR JOURNALNo ratings yet
- Vethathiriyam - Wellness & LongevityDocument2 pagesVethathiriyam - Wellness & LongevityaleppyNo ratings yet