You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Care Plan On PneumoniaDocument22 pagesCare Plan On PneumoniaDimpal Choudhary100% (5)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Procedure On Chest PhysiotherapyDocument13 pagesProcedure On Chest PhysiotherapyDimpal ChoudharyNo ratings yet
- Bladder IrrigationDocument5 pagesBladder IrrigationDimpal ChoudharyNo ratings yet
- Pathophysiology of PneumoniaDocument4 pagesPathophysiology of PneumoniaDimpal ChoudharyNo ratings yet
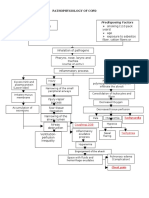
- Streptococcus Pneumonae: Pathophysiology of CopdDocument1 pageStreptococcus Pneumonae: Pathophysiology of CopdDimpal ChoudharyNo ratings yet
- Pathophysiology of Pleural EffusionDocument1 pagePathophysiology of Pleural EffusionDimpal ChoudharyNo ratings yet
- Peripheral Artery Disease: Nikhil Vaishnav M.Sc. (Nursing)Document70 pagesPeripheral Artery Disease: Nikhil Vaishnav M.Sc. (Nursing)Dimpal ChoudharyNo ratings yet
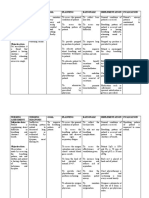
- Nursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDocument5 pagesNursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDimpal Choudhary100% (1)
- Nursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDocument4 pagesNursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDimpal ChoudharyNo ratings yet
- Lumber Puncture ProcedureDocument8 pagesLumber Puncture ProcedureDimpal ChoudharyNo ratings yet
- Pulmonary FibrosisDocument4 pagesPulmonary FibrosisDimpal Choudhary100% (2)
- Procedure On Lumber PunctureDocument8 pagesProcedure On Lumber PunctureDimpal ChoudharyNo ratings yet
- Nursing EducationDocument19 pagesNursing EducationDimpal ChoudharyNo ratings yet
- Congenital Heart DiseaseDocument82 pagesCongenital Heart DiseaseDimpal ChoudharyNo ratings yet
- Uninodular Goitre: One Thyroid Nodule Can Be Either Inactive, or Active (Toxic)Document6 pagesUninodular Goitre: One Thyroid Nodule Can Be Either Inactive, or Active (Toxic)Dimpal ChoudharyNo ratings yet
- Polycythemia Vera: What Are The Symptoms of Polycythemia?Document10 pagesPolycythemia Vera: What Are The Symptoms of Polycythemia?Dimpal ChoudharyNo ratings yet
- Preparation OF Group Work: Netaji Subhash College of NursingDocument7 pagesPreparation OF Group Work: Netaji Subhash College of NursingDimpal ChoudharyNo ratings yet
- Self-Directed LearningDocument18 pagesSelf-Directed LearningDimpal ChoudharyNo ratings yet
- Introduction-:: Time Specific Objective Content Av AidsDocument7 pagesIntroduction-:: Time Specific Objective Content Av AidsDimpal ChoudharyNo ratings yet
- It Is of Two Types Natural Disaster Man - Made DisasterDocument4 pagesIt Is of Two Types Natural Disaster Man - Made DisasterDimpal ChoudharyNo ratings yet
- Capillaria PhilippinensisDocument16 pagesCapillaria PhilippinensisMichelle San Miguel FeguroNo ratings yet
- DOH Administrative Order No. 2021-0005Document25 pagesDOH Administrative Order No. 2021-0005Legal Office Antipolo CityNo ratings yet
- Mental Health - Quiz #1Document5 pagesMental Health - Quiz #1SabrinaNicole100% (1)
- Case StudyDocument5 pagesCase StudyHomework PingNo ratings yet
- Administration of O2 TherapyDocument36 pagesAdministration of O2 TherapyFatima Ysabelle Marie RuizNo ratings yet
- ReferensiDocument8 pagesReferensiRabiatul AdawiyahNo ratings yet
- Hand InjuriesDocument13 pagesHand InjuriesRifQi KurniawanNo ratings yet
- Laporan-Laporan ObatDocument83 pagesLaporan-Laporan Obatsofyan hadyNo ratings yet
- Buy Zopiclone Online - PDF 2Document14 pagesBuy Zopiclone Online - PDF 2rxmed usaNo ratings yet
- CP PPT 10-11-11Document49 pagesCP PPT 10-11-11Eaht QuirongNo ratings yet
- Lec4Morbidity (Revised07)Document29 pagesLec4Morbidity (Revised07)Zahra MotorwalaNo ratings yet
- Delivery of Health Care Services in RuralDocument29 pagesDelivery of Health Care Services in RuralMahenurNo ratings yet
- 1035 Pathway CKDDocument1 page1035 Pathway CKDeka pandeNo ratings yet
- Bye-Bye Back Pain - 9 Holistic Solutions For Relief From Sciatica, Lumbago, Slipped Disc, and Backache PDFDocument150 pagesBye-Bye Back Pain - 9 Holistic Solutions For Relief From Sciatica, Lumbago, Slipped Disc, and Backache PDFMurali R100% (1)
- Preventive PanchakarmaDocument6 pagesPreventive PanchakarmaanuNo ratings yet
- Suicidal Ideation, Suicide Attempt and Completed SuicideDocument3 pagesSuicidal Ideation, Suicide Attempt and Completed SuicideHannah BenitezNo ratings yet
- Pilot Testing of Triage Coding System in Home-Based Palliative Care Using Edmonton Symptom Assessment ScaleDocument6 pagesPilot Testing of Triage Coding System in Home-Based Palliative Care Using Edmonton Symptom Assessment ScaleMehak KhannaNo ratings yet
- Depresion PostpartoDocument6 pagesDepresion PostpartoOscar Alejandro Cardenas QuinteroNo ratings yet
- CardioDocument10 pagesCardioMar OrdanzaNo ratings yet
- Hulskamp, M.A.A. 08Document297 pagesHulskamp, M.A.A. 08Henry LopesNo ratings yet
- Classification of StrokeDocument3 pagesClassification of StrokeafhamazmanNo ratings yet
- Test QuestionsDocument28 pagesTest QuestionsJerson CastroNo ratings yet
- Professional Meeting Reflective Journal 1Document3 pagesProfessional Meeting Reflective Journal 1api-402479662No ratings yet
- List of Accredited DTLS: Republic of The Philippines Department of Health Bureau of Health Facilities and ServicesDocument63 pagesList of Accredited DTLS: Republic of The Philippines Department of Health Bureau of Health Facilities and ServicesNomar Casiven NonatoNo ratings yet
- Literature Review On Otc DrugsDocument6 pagesLiterature Review On Otc Drugsafmzsawcpkjfzj100% (1)
- Skill 23 Perform and Repair An EpisiotomyDocument2 pagesSkill 23 Perform and Repair An EpisiotomyThulasi tootsieNo ratings yet
- Lecture Diarrhea and ConstipationDocument63 pagesLecture Diarrhea and ConstipationKrittin NaravejsakulNo ratings yet
- Mksap PDFDocument2 pagesMksap PDFb16No ratings yet
- Application of Heat and ColdDocument63 pagesApplication of Heat and ColdNivek Adej Zuproc RotiduaNo ratings yet
- 6 - SINGKATAN Make A Past and Perfect TenseDocument3 pages6 - SINGKATAN Make A Past and Perfect TenseKarina Izafira NibrasNo ratings yet