You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- DR Sebi - Electric Foods ListDocument3 pagesDR Sebi - Electric Foods ListTehuti byNature90% (58)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Chrononutrition by Alain Delabos (English)Document14 pagesChrononutrition by Alain Delabos (English)JasminaIlincic100% (2)
- Care Plan On PneumoniaDocument22 pagesCare Plan On PneumoniaDimpal Choudhary100% (5)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Dropping Acid The Reflux Diet Cookbook & Cure Foods To Eat & AvoidDocument8 pagesDropping Acid The Reflux Diet Cookbook & Cure Foods To Eat & AvoidBig Krab33% (3)
- Procedure On Chest PhysiotherapyDocument13 pagesProcedure On Chest PhysiotherapyDimpal ChoudharyNo ratings yet
- Bladder IrrigationDocument5 pagesBladder IrrigationDimpal ChoudharyNo ratings yet
- Wild Fermentation, 2nd Edition - ForewordDocument2 pagesWild Fermentation, 2nd Edition - ForewordChelsea Green PublishingNo ratings yet
- Lunch Menu North Peak Brewing CompanyDocument6 pagesLunch Menu North Peak Brewing CompanyMatt SnyderNo ratings yet
- Pathophysiology of PneumoniaDocument4 pagesPathophysiology of PneumoniaDimpal ChoudharyNo ratings yet
- Streptococcus Pneumonae: Pathophysiology of CopdDocument1 pageStreptococcus Pneumonae: Pathophysiology of CopdDimpal ChoudharyNo ratings yet
- Pathophysiology of Pleural EffusionDocument1 pagePathophysiology of Pleural EffusionDimpal ChoudharyNo ratings yet
- Peripheral Artery Disease: Nikhil Vaishnav M.Sc. (Nursing)Document70 pagesPeripheral Artery Disease: Nikhil Vaishnav M.Sc. (Nursing)Dimpal ChoudharyNo ratings yet
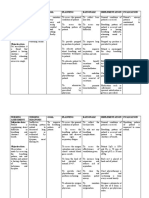
- Nursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDocument5 pagesNursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDimpal Choudhary100% (1)
- Nursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDocument4 pagesNursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDimpal ChoudharyNo ratings yet
- Lumber Puncture ProcedureDocument8 pagesLumber Puncture ProcedureDimpal ChoudharyNo ratings yet
- Pulmonary FibrosisDocument4 pagesPulmonary FibrosisDimpal Choudhary100% (2)
- Procedure On Lumber PunctureDocument8 pagesProcedure On Lumber PunctureDimpal ChoudharyNo ratings yet
- Nursing EducationDocument19 pagesNursing EducationDimpal ChoudharyNo ratings yet
- Congenital Heart DiseaseDocument82 pagesCongenital Heart DiseaseDimpal ChoudharyNo ratings yet
- Uninodular Goitre: One Thyroid Nodule Can Be Either Inactive, or Active (Toxic)Document6 pagesUninodular Goitre: One Thyroid Nodule Can Be Either Inactive, or Active (Toxic)Dimpal ChoudharyNo ratings yet
- Polycythemia Vera: What Are The Symptoms of Polycythemia?Document10 pagesPolycythemia Vera: What Are The Symptoms of Polycythemia?Dimpal ChoudharyNo ratings yet
- Preparation OF Group Work: Netaji Subhash College of NursingDocument7 pagesPreparation OF Group Work: Netaji Subhash College of NursingDimpal ChoudharyNo ratings yet
- Self-Directed LearningDocument18 pagesSelf-Directed LearningDimpal ChoudharyNo ratings yet
- Introduction-:: Time Specific Objective Content Av AidsDocument7 pagesIntroduction-:: Time Specific Objective Content Av AidsDimpal ChoudharyNo ratings yet
- It Is of Two Types Natural Disaster Man - Made DisasterDocument4 pagesIt Is of Two Types Natural Disaster Man - Made DisasterDimpal ChoudharyNo ratings yet
- When I'm Bored I Make Soup - The BookDocument77 pagesWhen I'm Bored I Make Soup - The BookPeter100% (50)
- Language Focus: Unit 4 Test: Extra - Answer KeyDocument2 pagesLanguage Focus: Unit 4 Test: Extra - Answer KeyGorgi TodorovNo ratings yet
- Enzymes in HoneyDocument4 pagesEnzymes in HoneyWJ NgNo ratings yet
- Aahar-Fusion Product CatalogDocument16 pagesAahar-Fusion Product CatalogAditi ChandrasekarNo ratings yet
- Buena Therese MonillasDocument3 pagesBuena Therese MonillasBuena Therese MonillasNo ratings yet
- F B Service TestDocument5 pagesF B Service TestWinkle Love Cefre OlivoNo ratings yet
- Student's Name: Fredy Andrés Chirivi Tellez: A Lot ofDocument3 pagesStudent's Name: Fredy Andrés Chirivi Tellez: A Lot ofyenifer guzmanNo ratings yet
- HE - Food and Beverage Services CG PDFDocument15 pagesHE - Food and Beverage Services CG PDFChona Maata-ColoniaNo ratings yet
- Cur Met GuavaDocument12 pagesCur Met Guavapalak mograNo ratings yet
- PKC ContentsDocument3 pagesPKC ContentsCt HajarNo ratings yet
- Case Study 2 Meal Time With A ToddlerDocument2 pagesCase Study 2 Meal Time With A ToddlerHEIDE FULLEROSNo ratings yet
- Organic Bengal Gram Split Rev 01Document1 pageOrganic Bengal Gram Split Rev 01Jerome InfantNo ratings yet
- Prova de Inglês 7º Ano Av1 4° B HectorDocument2 pagesProva de Inglês 7º Ano Av1 4° B HectorHector GuilhermeNo ratings yet
- Packaged Foods & Meats in India: Industry ProfileDocument21 pagesPackaged Foods & Meats in India: Industry ProfileAbhishek SinghNo ratings yet
- Vanilla Rum Panna Cotta With Salted Caramel Recipe - Ina Garten - Food NetworkDocument1 pageVanilla Rum Panna Cotta With Salted Caramel Recipe - Ina Garten - Food NetworkMaria Goreti RodriguesNo ratings yet
- Filipino RecipesDocument7 pagesFilipino RecipesJerlyn OberioNo ratings yet
- 002-Alimon Ketik SettingDocument8 pages002-Alimon Ketik Settingambo wellangNo ratings yet
- NVSU-FR-ICD-05-00 (081220) : Purposes Only and Not For Commercial Distribution,"Document21 pagesNVSU-FR-ICD-05-00 (081220) : Purposes Only and Not For Commercial Distribution,"Andrei Lorraine Keith MacasuNo ratings yet
- SOP Allergen ControlDocument3 pagesSOP Allergen Controlyolasusanto100% (1)
- (Bam) (Bam) (Bam) (Bam) (Bam) (Bam) (Bam)Document3 pages(Bam) (Bam) (Bam) (Bam) (Bam) (Bam) (Bam)Nhan Trinh NgocNo ratings yet
- Region: RNL Food Concepts. Inc Company Profile 2018Document12 pagesRegion: RNL Food Concepts. Inc Company Profile 2018Steve MaiwatNo ratings yet
- 1191 & 1153Document7 pages1191 & 1153Amruta JadhavNo ratings yet
- Nuts, Oilseeds, Dried LegumesDocument8 pagesNuts, Oilseeds, Dried LegumesAhmad Nur AyanlehNo ratings yet
- Role of Monsoon in Indian AgricultureDocument4 pagesRole of Monsoon in Indian AgricultureRoshan GiriNo ratings yet
- Research-1 On BarleyDocument35 pagesResearch-1 On Barleyharmeetsingh7739No ratings yet