You might also like
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- 134 - Neurology Pathology) Pons LesionsDocument5 pages134 - Neurology Pathology) Pons LesionsTamaraNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Antifungal Drugs: Side Effects and Adverse Reactions of Amphotericin BDocument23 pagesAntifungal Drugs: Side Effects and Adverse Reactions of Amphotericin BElizabeth IdananNo ratings yet
- The Neuropsychiatry of EpilepsyDocument361 pagesThe Neuropsychiatry of Epilepsypablo_zabala100% (3)
- Chest ExaminationDocument14 pagesChest Examinationsajad abasewNo ratings yet
- Pediatric Drug DosesDocument27 pagesPediatric Drug DosesAlisha AhmadNo ratings yet
- Drug Study (Seretide)Document1 pageDrug Study (Seretide)Rene John Francisco100% (1)
- 21.neural Control and CoordinationDocument44 pages21.neural Control and Coordinationg1307No ratings yet
- Mental Health and Suicide Prevention During Covid-19 PandemicDocument30 pagesMental Health and Suicide Prevention During Covid-19 PandemicAkanksha DubeyNo ratings yet
- Physical Assesment Assignment 1Document25 pagesPhysical Assesment Assignment 1inoka sandamali AriyarathneNo ratings yet
- Sleep Calculator: How Much Sleep Do You NeedDocument12 pagesSleep Calculator: How Much Sleep Do You NeedNyarickInsomNisaNo ratings yet
- Short Case and Long Case by Dr. MurtozaDocument79 pagesShort Case and Long Case by Dr. Murtoza202Manjida Rahman OniNo ratings yet
- Preeclampsia and EclampsiaDocument24 pagesPreeclampsia and EclampsiaLuisa SarangayNo ratings yet
- Headnursing Final OutputDocument30 pagesHeadnursing Final OutputCharissa Magistrado De LeonNo ratings yet
- Asf PR1Document10 pagesAsf PR1Norryne Myla N. NovidaNo ratings yet
- Sore ThroatDocument10 pagesSore Throatapi-551073862No ratings yet
- Peringkasan Noun ClauseDocument4 pagesPeringkasan Noun Clauseria.janitaNo ratings yet
- Morrison, 2010Document11 pagesMorrison, 2010Jbl2328No ratings yet
- NCP ThoracostomyDocument3 pagesNCP ThoracostomyMark Zedrix MediarioNo ratings yet
- F DrugsDocument3 pagesF DrugsChesca LayosaNo ratings yet
- Aplastic AnemiaDocument6 pagesAplastic AnemiaJoezer Gumangan VeranoNo ratings yet
- Proposed Davao Occidental Provincial HospitalDocument3 pagesProposed Davao Occidental Provincial HospitalKenneth BermudezNo ratings yet
- 17 Human Health and Disease: SolutionsDocument64 pages17 Human Health and Disease: SolutionsKirtan ShuklaNo ratings yet
- Textbook Ebook Nutritional Fish and Shrimp Pathology A Handbook European Association of Fish Pathologists Eafp 5M Books Series Tran All Chapter PDFDocument43 pagesTextbook Ebook Nutritional Fish and Shrimp Pathology A Handbook European Association of Fish Pathologists Eafp 5M Books Series Tran All Chapter PDFnicholas.stone880100% (6)
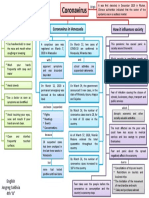
- Mapa Mental Coronavirus en InglesDocument1 pageMapa Mental Coronavirus en InglestavimayrNo ratings yet
- Obstetric ShockDocument65 pagesObstetric Shockkqz39931No ratings yet
- Hesi Med Surg-14Document1 pageHesi Med Surg-14GeorgeNo ratings yet
- Sust Nov'19 (Rafi) PDFDocument10 pagesSust Nov'19 (Rafi) PDFFahad2036No ratings yet
- Questionnaire On The Knowledge, Attitude, and Practices Towards COVID-19Document4 pagesQuestionnaire On The Knowledge, Attitude, and Practices Towards COVID-19Mae GonzalesNo ratings yet
- Miler Bianca MariaDocument3 pagesMiler Bianca MariaBianca MilerNo ratings yet
- AssignmentDocument14 pagesAssignmentAseer KhanNo ratings yet