You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- National Clinical Guideline For Stroke in Secondary CareDocument25 pagesNational Clinical Guideline For Stroke in Secondary CareSebastian SalvadorNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Endoscopic Surgical Management of Intracranial SymDocument15 pagesEndoscopic Surgical Management of Intracranial SymSebastian SalvadorNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Decompressive Craniectomy in Children With Severe Traumatic Brain Injury: A Multicenter Retrospective Study and Literature ReviewDocument8 pagesDecompressive Craniectomy in Children With Severe Traumatic Brain Injury: A Multicenter Retrospective Study and Literature ReviewSebastian SalvadorNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- (10920684 - Neurosurgical Focus) Traumatic Brain Injury in Pediatric Patients - Evidence For The Effectiveness of Decompressive SurgeryDocument8 pages(10920684 - Neurosurgical Focus) Traumatic Brain Injury in Pediatric Patients - Evidence For The Effectiveness of Decompressive SurgerySebastian SalvadorNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Cancers: New Developments in The Pathogenesis, Therapeutic Targeting, and Treatment of Pediatric MedulloblastomaDocument15 pagesCancers: New Developments in The Pathogenesis, Therapeutic Targeting, and Treatment of Pediatric MedulloblastomaSebastian SalvadorNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Endoscopic Third Ventriculostomy in The Treatment of Hydrocephalus in Pediatric PatientsDocument101 pagesEndoscopic Third Ventriculostomy in The Treatment of Hydrocephalus in Pediatric PatientsSebastian SalvadorNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Journal Pre-Proof: European Journal of Paediatric NeurologyDocument31 pagesJournal Pre-Proof: European Journal of Paediatric NeurologySebastian SalvadorNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Opab 314Document7 pagesOpab 314Sebastian SalvadorNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Glioma Invasion: Mechanisms and Therapeutic Challenges: Mariano S. Viapiano Sean E. LawlerDocument35 pagesGlioma Invasion: Mechanisms and Therapeutic Challenges: Mariano S. Viapiano Sean E. LawlerSebastian SalvadorNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Clasificacion de Tumores Cerebreales de La OMS 2016 Articulo de RevisionDocument17 pagesClasificacion de Tumores Cerebreales de La OMS 2016 Articulo de RevisionSebastian SalvadorNo ratings yet
- Acromegaly: Excess Growth Hormone SecretionDocument4 pagesAcromegaly: Excess Growth Hormone SecretionKavita PathakNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- NCM 116 Endocrine DisordersDocument106 pagesNCM 116 Endocrine DisordersAnthony Seth AguilandoNo ratings yet
- Radiopharmaceuticas For TherapyDocument357 pagesRadiopharmaceuticas For TherapyRahma Al SharkawyNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Best Practice & Research Clinical Gastroenterology: Zhongzhen Li, MD, Haleh Vaziri, MDDocument11 pagesBest Practice & Research Clinical Gastroenterology: Zhongzhen Li, MD, Haleh Vaziri, MDEliza ToteNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Content 3Document128 pagesContent 3Mohamed AbbasNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Uso de Octreotide en Niños Con Enfermedades GastrointestinalesDocument18 pagesUso de Octreotide en Niños Con Enfermedades GastrointestinalesEliana Pulido DueñasNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Hormone Regulation 1Document20 pagesHormone Regulation 1Manila MedNo ratings yet
- RIZ - Enterocutaneous FistulaDocument35 pagesRIZ - Enterocutaneous FistulaAdiwirya AristiaraNo ratings yet
- Tektrotyd Kit For Radiopharmaceutical Preparation ENG PAR - 09001be681383ac7Document17 pagesTektrotyd Kit For Radiopharmaceutical Preparation ENG PAR - 09001be681383ac7Ruxandra LúthienNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Acromegaly by DR SunilDocument33 pagesAcromegaly by DR Sunilsinan kNo ratings yet
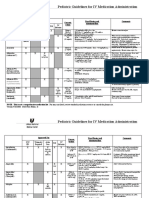
- Pediatric Guidelines For MedicationsDocument24 pagesPediatric Guidelines For MedicationsjonatasmartinezNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- A Case-Based Guide To Clinical Endocrinology (October 23, 2015) - (1493920588) - (Springer)Document434 pagesA Case-Based Guide To Clinical Endocrinology (October 23, 2015) - (1493920588) - (Springer)AbdulraHman KhalEd100% (2)
- EndocrineDocument144 pagesEndocrineaartiNo ratings yet
- Chapter 47 - Endocrine SystemDocument3 pagesChapter 47 - Endocrine SystemStacey100% (1)
- Sleisenger and Fordtrans Gastrointestinal and Liver Disease Review and AssessmentDocument325 pagesSleisenger and Fordtrans Gastrointestinal and Liver Disease Review and AssessmentJimmy Alberto González Castillo100% (2)
- Nutritional Management of Chyle Leaks: An Update: Nutrition Issues in Gastroenterology, Series #94Document13 pagesNutritional Management of Chyle Leaks: An Update: Nutrition Issues in Gastroenterology, Series #94mmmdeandradeNo ratings yet
- Seminars in Pediatric Surgery: Short Bowel Syndrome in Children: Surgical and Medical PerspectivesDocument7 pagesSeminars in Pediatric Surgery: Short Bowel Syndrome in Children: Surgical and Medical PerspectivesrodyNo ratings yet
- Test Bank For Daviss Drug Guide For Nurses 16th Edition VallerandDocument27 pagesTest Bank For Daviss Drug Guide For Nurses 16th Edition VallerandCary Green100% (35)
- 1756 0500 4 344 PDFDocument8 pages1756 0500 4 344 PDFAjeet SinghNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Drugs Affecting The Endocrine SystemDocument43 pagesDrugs Affecting The Endocrine SystemJustine Vens G. AgustinNo ratings yet
- Gastro Colopatia HTPDocument18 pagesGastro Colopatia HTPHernan Del CarpioNo ratings yet
- Ranbaxy Takes The Lions Share: Win A Press & Go Nails PackDocument3 pagesRanbaxy Takes The Lions Share: Win A Press & Go Nails Packapi-139438053No ratings yet
- C. Palpate Neck For Air Bubble Popping SensationDocument4 pagesC. Palpate Neck For Air Bubble Popping SensationNom NomNo ratings yet
- RFDS Western Operations HEA16 - V3.0 Clinical ManualDocument28 pagesRFDS Western Operations HEA16 - V3.0 Clinical ManualJoed BiasonNo ratings yet
- OctreotideDocument3 pagesOctreotideHatim DziauddinNo ratings yet
- Endocrinology-II Past Papers 3rd Year-1Document11 pagesEndocrinology-II Past Papers 3rd Year-1Syed Muhammad HameemNo ratings yet
- NCLEX Review Questions With RationalsDocument32 pagesNCLEX Review Questions With Rationalsmelissamichellle100% (2)
- Pharmacology II - Exam 3 Review (Katzung) Flashcards - QuizletDocument16 pagesPharmacology II - Exam 3 Review (Katzung) Flashcards - Quizletyeshuavelando13No ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Pure Autonomic FailureDocument9 pagesPure Autonomic FailureAnna KolpinaNo ratings yet