You might also like
- ECG Mastery Yellow Belt WorkbookDocument118 pagesECG Mastery Yellow Belt WorkbookOana Anghel100% (9)
- Dystolic Dysfunction Ppt. SalmanDocument42 pagesDystolic Dysfunction Ppt. SalmanMustajab MujtabaNo ratings yet
- Valvular Heart DiseaseDocument27 pagesValvular Heart DiseaseOwen J. WieseNo ratings yet
- Arterial Spectral Doppler WaveformDocument21 pagesArterial Spectral Doppler WaveformL0v3B00k5100% (6)
- Assessing Potential Divers Congenital Heart DiseaseDocument5 pagesAssessing Potential Divers Congenital Heart Diseasetonylee24No ratings yet
- Echocardiographic Assessment of Diastolic Function and Diagnosis of Diastolic Heart FailureDocument15 pagesEchocardiographic Assessment of Diastolic Function and Diagnosis of Diastolic Heart FailureDian HasanahNo ratings yet
- Diastolic Heart Failure AssessmentDocument16 pagesDiastolic Heart Failure AssessmentMd. ashfaque Ahemmed khanNo ratings yet
- Clinical Implications of Left Atrial Enlargement - A ReviewDocument6 pagesClinical Implications of Left Atrial Enlargement - A ReviewRMO RSJDNo ratings yet
- Grade 1 Pattern of LV Diastolic FillingDocument3 pagesGrade 1 Pattern of LV Diastolic FillingNicoleNo ratings yet
- Diastolic Dys Func Tion Asalinkbetween Hypertension A ND Hear T FailureDocument18 pagesDiastolic Dys Func Tion Asalinkbetween Hypertension A ND Hear T FailureCristian AltunaNo ratings yet
- DiastologiaDocument10 pagesDiastologiaReinaldo Pacheco VásquezNo ratings yet
- 10 1016@j Echo 2018 11 011Document19 pages10 1016@j Echo 2018 11 011Jose Ignacio Tarton SisimitNo ratings yet
- Heart Failure With Normal Ejection Fraction (HFNEF) : Is It Worth Considering?Document7 pagesHeart Failure With Normal Ejection Fraction (HFNEF) : Is It Worth Considering?bhaskarpurushottamNo ratings yet
- Mala Goli 2018Document9 pagesMala Goli 2018ErtanNo ratings yet
- 67-Article Text-115-1-10-20171026Document5 pages67-Article Text-115-1-10-20171026Maria MiripNo ratings yet
- ICRJ-Validation of Cornell Product As A Method of Assessing Left Ventricular HypertrophyDocument5 pagesICRJ-Validation of Cornell Product As A Method of Assessing Left Ventricular Hypertrophysamir raflaNo ratings yet
- Agustus Monitoring HemodinamikDocument61 pagesAgustus Monitoring HemodinamikFikriYTNo ratings yet
- Management of Right Ventricular Failure in Pulmonary EmbolisDocument11 pagesManagement of Right Ventricular Failure in Pulmonary EmbolissamuelNo ratings yet
- Poster Session I: Thursday 10 December 2009, 08:30 - 12:30 Location: Poster AreaDocument31 pagesPoster Session I: Thursday 10 December 2009, 08:30 - 12:30 Location: Poster AreaK Danam Nadar RajanNo ratings yet
- Characteristics of Left Ventricular Diastolic Dysfunction in The Community: An Echocardiographic SurveyDocument7 pagesCharacteristics of Left Ventricular Diastolic Dysfunction in The Community: An Echocardiographic SurveyPaul AsturbiarisNo ratings yet
- Diastolic CHF DiagnosisDocument3 pagesDiastolic CHF DiagnosissamNo ratings yet
- Transesophageal Echocardiography: The Hemodynamic Monitoring UtilizingDocument14 pagesTransesophageal Echocardiography: The Hemodynamic Monitoring UtilizingvegasbabyNo ratings yet
- Role of Echocardiography in Atrial Fibrillation Ablation: Andrew C. Y. To MBCHB, Allan L. Klein MDDocument14 pagesRole of Echocardiography in Atrial Fibrillation Ablation: Andrew C. Y. To MBCHB, Allan L. Klein MDsarahNo ratings yet
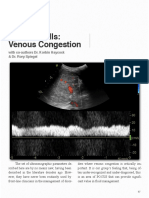
- Venous Congestion ChapterDocument8 pagesVenous Congestion ChapterpcarrascoeNo ratings yet
- Heart Failure With Preserved Ejection Fraction HF PEF A Mini ReviewDocument3 pagesHeart Failure With Preserved Ejection Fraction HF PEF A Mini ReviewPaul HartingNo ratings yet
- Left Atrial Expansion Index Predicts All-Cause Mortality and Heart Failure Admissions in DyspnoeaDocument8 pagesLeft Atrial Expansion Index Predicts All-Cause Mortality and Heart Failure Admissions in DyspnoeaMathew McCarthyNo ratings yet
- Heart Failure and AnaesthesiaDocument7 pagesHeart Failure and AnaesthesiaShinta RizkyNo ratings yet
- Jev 149Document2 pagesJev 149Flavio RibeiroNo ratings yet
- Effect of Right Ventricular Function and Pulmonary Pressures On Heart Failure PrognosisDocument7 pagesEffect of Right Ventricular Function and Pulmonary Pressures On Heart Failure PrognosisMatthew MckenzieNo ratings yet
- Jeac123 PDFDocument3 pagesJeac123 PDFRaquel AguilarNo ratings yet
- 12015exr PDFDocument10 pages12015exr PDFWahidur Rahman RafsanNo ratings yet
- With Increasing Age There Is A Gradual Decrease in The Rate: Restrictive Filling Versus Restrictive CardiomyopathyDocument0 pagesWith Increasing Age There Is A Gradual Decrease in The Rate: Restrictive Filling Versus Restrictive Cardiomyopathydani7MAUNo ratings yet
- 0249 Assessment of Left Ventricle Filling Using in Annas ArchiveDocument1 page0249 Assessment of Left Ventricle Filling Using in Annas Archiveqe202300No ratings yet
- Underwriting LVH 1992Document6 pagesUnderwriting LVH 1992Nisa FjrNo ratings yet
- Diastolic Heart Failure A Disorder of The Elderly Patient - 46PDocument46 pagesDiastolic Heart Failure A Disorder of The Elderly Patient - 46PproctaNo ratings yet
- Pericardial Disease: Adel Hasanin Ahmed 1Document5 pagesPericardial Disease: Adel Hasanin Ahmed 1Shaz ChindhyNo ratings yet
- Right Atrial Pressure in The Critically Ill: How To Measure, What Is The Value, What Are The Limitations?Document9 pagesRight Atrial Pressure in The Critically Ill: How To Measure, What Is The Value, What Are The Limitations?Trần Quang HuyNo ratings yet
- Contin Educ Anaesth Crit Care Pain-2010-Eyre-59-62Document4 pagesContin Educ Anaesth Crit Care Pain-2010-Eyre-59-62deadbysunriseeNo ratings yet
- Mond Illo 2011Document11 pagesMond Illo 2011Triệu Khánh VinhNo ratings yet
- The Role of Echocardiography in The Diagnosis Of: Hypertensiv E Heart DiseaseDocument38 pagesThe Role of Echocardiography in The Diagnosis Of: Hypertensiv E Heart DiseasewidiyaNo ratings yet
- PDF 7Document11 pagesPDF 7bourezgsofiane3500No ratings yet
- The Role and Clinical Implications of DiastolicDocument8 pagesThe Role and Clinical Implications of DiastolicGaal PinNo ratings yet
- VExUS Nexus Bedside Assessment of Venous CongestiDocument10 pagesVExUS Nexus Bedside Assessment of Venous Congestilegap27No ratings yet
- Weber 2002Document12 pagesWeber 2002Wisnu Zeus SullivanNo ratings yet
- 1207 Angela Morello Constrictive PericarditisDocument53 pages1207 Angela Morello Constrictive PericarditisMuhammad JazibNo ratings yet
- Systolic and Diastolic Function in Congestive Heart Failure Pediatric PatientsDocument10 pagesSystolic and Diastolic Function in Congestive Heart Failure Pediatric PatientsMiguelNo ratings yet
- Hemodynamic Monitoring ModalitiesDocument14 pagesHemodynamic Monitoring Modalitiesrudy sanabriaNo ratings yet
- Moderate To Severe ASDocument7 pagesModerate To Severe ASTheresia Sri RezekiNo ratings yet
- Diastole and AnesthesiaDocument16 pagesDiastole and AnesthesiadrsubramanianNo ratings yet
- Evaluation of Diastolic Function With Doppler Echocardiography: The PDF FormalismDocument10 pagesEvaluation of Diastolic Function With Doppler Echocardiography: The PDF Formalismjhon contrerasNo ratings yet
- Arterial DopplerDocument29 pagesArterial DopplerAudrey100% (20)
- Jcu 17 127 PDFDocument8 pagesJcu 17 127 PDFRezkyFYNo ratings yet
- CHAPTER 27 - Heart Failure With A Preserved Ejection FractionDocument15 pagesCHAPTER 27 - Heart Failure With A Preserved Ejection FractionReda SoNo ratings yet
- Pitfalls in Anesthesia MonitoringDocument56 pagesPitfalls in Anesthesia MonitoringDr.Sandeep Kumar Kar100% (1)
- Diastolic Dysfunction Heart FailureDocument46 pagesDiastolic Dysfunction Heart FailureChadi Alraies100% (4)
- Howtotreatrightheart Failure - Tipsforclinicians IneverydaypracticeDocument11 pagesHowtotreatrightheart Failure - Tipsforclinicians IneverydaypracticesaqqarazoserNo ratings yet
- Hemodynamic Monitoring Pocket CardDocument5 pagesHemodynamic Monitoring Pocket CardFitz JaminitNo ratings yet
- Howtotreatrightheart Failure - Tipsforclinicians IneverydaypracticeDocument11 pagesHowtotreatrightheart Failure - Tipsforclinicians IneverydaypracticeIsrael David Villalba FonsecaNo ratings yet
- Central Venous Pressure: Its Clinical Use and Role in Cardiovascular DynamicsFrom EverandCentral Venous Pressure: Its Clinical Use and Role in Cardiovascular DynamicsNo ratings yet
- Congenital Heart Disease: The Catheterization ManualFrom EverandCongenital Heart Disease: The Catheterization ManualLisa BergersenNo ratings yet
- Genome-Wide Search For Schizophrenia Susceptibility Loci: The NIMH Genetics InitiativeDocument7 pagesGenome-Wide Search For Schizophrenia Susceptibility Loci: The NIMH Genetics InitiativePaul AsturbiarisNo ratings yet
- Shaw1998 PDFDocument13 pagesShaw1998 PDFPaul AsturbiarisNo ratings yet
- Thin Solid Films, 196: (1991) 35-46 Electronics and OpticsDocument12 pagesThin Solid Films, 196: (1991) 35-46 Electronics and OpticsPaul AsturbiarisNo ratings yet
- Journal of Pharmaceutical and Biomedical AnalysisDocument7 pagesJournal of Pharmaceutical and Biomedical AnalysisPaul AsturbiarisNo ratings yet
- Thin Film and Interface Group, Department of Physics, University of Exeter, Exeter Devon EX4 4QL, UKDocument4 pagesThin Film and Interface Group, Department of Physics, University of Exeter, Exeter Devon EX4 4QL, UKPaul AsturbiarisNo ratings yet
- Impact of Diastolic Dysfunction Grade On Left Atrial Mechanics Assessed by Two-Dimensional Speckle Tracking EchocardiographyDocument7 pagesImpact of Diastolic Dysfunction Grade On Left Atrial Mechanics Assessed by Two-Dimensional Speckle Tracking EchocardiographyPaul AsturbiarisNo ratings yet
- Direct Measurement of Cold Neutron Moderator Spectra: Article in PressDocument5 pagesDirect Measurement of Cold Neutron Moderator Spectra: Article in PressPaul AsturbiarisNo ratings yet
- Shammas 2007Document9 pagesShammas 2007Paul AsturbiarisNo ratings yet
- Characteristics of Left Ventricular Diastolic Dysfunction in The Community: An Echocardiographic SurveyDocument7 pagesCharacteristics of Left Ventricular Diastolic Dysfunction in The Community: An Echocardiographic SurveyPaul AsturbiarisNo ratings yet
- Feminist Legal Studies Volume 5 Issue 2 1997 (Doi 10.1007 - bf02684881) Patricia Moynihan - Ariadne and The "Pathos of Distance" - Re-Considering Judgment in Feminist CriminologyDocument30 pagesFeminist Legal Studies Volume 5 Issue 2 1997 (Doi 10.1007 - bf02684881) Patricia Moynihan - Ariadne and The "Pathos of Distance" - Re-Considering Judgment in Feminist CriminologyPaul AsturbiarisNo ratings yet
- PCL's Analysis of Thermal Hazards On Offshore Structures (PATHOS 2)Document6 pagesPCL's Analysis of Thermal Hazards On Offshore Structures (PATHOS 2)Paul AsturbiarisNo ratings yet
- Bemisia TabaciDocument7 pagesBemisia TabaciPaul AsturbiarisNo ratings yet
- Fibrinogen Allele Frequencies in Peruvian Quechua, A High-Altitude Native PopulationDocument6 pagesFibrinogen Allele Frequencies in Peruvian Quechua, A High-Altitude Native PopulationPaul AsturbiarisNo ratings yet
- Correadesa 2010Document6 pagesCorreadesa 2010Paul AsturbiarisNo ratings yet
- Argumentation Volume 6 Issue 3 1992 (Doi 10.1007 - bf00154696) Antoine C. Braet - Ethos, Pathos and Logos in Aristotle's Rhetoric - A Re-ExaminationDocument14 pagesArgumentation Volume 6 Issue 3 1992 (Doi 10.1007 - bf00154696) Antoine C. Braet - Ethos, Pathos and Logos in Aristotle's Rhetoric - A Re-ExaminationPaul AsturbiarisNo ratings yet
- Mechanisms of Resistance To Acetyl-Coenzyme A Carboxylase Inhibitors: A ReviewDocument6 pagesMechanisms of Resistance To Acetyl-Coenzyme A Carboxylase Inhibitors: A ReviewPaul AsturbiarisNo ratings yet
- Locally Pelvic Advanced Rectal Cancer Kidney Complicating Adjuvant Radiation TherapyDocument4 pagesLocally Pelvic Advanced Rectal Cancer Kidney Complicating Adjuvant Radiation TherapyPaul AsturbiarisNo ratings yet
- Lethal and Sublethal Effects of Imidacloprid Nicotine-Tolerant andDocument6 pagesLethal and Sublethal Effects of Imidacloprid Nicotine-Tolerant andPaul AsturbiarisNo ratings yet
- Sexual Dimorphism in The Pelvic Midplane and Its Relationship To Neandertal Reproductive PatternsDocument12 pagesSexual Dimorphism in The Pelvic Midplane and Its Relationship To Neandertal Reproductive PatternsPaul AsturbiarisNo ratings yet
- Salah A. Alhumood, Dana V. Devine, Laurie Lawson, Stephen H. Nantel, and Cedric J. CarterDocument7 pagesSalah A. Alhumood, Dana V. Devine, Laurie Lawson, Stephen H. Nantel, and Cedric J. CarterPaul AsturbiarisNo ratings yet
- Prenatal Growth Retardation, Pelvic Hypoplasia, and Arthrogrypotic Changes of Lower LimbsDocument8 pagesPrenatal Growth Retardation, Pelvic Hypoplasia, and Arthrogrypotic Changes of Lower LimbsPaul AsturbiarisNo ratings yet
- Preoperative Angiography and Embolization of Large Pelvic TumorsDocument4 pagesPreoperative Angiography and Embolization of Large Pelvic TumorsPaul AsturbiarisNo ratings yet
- Little Languages: Little Maintenance? : PracticeDocument18 pagesLittle Languages: Little Maintenance? : PracticePaul AsturbiarisNo ratings yet
- Letters: R. S. Lindsay, J. A. Little, A. J. Jaap, P. L. Padfield, J. D. Walker, K. J. HardyDocument1 pageLetters: R. S. Lindsay, J. A. Little, A. J. Jaap, P. L. Padfield, J. D. Walker, K. J. HardyPaul AsturbiarisNo ratings yet
- Pelvic Lymphocysts Following Retroperitoneal Lymphadenectomy: Retroperitoneal Partial No-Closure'' For Ovarian and Endometrial CancersDocument4 pagesPelvic Lymphocysts Following Retroperitoneal Lymphadenectomy: Retroperitoneal Partial No-Closure'' For Ovarian and Endometrial CancersPaul AsturbiarisNo ratings yet
- Femtosecond Dynamics of Dioxygen Picket-Fence Cobalt Porphyrins: Ultrafast Release of O and The Nature of Dative BondingDocument4 pagesFemtosecond Dynamics of Dioxygen Picket-Fence Cobalt Porphyrins: Ultrafast Release of O and The Nature of Dative BondingPaul AsturbiarisNo ratings yet
- Cloning Candidate Genes Involved in The Beckwith-Wiedemann Syndrome and Childhood TumorsDocument3 pagesCloning Candidate Genes Involved in The Beckwith-Wiedemann Syndrome and Childhood TumorsPaul AsturbiarisNo ratings yet
- Femtosecond Dynamics of Dioxygen Picket-Fence Cobalt Porphyrins: Ultrafast Release of O and The Nature of Dative BondingDocument4 pagesFemtosecond Dynamics of Dioxygen Picket-Fence Cobalt Porphyrins: Ultrafast Release of O and The Nature of Dative BondingPaul AsturbiarisNo ratings yet
- NCM 106 Cardiac DrugsDocument111 pagesNCM 106 Cardiac DrugsKatie HolmesNo ratings yet
- Solutions AIATS Medical-2017 Test-3 (Code-A B) (18!12!2016)Document24 pagesSolutions AIATS Medical-2017 Test-3 (Code-A B) (18!12!2016)HaRry0% (1)
- Myocarditis Diagnosis AdultsDocument44 pagesMyocarditis Diagnosis AdultsGiga HasabiNo ratings yet
- Soak Feet With Warm Water and Progressive Muscle Relaxation Therapy On Blood Pressure in Hypertension ElderlyDocument5 pagesSoak Feet With Warm Water and Progressive Muscle Relaxation Therapy On Blood Pressure in Hypertension ElderlyInda MegaNo ratings yet
- Textbook Paediatrics A Core Text On Child Health Second Edition Tony Waterston Ebook All Chapter PDFDocument50 pagesTextbook Paediatrics A Core Text On Child Health Second Edition Tony Waterston Ebook All Chapter PDFhelen.black690100% (4)
- Food Uses of GingerDocument7 pagesFood Uses of Gingerbash kinedNo ratings yet
- Secure Your Family Against Uncertainties, With A Plan That Adjusts To Your NeedsDocument25 pagesSecure Your Family Against Uncertainties, With A Plan That Adjusts To Your Needsroxcox216No ratings yet
- Perioperative CareDocument53 pagesPerioperative Caregugu888100% (2)
- Multiple-Choice Test Chapter 9: Transport in Humans: 1 A B C D 2 A B C D 3 A B C D 4 A B C D 5 A B C DDocument2 pagesMultiple-Choice Test Chapter 9: Transport in Humans: 1 A B C D 2 A B C D 3 A B C D 4 A B C D 5 A B C DsybejoboNo ratings yet
- Forensic Autopsy ProtocolDocument12 pagesForensic Autopsy Protocolapi-3701786100% (1)
- PHCP FinalsDocument75 pagesPHCP FinalsSamantha SantosNo ratings yet
- Principles of Treatment of IhdDocument3 pagesPrinciples of Treatment of IhdArvinth Guna SegaranNo ratings yet
- Atrial Septal DefectDocument3 pagesAtrial Septal Defectktin17No ratings yet
- Speaking Test Avcn 1: Unit 1: Hospital StaffDocument5 pagesSpeaking Test Avcn 1: Unit 1: Hospital StaffHoàng Huy NguyễnNo ratings yet
- Ex - Drugs On BP and Heart Rate of DogDocument5 pagesEx - Drugs On BP and Heart Rate of DogAryan Pisat100% (1)
- Ahs Question Bank Second Year MedicineDocument17 pagesAhs Question Bank Second Year MedicineAdhithiayan ANo ratings yet
- Capillary Refill Time Exploration During Septic ShockDocument8 pagesCapillary Refill Time Exploration During Septic ShockVictoriano ValienteNo ratings yet
- Accurate Recognition of Coronary Artery Disease by Applying Machine Learning ClassifiersDocument6 pagesAccurate Recognition of Coronary Artery Disease by Applying Machine Learning ClassifiersKawshik BanerjeeNo ratings yet
- Science 6 - Q2 - Test No 3Document2 pagesScience 6 - Q2 - Test No 3MARY JANE PALISPISNo ratings yet
- Module 8. Animal Organ SystemDocument151 pagesModule 8. Animal Organ SystemMarkAnthony PagaNo ratings yet
- Orem's Assessment GuideDocument39 pagesOrem's Assessment Guidemaynard bairdNo ratings yet
- Vital SignsDocument3 pagesVital SignsNicole NipasNo ratings yet
- Care of The Chronically Ill and The Older PersonDocument8 pagesCare of The Chronically Ill and The Older PersonAnne Con100% (1)
- Doctors OpinionDocument30 pagesDoctors Opinionitsjai1303m80100% (1)
- Chest X Ray - BasicsDocument4 pagesChest X Ray - BasicsEd ChangNo ratings yet
- Overview of Cardiovascular System: An Introduction To Chapters 9 - 24 and Chapter 36 Guyton and Hall, 12 EditionDocument10 pagesOverview of Cardiovascular System: An Introduction To Chapters 9 - 24 and Chapter 36 Guyton and Hall, 12 EditionbahahahahNo ratings yet
- Levine 1967 Nursing ForumDocument15 pagesLevine 1967 Nursing ForumJelly Bean100% (1)
- ANPH Midterm NotesDocument44 pagesANPH Midterm NotesClaudine Jo B. TalabocNo ratings yet
- Cardiogenic ShockDocument42 pagesCardiogenic ShockpashaNo ratings yet