You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Male Urethritis With or Without Discharge A ClinicDocument5 pagesMale Urethritis With or Without Discharge A ClinicDian FitriNo ratings yet
- MJMHS 0173Document3 pagesMJMHS 0173YudistiraJefriRamadhanNo ratings yet
- INDIKATOR WHO-GIZI ANAK HabibDocument12 pagesINDIKATOR WHO-GIZI ANAK HabibYudistiraJefriRamadhanNo ratings yet
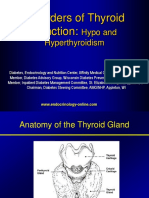
- Disorders of Thyroid Function Kulpak PDFDocument59 pagesDisorders of Thyroid Function Kulpak PDFYudistiraJefriRamadhanNo ratings yet
- Calcium Metabolism: Dr. Joko Wahyu Wibowo MkesDocument46 pagesCalcium Metabolism: Dr. Joko Wahyu Wibowo MkesYudistiraJefriRamadhanNo ratings yet
- Minimally Invasive Surgery Alone Compared With Intensity-Modulated Radiotherapy For Primary Stage I Nasopharyngeal CarcinomaDocument11 pagesMinimally Invasive Surgery Alone Compared With Intensity-Modulated Radiotherapy For Primary Stage I Nasopharyngeal CarcinomaYudistiraJefriRamadhanNo ratings yet
- Tiroid PDFDocument17 pagesTiroid PDFYudistiraJefriRamadhanNo ratings yet
- The Adrenal Cortex Hormone C/O: Glucocorticoids, Mineralocorticoids, AndrogensDocument22 pagesThe Adrenal Cortex Hormone C/O: Glucocorticoids, Mineralocorticoids, AndrogensYudistiraJefriRamadhanNo ratings yet
- Laryngopharyngeal Reflux Disease - LPRD: Professional PaperDocument4 pagesLaryngopharyngeal Reflux Disease - LPRD: Professional PaperAndi Tiara S. AdamNo ratings yet
- Complication of Diabetes MellitusDocument51 pagesComplication of Diabetes MellitusAde Yurga TonaraNo ratings yet
- Minimally Invasive Surgery Alone Compared With Intensity-Modulated Radiotherapy For Primary Stage I Nasopharyngeal CarcinomaDocument11 pagesMinimally Invasive Surgery Alone Compared With Intensity-Modulated Radiotherapy For Primary Stage I Nasopharyngeal CarcinomaYudistiraJefriRamadhanNo ratings yet
- Double Dummy TechniqueDocument2 pagesDouble Dummy TechniqueBelinda Putri AgustiaNo ratings yet
- KudaDocument10 pagesKudaYudistiraJefriRamadhanNo ratings yet
- The Adrenal Cortex Hormone C/O: Glucocorticoids, Mineralocorticoids, AndrogensDocument22 pagesThe Adrenal Cortex Hormone C/O: Glucocorticoids, Mineralocorticoids, AndrogensYudistiraJefriRamadhanNo ratings yet
- Mata 1Document10 pagesMata 1YudistiraJefriRamadhanNo ratings yet
- Daftar Isi BagilDocument11 pagesDaftar Isi BagilYudistiraJefriRamadhanNo ratings yet
- FULLTEXT01Document10 pagesFULLTEXT01YudistiraJefriRamadhanNo ratings yet
- Deck List: GT Pantura 2014Document1 pageDeck List: GT Pantura 2014YudistiraJefriRamadhanNo ratings yet
- Journal ReadingDocument17 pagesJournal ReadingYudistiraJefriRamadhanNo ratings yet
- KudaDocument10 pagesKudaYudistiraJefriRamadhanNo ratings yet
- Bawang Putih 1 PDFDocument8 pagesBawang Putih 1 PDFYudistiraJefriRamadhanNo ratings yet
- Contracting Skeletal Muscle Generates An Increased Amount 1Document2 pagesContracting Skeletal Muscle Generates An Increased Amount 1YudistiraJefriRamadhanNo ratings yet
- Hasil Ujian Mid Modul Reproduksi Tanggal 15 November 2014Document1 pageHasil Ujian Mid Modul Reproduksi Tanggal 15 November 2014YudistiraJefriRamadhanNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Cayo West PDFDocument127 pagesCayo West PDFSeinsu ManNo ratings yet
- The 5 Types of Female OrgasmsDocument16 pagesThe 5 Types of Female OrgasmsKriketNo ratings yet
- Assessment of Fetal Growth and DevelopmentDocument12 pagesAssessment of Fetal Growth and Developmentaracelisurat100% (1)
- Sex Toys: November 2020Document11 pagesSex Toys: November 2020Luky SubiantoroNo ratings yet
- Science 5Document81 pagesScience 5Michael Joseph Santos100% (2)
- Exhibicionismo y Vouyerismo CompulsivoDocument8 pagesExhibicionismo y Vouyerismo CompulsivoPsiquiatria Hospital Cayetano HerediaNo ratings yet
- Purpose:: Procedure: Rationale: Introduce Yourself and Inform Pregnant Woman About The ProcedureDocument5 pagesPurpose:: Procedure: Rationale: Introduce Yourself and Inform Pregnant Woman About The ProcedureArmySapphireNo ratings yet
- Partograf 1 PDFDocument6 pagesPartograf 1 PDFnurlatifahNo ratings yet
- Who Feels It Knows: The Challenges of HIV Prevention For Young Black Women in TorontoDocument56 pagesWho Feels It Knows: The Challenges of HIV Prevention For Young Black Women in TorontoOwn VolitionNo ratings yet
- Hinanay - SSG 3 CmcaDocument3 pagesHinanay - SSG 3 CmcaHenie Louise HinanayNo ratings yet
- A2 Calling A Neonatal Team To Delivery Suitefeb2014Document3 pagesA2 Calling A Neonatal Team To Delivery Suitefeb2014madimadi11No ratings yet
- The Male BrainDocument2 pagesThe Male Brainimoez imoetNo ratings yet
- Incest Taboo and FamilyDocument21 pagesIncest Taboo and FamilyOjasvi Monga100% (1)
- PumadesDocument46 pagesPumadesIrwin FitriansyahNo ratings yet
- Instrumental DeliveryDocument25 pagesInstrumental DeliveryAhmed ElmohandesNo ratings yet
- NCM 109 Week 7 1Document47 pagesNCM 109 Week 7 1Stephanie Ann ZanoriaNo ratings yet
- Oogenesis and The Ovarian Cycle: Angelbert R. Bacongco Justin Rhea M. BandiolaDocument19 pagesOogenesis and The Ovarian Cycle: Angelbert R. Bacongco Justin Rhea M. BandiolaJustin Rhea BandiolaNo ratings yet
- Human Development and Human BehaviorDocument11 pagesHuman Development and Human BehaviormirtchNo ratings yet
- Post Partum Family Planning/Planification Familiale Du Post - PartumDocument18 pagesPost Partum Family Planning/Planification Familiale Du Post - PartumJhpiego100% (2)
- Estimating EDC and fetal age with Naegele's, McDonald's, Bartholome's and Johnson's RulesDocument6 pagesEstimating EDC and fetal age with Naegele's, McDonald's, Bartholome's and Johnson's RulesREANNE MAE ABRERANo ratings yet
- Reproductive Health SK SinghDocument31 pagesReproductive Health SK SinghKUNAL KISHORENo ratings yet
- Natasha Nice Cumshot. Top Adult FREE Pic. Comments 1 2Document1 pageNatasha Nice Cumshot. Top Adult FREE Pic. Comments 1 2stellamabel58No ratings yet
- San Pedro Hospital of Davao City, Inc. - Doctor's Directory - Ob-Gyne SCHEDULEDocument5 pagesSan Pedro Hospital of Davao City, Inc. - Doctor's Directory - Ob-Gyne SCHEDULEVanessa ManuelNo ratings yet
- Modern Sex TechniquesDocument233 pagesModern Sex TechniquesOreja Checho60% (5)
- TatarinDocument2 pagesTatarinXandae Mempin100% (1)
- Determinant Factors That Influence The Prevalence of Gonorrhea in Female Sex Wokers in YogyakartaDocument12 pagesDeterminant Factors That Influence The Prevalence of Gonorrhea in Female Sex Wokers in YogyakartaSiti MaesarohNo ratings yet
- Act Providing For A Nat Ional Policy On Responsible Parent Hood and Reproduct Ive Healt HDocument14 pagesAct Providing For A Nat Ional Policy On Responsible Parent Hood and Reproduct Ive Healt HChris EstalloNo ratings yet
- Menstrual Cycle and Physical Performance of Female AthletesDocument3 pagesMenstrual Cycle and Physical Performance of Female AthletesBiee BarbNo ratings yet
- Zambia ANC Guidelines 2022 - Print ReadyDocument44 pagesZambia ANC Guidelines 2022 - Print ReadyMibenge MichaelNo ratings yet
- An Islamic View On Contraception and AbortionDocument4 pagesAn Islamic View On Contraception and AbortionhahaNo ratings yet