You might also like
- Competency MappingDocument20 pagesCompetency MappingMalleyboina NagarajuNo ratings yet
- Manual of HR Administration Policies RegulationsDocument101 pagesManual of HR Administration Policies Regulationshr hrNo ratings yet
- Chur Human Resource ProcessDocument5 pagesChur Human Resource Processvickyanam1978No ratings yet
- Employment ContractDocument3 pagesEmployment ContractMA FATIMAH VELASCO VILLANUEVANo ratings yet
- Free HR Incident Investigation FormDocument2 pagesFree HR Incident Investigation FormRichard R M ThodéNo ratings yet
- HR Calender & ActivitiesDocument9 pagesHR Calender & ActivitiesAnandReddyNo ratings yet
- Employee Joining Form: A-238 (N), Oppo. Mangala Sariya Road No. 09, VKI Area, Jaipur-302013Document2 pagesEmployee Joining Form: A-238 (N), Oppo. Mangala Sariya Road No. 09, VKI Area, Jaipur-302013VAIBHAV JAKHALIANo ratings yet
- RecruitmentDocument1 pageRecruitmentDimas YudiNo ratings yet
- Process of HR Dept.Document5 pagesProcess of HR Dept.VINAY SINGHNo ratings yet
- Recruitment Selection Process in A CompanyDocument5 pagesRecruitment Selection Process in A CompanySudamBeheraNo ratings yet
- WGU C233 Employment LawDocument60 pagesWGU C233 Employment LawGene's100% (1)
- R.R. Ispat (A Unit of Gpil) : Recruitment PolicyDocument3 pagesR.R. Ispat (A Unit of Gpil) : Recruitment PolicyVinod KumarNo ratings yet
- ArellanoDocument10 pagesArellanoLeidi Chua BayudanNo ratings yet
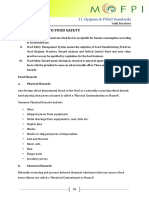
- Legal Compliance Food IndustryDocument37 pagesLegal Compliance Food IndustryUjjwal AnandNo ratings yet
- Hygiene & FSSAI StandardsDocument29 pagesHygiene & FSSAI StandardsSuchithra DeviNo ratings yet
- Employee Accommodation Policy: Ramana Gounder Medical TrustDocument22 pagesEmployee Accommodation Policy: Ramana Gounder Medical TrustAaju KausikNo ratings yet
- Dash Boards For Manufacturing IndustriesDocument3 pagesDash Boards For Manufacturing IndustriesSenthilmani MuthuswamyNo ratings yet
- HR11 1EmployeeSeparation04072018SignedDocument6 pagesHR11 1EmployeeSeparation04072018Signedruchitss100% (1)
- Annual Appraisal Form - Executive CadreDocument3 pagesAnnual Appraisal Form - Executive CadreSripal JainNo ratings yet
- Mis Report 146Document24 pagesMis Report 146Arpita DasNo ratings yet
- SOP-HR-01 (Recruitment Process)Document2 pagesSOP-HR-01 (Recruitment Process)M CNo ratings yet
- Labor Code Article 285: Employee Termination RightsDocument2 pagesLabor Code Article 285: Employee Termination RightsMaybelle100% (1)
- Policy On Performance EvaluationDocument5 pagesPolicy On Performance EvaluationSathish Haran100% (1)
- Clearance Form: Ahamed Aslam 0358/107499 Engineering/HCNS 11.11.2016 29135618448 Mechanical EngineerDocument1 pageClearance Form: Ahamed Aslam 0358/107499 Engineering/HCNS 11.11.2016 29135618448 Mechanical EngineerAslamNo ratings yet
- Skill Matrix SampleDocument14 pagesSkill Matrix SamplekalyangudluruNo ratings yet
- Assistant Professor Gift University Gujranwala: Job DescriptionDocument3 pagesAssistant Professor Gift University Gujranwala: Job DescriptionAli AslamNo ratings yet
- MIS Report For HRDocument10 pagesMIS Report For HRwelcomeumeshNo ratings yet
- JD HR Manager AssignmentDocument3 pagesJD HR Manager AssignmentNashwa El bahnasawyNo ratings yet
- Staff Disciplinary CodeDocument4 pagesStaff Disciplinary CodeOwunari Adaye-OrugbaniNo ratings yet
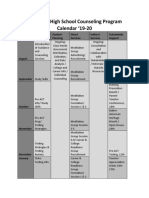
- School Counseling CalendarDocument2 pagesSchool Counseling Calendarapi-438988888No ratings yet
- Training Requisition FormatDocument1 pageTraining Requisition FormatSGNo ratings yet
- Career Pathways TemplateDocument4 pagesCareer Pathways TemplateFaula Iman SitompulNo ratings yet
- Power To People: Indiafirst Employee Benefit PlanDocument14 pagesPower To People: Indiafirst Employee Benefit PlanBhawzNo ratings yet
- Complaint Handling SOP SummaryDocument6 pagesComplaint Handling SOP SummarytesteNo ratings yet
- Perf App Model 2 - For ManagersDocument8 pagesPerf App Model 2 - For ManagersVamsi Krishna NukarajuNo ratings yet
- CISF Training Calendar 2019Document3 pagesCISF Training Calendar 2019Chaudhary RanvijayNo ratings yet
- Employee Gate Pass Form - ABC - OBDocument1 pageEmployee Gate Pass Form - ABC - OBFOODMNL Accounting100% (1)
- Employee Hand Book 03-12-11Document82 pagesEmployee Hand Book 03-12-11Anmohiey100% (1)
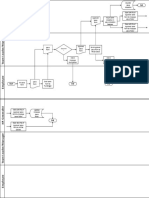
- Leave Policy - FlowchartDocument2 pagesLeave Policy - FlowchartAdid RachmadiansyahNo ratings yet
- HR M Annual Policies 201516Document64 pagesHR M Annual Policies 201516Shereen AbbangöNo ratings yet
- ERP SYSTEM MANAGEMENTDocument9 pagesERP SYSTEM MANAGEMENTRobbin HaidenNo ratings yet
- What is a Skills MatrixDocument3 pagesWhat is a Skills Matrixjagansd3No ratings yet
- Gartner - Reimaginehr-Global-Key-Takeaways-2020Document24 pagesGartner - Reimaginehr-Global-Key-Takeaways-2020PedroNo ratings yet
- Tasc Nbad Joining Form 04062014Document9 pagesTasc Nbad Joining Form 04062014mohd_nasir4uNo ratings yet
- Short Leave FormDocument2 pagesShort Leave FormMohd Javed KhanNo ratings yet
- AC - AMC PLAN - (02-Mar-20) (Split & Cas)Document1 pageAC - AMC PLAN - (02-Mar-20) (Split & Cas)Nilay GandhiNo ratings yet
- Date Name Vehcile No: Item DescriptionDocument2 pagesDate Name Vehcile No: Item DescriptionAnonymous VHB7VDPKNo ratings yet
- QA Roles & ResponsibleDocument5 pagesQA Roles & ResponsibleMohd Ezan MohammadiahNo ratings yet
- Manpower Request FormDocument1 pageManpower Request FormPragathishNo ratings yet
- 3 Kirkpatrick Evaluation Model PaperDocument7 pages3 Kirkpatrick Evaluation Model Papererine5995No ratings yet
- Ehs Training Calendar - 2019Document2 pagesEhs Training Calendar - 2019Ritesh kumarNo ratings yet
- 11 Employees Transfer Request FormDocument1 page11 Employees Transfer Request FormsekarNo ratings yet
- Adecco Escalation Matrix - HCLDocument5 pagesAdecco Escalation Matrix - HCLJaspal KumarNo ratings yet
- KRA For FY 2019-2020: HRDocument3 pagesKRA For FY 2019-2020: HRMohit GuptaNo ratings yet
- Facilities Management OfficeDocument2 pagesFacilities Management OfficeEmieda EraineNo ratings yet
- Form Clearance CheclistDocument2 pagesForm Clearance CheclistMedikaloka House Of HealthNo ratings yet
- Recruitment Policy1 178Document7 pagesRecruitment Policy1 178vinay8464No ratings yet
- Probation and Performance PolicyDocument8 pagesProbation and Performance PolicyAnkitaNo ratings yet
- Joining Kit Sample 2Document15 pagesJoining Kit Sample 2Utkarsh AnandNo ratings yet
- Leave and Attendance Requirements - V2.0Document43 pagesLeave and Attendance Requirements - V2.0simplynotesNo ratings yet
- Genius Joining Kit-1Document8 pagesGenius Joining Kit-1Aditya RajNo ratings yet
- HR PolicyDocument25 pagesHR PolicySaurabh DwivediNo ratings yet
- Survey HR PDFDocument2 pagesSurvey HR PDFMd Saidunnabi JohaNo ratings yet
- Gratuity-Form Form FDocument3 pagesGratuity-Form Form FData. GetNo ratings yet
- Change of Personal Details Form HR 104: Please Complete in Block Capitals and Place A Tick in The Appropriate BoxesDocument3 pagesChange of Personal Details Form HR 104: Please Complete in Block Capitals and Place A Tick in The Appropriate BoxesLexNo ratings yet
- Employee Transfer FormDocument6 pagesEmployee Transfer FormLexNo ratings yet
- HSE HR circular outlines transfer scheme pauseDocument17 pagesHSE HR circular outlines transfer scheme pauseLexNo ratings yet
- Dr. Steevens' Hospital Dublin 8Document4 pagesDr. Steevens' Hospital Dublin 8LexNo ratings yet
- HSE HR Circular Reminder - Deadline for Personal Fund Threshold ApplicationDocument2 pagesHSE HR Circular Reminder - Deadline for Personal Fund Threshold ApplicationLexNo ratings yet
- Circ 01615Document2 pagesCirc 01615LexNo ratings yet
- Dr. Steevens' Hospital Dublin 8: Sean - Keane@hse - IeDocument3 pagesDr. Steevens' Hospital Dublin 8: Sean - Keane@hse - IeLexNo ratings yet
- HSE HR circular outlines transfer scheme pauseDocument17 pagesHSE HR circular outlines transfer scheme pauseLexNo ratings yet
- Dr. Steevens' Hospital Dublin 8: Nurses and Midwives With The Nursing and Midwifery Board of IrelandDocument2 pagesDr. Steevens' Hospital Dublin 8: Nurses and Midwives With The Nursing and Midwifery Board of IrelandLexNo ratings yet
- Dr. Steevens' Hospital Dublin 8: Nurses and Midwives With The Nursing and Midwifery Board of IrelandDocument2 pagesDr. Steevens' Hospital Dublin 8: Nurses and Midwives With The Nursing and Midwifery Board of IrelandLexNo ratings yet
- Dr. Steevens' Hospital Dublin 8Document2 pagesDr. Steevens' Hospital Dublin 8LexNo ratings yet
- HSE HR Circular reduced interest rateDocument5 pagesHSE HR Circular reduced interest rateLexNo ratings yet
- Oifig An Stiúrthóra Náisiúnta, Acmhainní DaonnaDocument2 pagesOifig An Stiúrthóra Náisiúnta, Acmhainní DaonnaLexNo ratings yet
- HSE guidance on supervision for health professionalsDocument18 pagesHSE guidance on supervision for health professionalsLexNo ratings yet
- Oifig An Stiúrthóra Náisiúnta, Acmhainní DaonnaDocument2 pagesOifig An Stiúrthóra Náisiúnta, Acmhainní DaonnaLexNo ratings yet
- Rphost/ E-Mail: Nationalhr@hse - IeDocument2 pagesRphost/ E-Mail: Nationalhr@hse - IeLexNo ratings yet
- Implementing Social Distancing in Health Sector WorkplacesDocument2 pagesImplementing Social Distancing in Health Sector WorkplacesLexNo ratings yet
- Implementing Social Distancing in Health Sector WorkplacesDocument2 pagesImplementing Social Distancing in Health Sector WorkplacesLexNo ratings yet
- Reserve Defence Leave FormDocument2 pagesReserve Defence Leave FormLexNo ratings yet
- Oifig An Stiúrthóra Náisiúnta, Acmhainní DaonnaDocument3 pagesOifig An Stiúrthóra Náisiúnta, Acmhainní DaonnaLexNo ratings yet
- Oifig An Stiúrthóra Náisiúnta, Acmhainní DaonnaDocument2 pagesOifig An Stiúrthóra Náisiúnta, Acmhainní DaonnaLexNo ratings yet
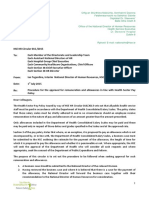
- HR Circular 002 2020 Re Extension of Location Allowance PDFDocument2 pagesHR Circular 002 2020 Re Extension of Location Allowance PDFLexNo ratings yet
- Oifig An Stiúrthóra Náisiúnta, Acmhainní Daonna: Nationalabsence@hse - IeDocument2 pagesOifig An Stiúrthóra Náisiúnta, Acmhainní Daonna: Nationalabsence@hse - IeLexNo ratings yet
- HR Circular 001 2020 Intern Induction 2018 PDFDocument4 pagesHR Circular 001 2020 Intern Induction 2018 PDFLexNo ratings yet
- Special Unpaid Leave Application Form - HR 108 (O) : Section 1. To Be Completed by The EmployeeDocument2 pagesSpecial Unpaid Leave Application Form - HR 108 (O) : Section 1. To Be Completed by The EmployeeLexNo ratings yet
- HR Circular 002 2020 Re Extension of Location Allowance PDFDocument2 pagesHR Circular 002 2020 Re Extension of Location Allowance PDFLexNo ratings yet
- Reserve Defence Leave FormDocument2 pagesReserve Defence Leave FormLexNo ratings yet
- Serious Assault Leave FormDocument3 pagesSerious Assault Leave FormLexNo ratings yet
- HR Circular 001 2020 Intern Induction 2018 PDFDocument4 pagesHR Circular 001 2020 Intern Induction 2018 PDFLexNo ratings yet
- Serious Assault Leave FormDocument3 pagesSerious Assault Leave FormLexNo ratings yet
- Special Unpaid Leave Application Form - HR 108 (O) : Section 1. To Be Completed by The EmployeeDocument2 pagesSpecial Unpaid Leave Application Form - HR 108 (O) : Section 1. To Be Completed by The EmployeeLexNo ratings yet
- HR Circular 001 2020 Intern Induction 2018 PDFDocument4 pagesHR Circular 001 2020 Intern Induction 2018 PDFLexNo ratings yet
- Carsome Employment Application FormDocument9 pagesCarsome Employment Application Formrabiatul adawiyahNo ratings yet
- ER HeritageDocument57 pagesER HeritagekartikNo ratings yet
- Pension RulesDocument230 pagesPension Rulesmacbook28487No ratings yet
- Max Weber Bureaucratic Theory PDFDocument1 pageMax Weber Bureaucratic Theory PDFVeronica TanNo ratings yet
- Human Resource Planning: DR Premalatha.P Adhoc SH&M Nit ApDocument36 pagesHuman Resource Planning: DR Premalatha.P Adhoc SH&M Nit ApSushma NelapatiNo ratings yet
- Eijmrs5242 PDFDocument7 pagesEijmrs5242 PDFDhruvilJakasaniyaNo ratings yet
- Mathadi Act in Marathi Language PDFDocument16 pagesMathadi Act in Marathi Language PDFKrishna Gupta100% (1)
- Alderfer's Erg TheoryDocument6 pagesAlderfer's Erg TheoryAiman MustaqimNo ratings yet
- Interview Preparation TipsDocument4 pagesInterview Preparation TipsElena EreminaNo ratings yet
- Detailed Lesson Plan: I. ObjectivesDocument5 pagesDetailed Lesson Plan: I. ObjectivesPeter TorresNo ratings yet
- Coida Service Book Version 23Document53 pagesCoida Service Book Version 23Lesedi ModibaneNo ratings yet
- Cover Letter Examples Fitness IndustryDocument5 pagesCover Letter Examples Fitness Industryfygemiduwef2100% (1)
- Republic of The Philippines Congress of The Philippines Metro Manila Fifth Regular SessionDocument9 pagesRepublic of The Philippines Congress of The Philippines Metro Manila Fifth Regular SessionDianne YcoNo ratings yet
- Allyza R. Renoballes Human Resource Management Bsba - 3A 04 Elms Quiz 1Document3 pagesAllyza R. Renoballes Human Resource Management Bsba - 3A 04 Elms Quiz 1Allyza RenoballesNo ratings yet
- Advice To All EmployeesDocument2 pagesAdvice To All EmployeesDel RicafortNo ratings yet
- A Case Study of Orissa Power ReformsDocument18 pagesA Case Study of Orissa Power ReformsDileep Shekhawat0% (1)
- EMP20221209 - Memorandum Pay SecrecyDocument2 pagesEMP20221209 - Memorandum Pay SecrecyEvonne TanNo ratings yet
- Part FourDocument3 pagesPart FourHannah CorpuzNo ratings yet
- Revised - Calendar - of - Examination - 2023-2024 - 19052023Document1 pageRevised - Calendar - of - Examination - 2023-2024 - 19052023HUSSAIN B GNo ratings yet
- Letter On Hazard Pay PDFDocument2 pagesLetter On Hazard Pay PDFAravella SimotasNo ratings yet
- 1 Welch Practices A Hard Nosed Management Style How Can SuchDocument2 pages1 Welch Practices A Hard Nosed Management Style How Can SuchAmit PandeyNo ratings yet
- MULTIPLE CHOICE. Choose The One Alternative That Best Completes The Statement or Answers TheDocument20 pagesMULTIPLE CHOICE. Choose The One Alternative That Best Completes The Statement or Answers TheJasmeet KaurNo ratings yet
- Case 5 - Wendell Unity Products CompanyDocument2 pagesCase 5 - Wendell Unity Products CompanyNeily Gwenne ChavezNo ratings yet
- Viva - PHI 401Document5 pagesViva - PHI 401Fariha FarjanaNo ratings yet