You might also like
- Understanding Risk Bat Coronavirus Emergence Grant NoticeDocument528 pagesUnderstanding Risk Bat Coronavirus Emergence Grant NoticeNew York Post100% (6)
- BeeKeeping For Profit Business Plan SpreadsheetDocument18 pagesBeeKeeping For Profit Business Plan SpreadsheetAllan Z McMakenNo ratings yet
- Experience Certificate Format Letter PDFDocument2 pagesExperience Certificate Format Letter PDFDenise0% (2)
- Administrative Healthcare Data: A Guide to Its Origin, Content, and Application Using SASFrom EverandAdministrative Healthcare Data: A Guide to Its Origin, Content, and Application Using SASRating: 4.5 out of 5 stars4.5/5 (2)
- Axa Claim FormDocument2 pagesAxa Claim FormReem Mohamed El BarraniNo ratings yet
- Erection Testing and Commissioning of Transmission Lines & Sub-StationDocument19 pagesErection Testing and Commissioning of Transmission Lines & Sub-Stationarun kumarNo ratings yet
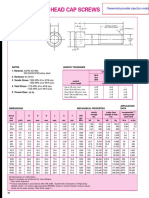
- Metric Socket Head Cap ScrewsDocument2 pagesMetric Socket Head Cap ScrewsImam MulyonoNo ratings yet
- Whats Really Important When Youre Designing The Low Voltage SwitchgearDocument5 pagesWhats Really Important When Youre Designing The Low Voltage SwitchgearsulphurdioxideNo ratings yet
- Authentication Application Form 2017 WhiteBGDocument1 pageAuthentication Application Form 2017 WhiteBGYasuhiro KeiNo ratings yet
- Bosch Pack 101 Wrapper enDocument2 pagesBosch Pack 101 Wrapper enHaider AliNo ratings yet
- AXA Reimbursement Form ALL enDocument2 pagesAXA Reimbursement Form ALL enReynard Delos SantosNo ratings yet
- NHC-06-11-2023 - Server Upgrade, Virtualisation and MigrationDocument60 pagesNHC-06-11-2023 - Server Upgrade, Virtualisation and Migrationjuniordiago837No ratings yet
- Educational-Grant-Application US V 1-0Document5 pagesEducational-Grant-Application US V 1-0Okiki Jesu Ajasa BranchNo ratings yet
- Greatwestlife Claim FormDocument2 pagesGreatwestlife Claim Formhome2022novNo ratings yet
- HRD C1 001 017 R00 Applicant Screening Form (Staffs)Document2 pagesHRD C1 001 017 R00 Applicant Screening Form (Staffs)radha jayaramanNo ratings yet
- Caribbean Examinations Council: Application For Replacement Certificate or Diploma Declaration of LossDocument2 pagesCaribbean Examinations Council: Application For Replacement Certificate or Diploma Declaration of LossMandy ThomasNo ratings yet
- CHECK LIST Mandatory Documents To Be Submitted Along With The Application Form 2-2-24Document9 pagesCHECK LIST Mandatory Documents To Be Submitted Along With The Application Form 2-2-24Street TalentNo ratings yet
- Securian Hospital Indemnity Claim Form - Pre-ExDocument8 pagesSecurian Hospital Indemnity Claim Form - Pre-Exvkpf2tfymmNo ratings yet
- NB 21 Post Nomination RequestsDocument2 pagesNB 21 Post Nomination Requestssudarshansunar96No ratings yet
- 2016 17 EDITABLE Matched Funding Grant Application FormDocument6 pages2016 17 EDITABLE Matched Funding Grant Application FormeddyNo ratings yet
- PHMN2983759454584 1Document5 pagesPHMN2983759454584 1aeronjhricksen1029No ratings yet
- Authorization Form For Oxygen Equipment and Supplies: Section 1 - Plan Member InformationDocument1 pageAuthorization Form For Oxygen Equipment and Supplies: Section 1 - Plan Member Informationmichel_adam1701No ratings yet
- Check List For Hard Copy of Documents To Be Submitted To NTS For Mora 31-1-24Document9 pagesCheck List For Hard Copy of Documents To Be Submitted To NTS For Mora 31-1-24uneed0% (1)
- Hnca Physician Network Participation Request Form PDFDocument1 pageHnca Physician Network Participation Request Form PDFMalsom SingsonNo ratings yet
- 2010 Claim FormDocument2 pages2010 Claim FormChris GreenmanNo ratings yet
- SGP Generic Claim FormDocument5 pagesSGP Generic Claim FormSanny HamdaniNo ratings yet
- Checklist of Requirements For SRRV Application PDF EDITABLEDocument1 pageChecklist of Requirements For SRRV Application PDF EDITABLEОлег ТимченкоNo ratings yet
- Deers Enrollment PDFDocument8 pagesDeers Enrollment PDFlzeron75No ratings yet
- Claim Form For Out of Canada H.S.M. Expense Benefit: Section 1 - Must Be Completed by The Provider of ServiceDocument1 pageClaim Form For Out of Canada H.S.M. Expense Benefit: Section 1 - Must Be Completed by The Provider of Servicemichel_adam1701No ratings yet
- Moratorium Exemption Request FormDocument3 pagesMoratorium Exemption Request FormEsra KhaleelNo ratings yet
- Form ADocument5 pagesForm AShema MayanjaNo ratings yet
- AXA Reimbursement Claim FormDocument2 pagesAXA Reimbursement Claim Formrajkamal eshwarNo ratings yet
- General Claim Submission Form: Section 1 - Plan Member InformationDocument2 pagesGeneral Claim Submission Form: Section 1 - Plan Member Informationmichel_adam1701No ratings yet
- Guidelines For Shariah Advisers - Appendix 2 - (Clean)Document7 pagesGuidelines For Shariah Advisers - Appendix 2 - (Clean)Ahmad SyafeeqNo ratings yet
- O P C A: Regon Ractitioner Redentialing PplicationDocument14 pagesO P C A: Regon Ractitioner Redentialing PplicationReyn JohnsonNo ratings yet
- Form Medical ReimbursmentDocument1 pageForm Medical ReimbursmentMayani ElizaNo ratings yet
- CADTH Advance Notification FormDocument8 pagesCADTH Advance Notification FormdawnNo ratings yet
- Test AxaDocument2 pagesTest AxaElmedina Berin HalilovićNo ratings yet
- Inbound 2401892485776729288Document3 pagesInbound 2401892485776729288Elrym BanuaNo ratings yet
- Energy Savings Assistance Program Categorical Eligibility GuideDocument2 pagesEnergy Savings Assistance Program Categorical Eligibility GuidedomermaNo ratings yet
- Vendor Submittal Checklist - MOI ProjectDocument12 pagesVendor Submittal Checklist - MOI ProjectIssam SalehNo ratings yet
- Agro Grant From USADF & NassikannoDocument8 pagesAgro Grant From USADF & NassikannoMuhammad Bara'u SuleimanNo ratings yet
- DM Submission of List of Stakeholder PartnersDocument4 pagesDM Submission of List of Stakeholder PartnersLearsi AfableNo ratings yet
- New VerifyDocument1 pageNew VerifyMelissa MNo ratings yet
- Group: Application Checklist For Maryland Medical Assistance Program Application GroupDocument21 pagesGroup: Application Checklist For Maryland Medical Assistance Program Application GroupkwonjuNo ratings yet
- Healthcare Spending Account Claim Form: Member InformationDocument2 pagesHealthcare Spending Account Claim Form: Member InformationANGEL DELOSSANTOSNo ratings yet
- Axa Reimbursement Claim Form 01Document2 pagesAxa Reimbursement Claim Form 01Tarak FakhfakhNo ratings yet
- Revised - Med Assistance Form - With CNDocument3 pagesRevised - Med Assistance Form - With CNchristine vizcondeNo ratings yet
- Loan Application FormDocument2 pagesLoan Application Formal lakwenaNo ratings yet
- Relocation MH Verification Form - 8.21Document1 pageRelocation MH Verification Form - 8.21jayteebasiNo ratings yet
- National Health Service Corps Application - Loan Repayment Program - HHS HRSA NHSC LRPDocument17 pagesNational Health Service Corps Application - Loan Repayment Program - HHS HRSA NHSC LRPAccessible Journal Media: Peace Corps DocumentsNo ratings yet
- VA 10-0361D Per Diem Form FillableDocument1 pageVA 10-0361D Per Diem Form FillableJames FreyNo ratings yet
- CMRL.12.18 : Section A: New Business, Regulatory and Sales-Related RequirementsDocument2 pagesCMRL.12.18 : Section A: New Business, Regulatory and Sales-Related RequirementsJovelyn ArgeteNo ratings yet
- Short Application For Eligibility EnglishDocument18 pagesShort Application For Eligibility EnglishdukegarrikNo ratings yet
- ADR Letter Sample - Part - A - InitialDocument5 pagesADR Letter Sample - Part - A - InitialAiEnmaNo ratings yet
- 'NEXtCARE UAE - ASOAP FormDocument1 page'NEXtCARE UAE - ASOAP FormMohyee Eldin RagebNo ratings yet
- Fort Lyon Referral Application - 2021Document13 pagesFort Lyon Referral Application - 2021carrerasjaxxxNo ratings yet
- 2021 Standards For Medical TransportationDocument6 pages2021 Standards For Medical TransportationThu Hien PHAMNo ratings yet
- TN - Enrollment Document For SCWI0 - Created 6 12 2023 - 37734108Document4 pagesTN - Enrollment Document For SCWI0 - Created 6 12 2023 - 37734108kalinalveyNo ratings yet
- Claim Health Care Benefits 19132ADocument2 pagesClaim Health Care Benefits 19132ACharles MoncyNo ratings yet
- Empanelment Form 2020 UpdateDocument35 pagesEmpanelment Form 2020 UpdateasminrajeNo ratings yet
- Application 2 PDFDocument15 pagesApplication 2 PDFMary SoteloNo ratings yet
- Molina FormDocument2 pagesMolina FormscorreaNo ratings yet
- Supporting Information For The CRCB Application: IdentificationDocument2 pagesSupporting Information For The CRCB Application: IdentificationEWO ATTNo ratings yet
- 62 Sundance Pollen TrapDocument7 pages62 Sundance Pollen TrapAllan Z McMakenNo ratings yet
- T-Shirt and Hat Order FormDocument1 pageT-Shirt and Hat Order FormAllan Z McMakenNo ratings yet
- Hive Record 01 PDFDocument1 pageHive Record 01 PDFAllan Z McMakenNo ratings yet
- ABJ March 1996A Different Twist On Swarm Prevention Part 1 of Two PartsDocument2 pagesABJ March 1996A Different Twist On Swarm Prevention Part 1 of Two PartsAllan Z McMakenNo ratings yet
- Summer Fall Chapter 9Document34 pagesSummer Fall Chapter 9Allan Z McMakenNo ratings yet
- Dummy PDFDocument1 pageDummy PDFAllan Z McMakenNo ratings yet
- Nolimitdrones Overview: Your Drone. This All Changes With NLDDocument20 pagesNolimitdrones Overview: Your Drone. This All Changes With NLDAllan Z McMakenNo ratings yet
- Abuse PDFDocument3 pagesAbuse PDFAllan Z McMakenNo ratings yet
- f1040 2000 PDFDocument2 pagesf1040 2000 PDFAllan Z McMakenNo ratings yet
- LinuslucyDocument6 pagesLinuslucyAllan Z McMaken100% (4)
- Constitution of IndiaDocument44 pagesConstitution of Indiasoumya612No ratings yet
- United States of America v. One Parcel of Real Property and Improvements, Located at 1100 Peeler Avenue, Lakeland, Lanier County, Georgia - Document No. 5Document3 pagesUnited States of America v. One Parcel of Real Property and Improvements, Located at 1100 Peeler Avenue, Lakeland, Lanier County, Georgia - Document No. 5Justia.comNo ratings yet
- Ligia Dorina CREMENE: Associate ProfessorDocument3 pagesLigia Dorina CREMENE: Associate ProfessorEmoke SzekelyNo ratings yet
- Key Success Factors of SME Entrepreneurs: Empirical Study in VietnamDocument8 pagesKey Success Factors of SME Entrepreneurs: Empirical Study in VietnamRekhsa AngkasawanNo ratings yet
- Converting V7 Filesto V8 MR3 in Micro StationDocument8 pagesConverting V7 Filesto V8 MR3 in Micro StationerikestrelaNo ratings yet
- Business Environment-HA 1Document2 pagesBusiness Environment-HA 1SrinivasNo ratings yet
- Reynold Fredrik Tallo Bato Godo - Jurnal Fakultas HukumDocument17 pagesReynold Fredrik Tallo Bato Godo - Jurnal Fakultas HukumMarcelino JacobNo ratings yet
- COST: It May Be Defined As The Monetary Value of All Sacrifices Made To Achieve An Objective (I.e. To Produce Goods and Services)Document18 pagesCOST: It May Be Defined As The Monetary Value of All Sacrifices Made To Achieve An Objective (I.e. To Produce Goods and Services)अक्षय शर्माNo ratings yet
- Free Holland Code Assessment ReportDocument13 pagesFree Holland Code Assessment ReportfisheriesNo ratings yet
- 3 Collaborate - Workshop Slides L7Document19 pages3 Collaborate - Workshop Slides L7Jackal ChauNo ratings yet
- Possible Implementation of Feasible Project Structure For LNG Distribution of Eastern IndonesiaDocument127 pagesPossible Implementation of Feasible Project Structure For LNG Distribution of Eastern IndonesiaCicakHey2No ratings yet
- Specification For Installation of Underground Conduit SystemsDocument60 pagesSpecification For Installation of Underground Conduit SystemsMarkusMakuAldoNo ratings yet
- Legal Writing Reviewer Atty Arnold Cacho PDFDocument11 pagesLegal Writing Reviewer Atty Arnold Cacho PDFPaul ValerosNo ratings yet
- 7ano InglêsDocument116 pages7ano InglêsAnonymous ywG0ZNR9FNo ratings yet
- 11 Kriteria PenerimaanDocument33 pages11 Kriteria PenerimaanMohd Zulhairi Mohd NoorNo ratings yet
- My RTL Is An AlienDocument14 pagesMy RTL Is An AlienStudentNo ratings yet
- Kami Export - Online Classes Give Positive or Negative Impacts On Academic PerformanceDocument9 pagesKami Export - Online Classes Give Positive or Negative Impacts On Academic PerformanceTheresa MarionNo ratings yet
- Testing Ingine KaliDocument30 pagesTesting Ingine KaliIngiaNo ratings yet
- Tpa PPTX Weebly Assessment and Reporting CropDocument13 pagesTpa PPTX Weebly Assessment and Reporting Cropapi-532162660No ratings yet
- Anonymous Complaint Says Officer Selling GunsDocument5 pagesAnonymous Complaint Says Officer Selling GunsLas Vegas Review-JournalNo ratings yet
- EMC Part 1a PDFDocument3 pagesEMC Part 1a PDFAlexander OngNo ratings yet
- Measuring National IncomeDocument26 pagesMeasuring National IncomeSaidur Rahman Sid100% (1)
- University of San AgustinDocument4 pagesUniversity of San AgustinMark PerryNo ratings yet
- ADs SBs StatusDocument22 pagesADs SBs StatusMelck O'brianNo ratings yet
- Application Form Vaanavil Super Star 2013 NewDocument3 pagesApplication Form Vaanavil Super Star 2013 NewParthiban MuthiahNo ratings yet