You might also like
- Revised Chapter 2Document25 pagesRevised Chapter 2Jahn Ross SabioNo ratings yet
- Water Quality Study: Democratic Republic of Timor-Leste Ministry of Health Environmental Health DivisionDocument29 pagesWater Quality Study: Democratic Republic of Timor-Leste Ministry of Health Environmental Health DivisionAkhil DattaNo ratings yet
- Water-Distribution-Report - PDF NovoDocument36 pagesWater-Distribution-Report - PDF NovoRhamadanny OmarNo ratings yet
- Water - Canada Legal - HPCDocument21 pagesWater - Canada Legal - HPCiguacu.qadNo ratings yet
- PDF Clean WaterDocument24 pagesPDF Clean WaterAishwaryaNo ratings yet
- Assessment of Hygiene Promotion in Madagascar - 2009Document66 pagesAssessment of Hygiene Promotion in Madagascar - 2009HayZara MadagascarNo ratings yet
- What Do The Numbers MeanDocument74 pagesWhat Do The Numbers MeanJoeNo ratings yet
- Guidelines For Canadian Drinking Water Quality Summary TableDocument26 pagesGuidelines For Canadian Drinking Water Quality Summary Tablehoussem houssemNo ratings yet
- Mainstreaming Water Safety Plans in ADB Water Sector Projects: Lessons and ChallengesFrom EverandMainstreaming Water Safety Plans in ADB Water Sector Projects: Lessons and ChallengesNo ratings yet
- WQMS Framework PDFDocument148 pagesWQMS Framework PDFSanchit khandelwalNo ratings yet
- Drinking Water Quality Monitoring & Surveillance FrameworkDocument148 pagesDrinking Water Quality Monitoring & Surveillance FrameworkCatarina MarquesNo ratings yet
- International Standards of Drinking WaterDocument148 pagesInternational Standards of Drinking Watere_afshahNo ratings yet
- 2019 Analysis of State Drinking Water Programs Resources and NeedsDocument66 pages2019 Analysis of State Drinking Water Programs Resources and NeedsNick SchwellenbachNo ratings yet
- Surveillance Strategies for Small Community Water SuppliesDocument16 pagesSurveillance Strategies for Small Community Water SuppliesSonish KhatriNo ratings yet
- Improving Water, Sanitation, and Hygiene in Schools: A Guide for Practitioners and Policy Makers in MongoliaFrom EverandImproving Water, Sanitation, and Hygiene in Schools: A Guide for Practitioners and Policy Makers in MongoliaNo ratings yet
- LE 01 - (1958) WHO - International Standards For Drinking-WaterDocument148 pagesLE 01 - (1958) WHO - International Standards For Drinking-WateryuliaNo ratings yet
- Surface Water Treatment Operator Certification ManualDocument309 pagesSurface Water Treatment Operator Certification ManualAshok Thakkar100% (1)
- Ere g14 FinalDocument30 pagesEre g14 FinalShivam YadavNo ratings yet
- Surveillance of Drinking Water Quality Worldwide: Scoping Review ProtocolDocument9 pagesSurveillance of Drinking Water Quality Worldwide: Scoping Review ProtocolKaniya IinNo ratings yet
- UniformDrinkingWaterQualityMonitoringProtocol PDFDocument70 pagesUniformDrinkingWaterQualityMonitoringProtocol PDFvikas2504No ratings yet
- SSRN Id4029784Document13 pagesSSRN Id4029784bryan cudalNo ratings yet
- WSH02 08Document44 pagesWSH02 08RoNo ratings yet
- UUBG Water Ver4Document31 pagesUUBG Water Ver4mihirhpatelNo ratings yet
- Water Quality USGSDocument23 pagesWater Quality USGScris.mendez.1993No ratings yet
- Guidelines for Drinking Water Safety Planning for West BengalFrom EverandGuidelines for Drinking Water Safety Planning for West BengalNo ratings yet
- Dc2018-0125-WSP Review and ApprovalDocument26 pagesDc2018-0125-WSP Review and ApprovalBoni MagtibayNo ratings yet
- 1999 Review of Phosphorous Control Measures in The United States and Their Effects On Water QualityDocument43 pages1999 Review of Phosphorous Control Measures in The United States and Their Effects On Water QualityFábio Paiva da SilvaNo ratings yet
- P2ad Water Efficiency Manual PDFDocument129 pagesP2ad Water Efficiency Manual PDFRenato RodriguezNo ratings yet
- Ensuring access to quality water servicesDocument36 pagesEnsuring access to quality water servicesAnnNo ratings yet
- Tank Report July 12 2011 PDFDocument152 pagesTank Report July 12 2011 PDFAveksaNo ratings yet
- Sonabel CHD2 LDWQMCDocument63 pagesSonabel CHD2 LDWQMCeoh.cvchdNo ratings yet
- Aquatabs Technical Report.2012Document48 pagesAquatabs Technical Report.2012Carlos Alberto Rivera RuizNo ratings yet
- PGD Researchfor Strategia NatherlandsDocument85 pagesPGD Researchfor Strategia NatherlandsManon DavidNo ratings yet
- 5 AbsDocument11 pages5 AbsAngelica PostreNo ratings yet
- CDC Survey PresentationDocument38 pagesCDC Survey PresentationHNNNo ratings yet
- WHO Guidelines for drinking water quality and standards (38 charactersDocument3 pagesWHO Guidelines for drinking water quality and standards (38 charactersSameer ArifNo ratings yet
- HACCP WATER FinalDocument68 pagesHACCP WATER FinalClifton JuraNo ratings yet
- Assessing Drinking Water QualityDocument12 pagesAssessing Drinking Water QualitykawterNo ratings yet
- Benjamin Dissertation 2-2-22 CommentsDocument29 pagesBenjamin Dissertation 2-2-22 Commentsbusinge benjaminNo ratings yet
- Lessons Learned FinalDocument81 pagesLessons Learned FinalNiladri ChakrabortiNo ratings yet
- DWSAC Paper 2 2018Document28 pagesDWSAC Paper 2 2018asdasd1414196No ratings yet
- Guidelines For The Use of Stainless Steel in The Water and Desalination IndustriesDocument213 pagesGuidelines For The Use of Stainless Steel in The Water and Desalination IndustriesMunir AbdullahNo ratings yet
- Chapter 3Document108 pagesChapter 3Jerrie Mae MenciasNo ratings yet
- MemoDocument3 pagesMemoapi-620070131No ratings yet
- Planning for Water Conservation in the GVRDDocument109 pagesPlanning for Water Conservation in the GVRD21131A04J2 NUTULAPATI NAGA SRIPADA VALLABHA ABHIRAMNo ratings yet
- UWSRA tr37 PDFDocument68 pagesUWSRA tr37 PDFdsgthfjNo ratings yet
- 1115 Ijac 02Document15 pages1115 Ijac 02cherryNo ratings yet
- Biofiltration For Advanced Treatment of WastewaterDocument53 pagesBiofiltration For Advanced Treatment of WastewaterdedisumarnoNo ratings yet
- WHO International Standards For Drinking Water PDFDocument204 pagesWHO International Standards For Drinking Water PDFAnonymous G6ceYCzwt100% (1)
- Everything you need to know about drinking waterDocument36 pagesEverything you need to know about drinking waterMatt OverbyNo ratings yet
- Willingness To Pay For Cleaner Water in Less Developed CountriesDocument8 pagesWillingness To Pay For Cleaner Water in Less Developed CountriesPuyanfard PmtNo ratings yet
- Data Analysis and Interpretation: 5.2.1 Evaluation of Water-Supply SystemsDocument11 pagesData Analysis and Interpretation: 5.2.1 Evaluation of Water-Supply SystemsVignesh DuraiNo ratings yet
- Ambient Water Quality Criteria For BacteriaDocument42 pagesAmbient Water Quality Criteria For Bacteriarenshi123No ratings yet
- In Situ Strategies Legislative ReportDocument18 pagesIn Situ Strategies Legislative ReportJane PorterNo ratings yet
- Waterproof 3: Full ReportDocument89 pagesWaterproof 3: Full ReportwinnipegsunNo ratings yet
- Thesis On Drinking Water AnalysisDocument7 pagesThesis On Drinking Water Analysisafloihzesdawig100% (2)
- Water Quality Index For Measuring Drinking Water Quality in Rural Bangladesh: A Cross-Sectional StudyDocument12 pagesWater Quality Index For Measuring Drinking Water Quality in Rural Bangladesh: A Cross-Sectional StudyMd.Sakil AhmedNo ratings yet
- Water For HealthDocument6 pagesWater For HealthKeren ZelcNo ratings yet
- Managing Water Resources for Sustainable Socioeconomic Development: A Country Water Assessment for the People’s Republic of ChinaFrom EverandManaging Water Resources for Sustainable Socioeconomic Development: A Country Water Assessment for the People’s Republic of ChinaNo ratings yet
- Quantifying Water and Energy Linkages in Irrigation: Experiences from Viet NamFrom EverandQuantifying Water and Energy Linkages in Irrigation: Experiences from Viet NamNo ratings yet
- Plot Diagram QuizDocument1 pagePlot Diagram QuizKim Alvic Bantilan SaldoNo ratings yet
- Cidam EappDocument2 pagesCidam EappJoice Dela CruzNo ratings yet
- English TG SHS v.1Document207 pagesEnglish TG SHS v.1Rhea O. Marimla100% (2)
- Verbs in The Present and Past TenseDocument13 pagesVerbs in The Present and Past TenseKim Alvic Bantilan SaldoNo ratings yet
- A Lesson Plan in Imagery 2Document3 pagesA Lesson Plan in Imagery 2HappyNeversmiles100% (3)
- Literary Essay RubricDocument1 pageLiterary Essay RubricKim Alvic Bantilan SaldoNo ratings yet
- Justin's BreakawayDocument4 pagesJustin's BreakawayKim Alvic Bantilan SaldoNo ratings yet
- 20 - The Different Types of Speeches Sept 2012Document3 pages20 - The Different Types of Speeches Sept 2012Chris LamochaNo ratings yet
- Grading Rubric for Short StoriesDocument2 pagesGrading Rubric for Short StoriesKim Alvic Bantilan SaldoNo ratings yet
- Lesson Plans - 12 - SI - ELA - ParallellStructureDocument3 pagesLesson Plans - 12 - SI - ELA - ParallellStructureKim Alvic Bantilan SaldoNo ratings yet
- 1.12 Student SheetDocument1 page1.12 Student SheetKim Alvic Bantilan SaldoNo ratings yet
- Useful Links:: Published First-Hand Accounts, or StoriesDocument2 pagesUseful Links:: Published First-Hand Accounts, or StoriesKim Alvic Bantilan SaldoNo ratings yet
- Understanding Academic Language in Your Discipline AreaDocument14 pagesUnderstanding Academic Language in Your Discipline AreaKim Alvic Bantilan SaldoNo ratings yet
- Verbal & Nonverbal CommunicationDocument41 pagesVerbal & Nonverbal CommunicationKim Alvic Bantilan SaldoNo ratings yet
- CH 7Document33 pagesCH 7Nestor Ricardo Chigne TrellesNo ratings yet
- Editorial PDFDocument2 pagesEditorial PDFCARMINA C. DAGUIONo ratings yet
- Lesson Plan On Report Writing 3 of 4 PDFDocument3 pagesLesson Plan On Report Writing 3 of 4 PDFKim Alvic Bantilan SaldoNo ratings yet
- How To Write Survey Report 2010Document2 pagesHow To Write Survey Report 2010Elissa AmbrosieNo ratings yet
- Lista de Palabras en Ingles PDFDocument2 pagesLista de Palabras en Ingles PDFHugo DominguezNo ratings yet
- From The Nobel Prize Speech by William FaulknerDocument1 pageFrom The Nobel Prize Speech by William FaulknerKim Alvic Bantilan SaldoNo ratings yet
- Teaching Guide SHS Oral CommunicationDocument8 pagesTeaching Guide SHS Oral CommunicationKim Alvic Bantilan SaldoNo ratings yet
- Noun Practice PagesDocument6 pagesNoun Practice PagesMaggie Plby100% (1)
- CSER Howto Use Word-Citations-Bibliography-ToolDocument38 pagesCSER Howto Use Word-Citations-Bibliography-Toolfaheem2005rajaNo ratings yet
- Lesson Plans - 12 - SI - ELA - ParallellStructureDocument3 pagesLesson Plans - 12 - SI - ELA - ParallellStructureKim Alvic Bantilan SaldoNo ratings yet
- Krista Nielsen West Clinton ElementaryDocument29 pagesKrista Nielsen West Clinton ElementaryKim Alvic Bantilan Saldo100% (1)
- Learn 6 Tenses with Verb PartsDocument29 pagesLearn 6 Tenses with Verb PartsKim Alvic Bantilan SaldoNo ratings yet
- Quant METHODSDocument18 pagesQuant METHODSAlexanderGonzalvoNo ratings yet
- English CG Grade 1-10 01.30.2014Document171 pagesEnglish CG Grade 1-10 01.30.2014Ken Hijastro100% (1)
- ERInt IMPACT OF COASTAL CLEAN UP TO BENEFICIARIES PDFDocument6 pagesERInt IMPACT OF COASTAL CLEAN UP TO BENEFICIARIES PDFKim Alvic Bantilan SaldoNo ratings yet
- AquaCulture Application Process and Product ChartDocument1 pageAquaCulture Application Process and Product ChartBhavya MewadaNo ratings yet
- Design of Each Process of ETPDocument9 pagesDesign of Each Process of ETPFaisal Sr. ExecutiveNo ratings yet
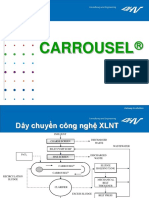
- CARROUSEL Introduction - enDocument49 pagesCARROUSEL Introduction - enKhang TrầnNo ratings yet
- Downloaded From Manuals Search EngineDocument36 pagesDownloaded From Manuals Search EngineJavier braganzaNo ratings yet
- Techno-Commercial Offer For 150 KLD STP, Based Upon MBBR.Document9 pagesTechno-Commercial Offer For 150 KLD STP, Based Upon MBBR.Anshika RaiNo ratings yet
- PF - Passavant Revolving Chain Screen Kur-CDocument2 pagesPF - Passavant Revolving Chain Screen Kur-Cmohamed100% (1)
- Domestic Wastewater TreatmentDocument20 pagesDomestic Wastewater TreatmentShayan SohailNo ratings yet
- Assignment-I (Syllabus Up To Mid-I)Document5 pagesAssignment-I (Syllabus Up To Mid-I)Nitish KumarNo ratings yet
- 28dye Removal by Adsorption A Review 2155 6199 1000371Document5 pages28dye Removal by Adsorption A Review 2155 6199 1000371niloofarNo ratings yet
- Annex 3: WHO Good Manufacturing Practices: Water For Pharmaceutical UseDocument19 pagesAnnex 3: WHO Good Manufacturing Practices: Water For Pharmaceutical UsedesignselvaNo ratings yet
- Packaged STPDocument25 pagesPackaged STPFarooqNo ratings yet
- Activated Sludge MathDocument21 pagesActivated Sludge Mathmohamedbadawy100% (1)
- Manila Water Company Water Safety Plan OverviewDocument154 pagesManila Water Company Water Safety Plan OverviewErwin JasarenoNo ratings yet
- ReNEW Series Fact SheetDocument4 pagesReNEW Series Fact Sheetjpsingh75No ratings yet
- Groundwater Treatment Technology, Third Edition (2009) PDFDocument431 pagesGroundwater Treatment Technology, Third Edition (2009) PDFnoel montanaNo ratings yet
- 1.wastewater Technology SBRDocument12 pages1.wastewater Technology SBRapi-19791607100% (2)
- Literature Review On Wastewater TreatmentDocument8 pagesLiterature Review On Wastewater Treatmentfvg93a8v100% (1)
- TCXDVN 33-2006 Design Standard Water Supply-External Networks and FacilitiesDocument171 pagesTCXDVN 33-2006 Design Standard Water Supply-External Networks and FacilitiesHoward to0% (1)
- Chapt14 - On Site SanitationDocument20 pagesChapt14 - On Site SanitationRyeanKRumano100% (1)
- Industrial Ro Plant 1000 LPH PDFDocument7 pagesIndustrial Ro Plant 1000 LPH PDFPurshottam AmreliyaNo ratings yet
- TILLEY Et Al 2014 S-11 Anaerobic FilterDocument2 pagesTILLEY Et Al 2014 S-11 Anaerobic FilterAshish GargNo ratings yet
- PF - PASSAVANT Bar Screen With Grab Cleaner SGRDocument2 pagesPF - PASSAVANT Bar Screen With Grab Cleaner SGRmohamedNo ratings yet
- Sewerage System PDFDocument2 pagesSewerage System PDFJatteah Suib CalulongNo ratings yet
- Sanitation System DrawingDocument5 pagesSanitation System DrawingFT Daniel SetiawanNo ratings yet
- Wastewater Story QsDocument6 pagesWastewater Story QsTUSHAR DASHNo ratings yet
- Manual: For Tublar BoilerDocument99 pagesManual: For Tublar BoileryahiateneNo ratings yet
- Group 4 - ManuscriptDocument28 pagesGroup 4 - ManuscriptKathleen Kaye CastilloNo ratings yet
- Innovative Water & Waste Water Treatment Solutions ProviderDocument16 pagesInnovative Water & Waste Water Treatment Solutions ProviderA3S ENVIRONo ratings yet
- Al Ansab STP boosts Muscat's wastewater treatmentDocument38 pagesAl Ansab STP boosts Muscat's wastewater treatmentDel MoralesNo ratings yet
- Efficient Water Utilisation in Textile Wet ProcessingDocument4 pagesEfficient Water Utilisation in Textile Wet ProcessingGarmentLearnerNo ratings yet