You might also like
- Cementada Atornillada Rev Sist PDFDocument15 pagesCementada Atornillada Rev Sist PDFjotapintorNo ratings yet
- Manhart 2009Document12 pagesManhart 2009Andrei OanaNo ratings yet
- Clinical Performance of Screw Versus Cement Retained Fixed Implants Supported ReconstructionsDocument15 pagesClinical Performance of Screw Versus Cement Retained Fixed Implants Supported ReconstructionsdanielcetateNo ratings yet
- Is Composite Repair Suitable For Anterior Restorations? A Long-Term Practice-Based Clinical StudyDocument10 pagesIs Composite Repair Suitable For Anterior Restorations? A Long-Term Practice-Based Clinical StudyclaudiaNo ratings yet
- INLAYDocument11 pagesINLAYMira AnggrianiNo ratings yet
- Sadowsky 2007Document9 pagesSadowsky 2007barbara buhlerNo ratings yet
- Da Costa 2013, A Meta Analysis of The Most Indicated Preparation Design For Porcelain Laminate VeneersDocument7 pagesDa Costa 2013, A Meta Analysis of The Most Indicated Preparation Design For Porcelain Laminate VeneersAaron MarroNo ratings yet
- Direct Resin Composite Restorations Versus Indirect Composite Inlays: One-Year ResultsDocument10 pagesDirect Resin Composite Restorations Versus Indirect Composite Inlays: One-Year ResultsHari PriyaNo ratings yet
- Clinical Study and Single-Bottle SystemsDocument7 pagesClinical Study and Single-Bottle SystemsSammer BurgosNo ratings yet
- Effect of Adaptation Time On The Occlusal Force at Denture Dislodgement With or Without AdhesiveDocument6 pagesEffect of Adaptation Time On The Occlusal Force at Denture Dislodgement With or Without AdhesivedentureNo ratings yet
- Selection of Dental Materials and Longevity of Replaced Restorations in Public Dental Health Clinics in Northern SwedenDocument6 pagesSelection of Dental Materials and Longevity of Replaced Restorations in Public Dental Health Clinics in Northern SwedenClara CarneiroNo ratings yet
- Longevity of Posterior Composite RestoraDocument15 pagesLongevity of Posterior Composite RestoraMelissa SierraNo ratings yet
- Restorations in Primary Teeth: A Systematic Review On Survival and Reasons For FailuresDocument17 pagesRestorations in Primary Teeth: A Systematic Review On Survival and Reasons For FailuresMel LlerenaNo ratings yet
- Relative Share, Frequency and Correlation of Restorations in Both Dental Dentitions in ChildhoodDocument8 pagesRelative Share, Frequency and Correlation of Restorations in Both Dental Dentitions in ChildhoodIJPHSNo ratings yet
- Longevity of Posterior Composite Restorations: Not Only A Matter of MaterialsDocument15 pagesLongevity of Posterior Composite Restorations: Not Only A Matter of MaterialsKalpanaNo ratings yet
- Ferrule PDFDocument7 pagesFerrule PDFVidya SenthuNo ratings yet
- Longevity of Posterior Resin Composite Restorations in Adults - A Systematic ReviewDocument21 pagesLongevity of Posterior Resin Composite Restorations in Adults - A Systematic ReviewCarla FloresNo ratings yet
- Direct Versus Indirect Inlayonlay Composite Restorations in Posterior Teeth. A Systematic Review and Meta-Analysis PDFDocument10 pagesDirect Versus Indirect Inlayonlay Composite Restorations in Posterior Teeth. A Systematic Review and Meta-Analysis PDFMel LlerenaNo ratings yet
- 18-Year Survival of Posterior Composite Resin Restorations With and Without Glass Ionomer Cement As BaseDocument7 pages18-Year Survival of Posterior Composite Resin Restorations With and Without Glass Ionomer Cement As BaseHurianNo ratings yet
- Clinical Performance of Bulk-Fill and Conventional Resin Composite Restorations in Posterior Teeth: A Systematic Review and Meta-AnalysisDocument13 pagesClinical Performance of Bulk-Fill and Conventional Resin Composite Restorations in Posterior Teeth: A Systematic Review and Meta-AnalysisNicolás SotoNo ratings yet
- 18 Co PDFDocument1 page18 Co PDFSaad LiaqatNo ratings yet
- Articulo 8Document10 pagesArticulo 8SofiaNo ratings yet
- Clinical Longevity of Indirect Composite Resin Inlays and Onlays: An Up To 9-Year Prospective StudyDocument7 pagesClinical Longevity of Indirect Composite Resin Inlays and Onlays: An Up To 9-Year Prospective StudyLuciano ESENARRONo ratings yet
- Clinical Effectiveness of Contemporary Adhesives A Systematic Review of Current Clinical Trials 2005Document18 pagesClinical Effectiveness of Contemporary Adhesives A Systematic Review of Current Clinical Trials 2005Mohamed OudaNo ratings yet
- Do Glass Ionomer Cements Prevent Caries On The Margins of Restaurations in Primary TeethDocument9 pagesDo Glass Ionomer Cements Prevent Caries On The Margins of Restaurations in Primary TeethDoruNo ratings yet
- 1 R Cambios OSEOS POSEXTRACCIONDocument16 pages1 R Cambios OSEOS POSEXTRACCIONfeli.riam24No ratings yet
- Medicine, Implantology, Removable Dentures, Technology DepartmentDocument7 pagesMedicine, Implantology, Removable Dentures, Technology DepartmentAnonymous AyxIccS4aXNo ratings yet
- Efficacy of Composite Versus Ceramic Inlays and Onlays: Study Protocol For The CECOIA Randomized Controlled TrialDocument10 pagesEfficacy of Composite Versus Ceramic Inlays and Onlays: Study Protocol For The CECOIA Randomized Controlled TrialMuhammad UlynnuhaNo ratings yet
- Wittneben Jomi 2014 07Document16 pagesWittneben Jomi 2014 07Nomica OdontologiaNo ratings yet
- Ask The Experts: Longevity of Posterior Composite RestorationsDocument3 pagesAsk The Experts: Longevity of Posterior Composite RestorationsAre BovedaNo ratings yet
- Three-Year Clinical Performance of Composite Restorations Placed by Undergraduate Dental StudentsDocument6 pagesThree-Year Clinical Performance of Composite Restorations Placed by Undergraduate Dental StudentsFaiz Ahmad HamzahNo ratings yet
- Healing of Intrabony Defects Following Regenerative SurgeryDocument13 pagesHealing of Intrabony Defects Following Regenerative SurgeryYou're Just As Sane As DivaNo ratings yet
- Dental Sealants Prevent Caries in PracticeDocument9 pagesDental Sealants Prevent Caries in PracticeAura EstradaNo ratings yet
- Clinical Performance of Screw-Versus Cement Retained Fixed Implant-Supported Reconstructions A Systematic ReviewDocument16 pagesClinical Performance of Screw-Versus Cement Retained Fixed Implant-Supported Reconstructions A Systematic ReviewSeptimiu TiplicaNo ratings yet
- Longevity of Posterior Composite RestorationDocument15 pagesLongevity of Posterior Composite Restorationvrana23No ratings yet
- Clinical Evaluation of Fissure Sealant Retention Rates Over 48 MonthsDocument7 pagesClinical Evaluation of Fissure Sealant Retention Rates Over 48 MonthsMaria Ximena Torres PovedaNo ratings yet
- Effect of dentin roughness on the adhesive performance in non cariousDocument10 pagesEffect of dentin roughness on the adhesive performance in non cariouslucasdorna92No ratings yet
- Laske 2016Document6 pagesLaske 2016KaouterNo ratings yet
- 10 3290@j Jad A35008Document13 pages10 3290@j Jad A35008Teresa BeltranNo ratings yet
- Artigo 1Document8 pagesArtigo 1joao pauloNo ratings yet
- Posterior Composite Restoration UpdateDocument10 pagesPosterior Composite Restoration UpdateBianca IovoaiaNo ratings yet
- Influence of Viscosity and Chemical Composition of Composite Resins in Non Carious Cervical Restorations 12 Month Randomized Clinical TrialDocument12 pagesInfluence of Viscosity and Chemical Composition of Composite Resins in Non Carious Cervical Restorations 12 Month Randomized Clinical TrialŞtefania ZalăNo ratings yet
- NANO EN INDIRECTAS - PDFDocument7 pagesNANO EN INDIRECTAS - PDFManuel Roberto Sarmiento LimasNo ratings yet
- Ari 15Document6 pagesAri 15mariaNo ratings yet
- Fixed Partial Dentures in An Up To 8-Year Follow-UpDocument8 pagesFixed Partial Dentures in An Up To 8-Year Follow-Updaniel187951No ratings yet
- Burbridge2007 NoDocument6 pagesBurbridge2007 NoKatherine VilchezNo ratings yet
- Kunz Pvm. 2022.Document17 pagesKunz Pvm. 2022.Nicolás SotoNo ratings yet
- Fiber-Reinforced Fixed Partial Dentures: A Preliminary Retrospective Clinical StudyDocument5 pagesFiber-Reinforced Fixed Partial Dentures: A Preliminary Retrospective Clinical StudyMuchlis Fauzi ENo ratings yet
- Art 1Document38 pagesArt 1Juan José Chacón BalderramaNo ratings yet
- DirectCompositesversusIndirectCompositeInlays One YearResultsDocument11 pagesDirectCompositesversusIndirectCompositeInlays One YearResultsAya Ibrahim YassinNo ratings yet
- Full Arch Implant Supported Rehabilitations: A Prospective Study Comparing Porcelain Veneered Zirconia Frameworks To Monolithic ZirconiaDocument11 pagesFull Arch Implant Supported Rehabilitations: A Prospective Study Comparing Porcelain Veneered Zirconia Frameworks To Monolithic ZirconiasnkidNo ratings yet
- Skupien 2016Document6 pagesSkupien 2016valperlunNo ratings yet
- Evaluations of Microleakage Around Class I Amalgam and Composite RestorationsDocument8 pagesEvaluations of Microleakage Around Class I Amalgam and Composite RestorationsJAYASOORYAN S P M.D.S. CONSERVATIVE DENTISTRY AND ENDODONTICSNo ratings yet
- Tooth-Implant Connection: A Review: Journal of Oral Implantology November 2010Document8 pagesTooth-Implant Connection: A Review: Journal of Oral Implantology November 2010MohamedFaragNo ratings yet
- Longterm Survey All Ceramic Inlays Onlays Quintessnce 2020Document11 pagesLongterm Survey All Ceramic Inlays Onlays Quintessnce 2020Raghu PratapNo ratings yet
- RostDocument56 pagesRostandi boyNo ratings yet
- 21 CoDocument26 pages21 CoSaad LiaqatNo ratings yet
- Millen2015 Rev SysDocument15 pagesMillen2015 Rev SysHicham AlkhayarNo ratings yet
- Cementation in Dental Implantology: An Evidence-Based GuideFrom EverandCementation in Dental Implantology: An Evidence-Based GuideChandur P.K. WadhwaniNo ratings yet
- Esthetic Oral Rehabilitation with Veneers: A Guide to Treatment Preparation and Clinical ConceptsFrom EverandEsthetic Oral Rehabilitation with Veneers: A Guide to Treatment Preparation and Clinical ConceptsRichard D. TrushkowskyNo ratings yet
- Proper selection of dental cementsDocument6 pagesProper selection of dental cementsNabilah NazalikaNo ratings yet
- RETENTIVE PROPERTIES OF DENTAL CEMENTSDocument9 pagesRETENTIVE PROPERTIES OF DENTAL CEMENTSSaad LiaqatNo ratings yet
- RETENTIVE PROPERTIES OF DENTAL CEMENTSDocument9 pagesRETENTIVE PROPERTIES OF DENTAL CEMENTSSaad LiaqatNo ratings yet
- A Review of Dental Cements: Kipp Wingo, DVM, DAVDCDocument10 pagesA Review of Dental Cements: Kipp Wingo, DVM, DAVDCSaad LiaqatNo ratings yet
- Characterization and Analyses of Acid-Extractable and Leached Trace Elements in Dental CementsDocument7 pagesCharacterization and Analyses of Acid-Extractable and Leached Trace Elements in Dental CementsSaad LiaqatNo ratings yet
- A Review of Conventional and Contemporary Luting Agents Used in DentistryDocument8 pagesA Review of Conventional and Contemporary Luting Agents Used in DentistryAnand KasiNo ratings yet
- 1 C PDFDocument9 pages1 C PDFSaad LiaqatNo ratings yet
- Maroulakos 2019Document12 pagesMaroulakos 2019Luis Alberto Carpio MorenoNo ratings yet
- 4 BaDocument18 pages4 BaSaad LiaqatNo ratings yet
- Advances in Dental Research: Review of Dental Impression MaterialsDocument15 pagesAdvances in Dental Research: Review of Dental Impression MaterialsSaad LiaqatNo ratings yet
- Skupien2015 Factores Asociados Con La Retencion Del PosteDocument8 pagesSkupien2015 Factores Asociados Con La Retencion Del PosteAmparo AnayaNo ratings yet
- Surface Characterization of Passive Film On Nicr-Based Dental Casting AlloysDocument8 pagesSurface Characterization of Passive Film On Nicr-Based Dental Casting AlloysSaad LiaqatNo ratings yet
- 8 DC PDFDocument6 pages8 DC PDFSaad LiaqatNo ratings yet
- Casting of Titanium and Ni-Ti Dental Alloys Using a New Vacuum Casting MachineDocument5 pagesCasting of Titanium and Ni-Ti Dental Alloys Using a New Vacuum Casting MachineSaad LiaqatNo ratings yet
- 4 DCDocument13 pages4 DCSaad LiaqatNo ratings yet
- Artifacts From Dental Casting Alloys in Magnetic Resonance ImagingDocument5 pagesArtifacts From Dental Casting Alloys in Magnetic Resonance ImagingSaad LiaqatNo ratings yet
- Biocompatibility of Dental Casting Alloys: A ReviewDocument12 pagesBiocompatibility of Dental Casting Alloys: A ReviewSaad LiaqatNo ratings yet
- 17 Co PDFDocument25 pages17 Co PDFSaad LiaqatNo ratings yet
- The Use of Mercury in Dentistry: A Critical Review of The Recent LiteratureDocument14 pagesThe Use of Mercury in Dentistry: A Critical Review of The Recent LiteratureSaad LiaqatNo ratings yet
- 1 Da PDFDocument8 pages1 Da PDFSaad LiaqatNo ratings yet
- Experimental Microleakage Around Ageing Dental Amalgam Restorations: A ReviewDocument11 pagesExperimental Microleakage Around Ageing Dental Amalgam Restorations: A ReviewSaad LiaqatNo ratings yet
- 6 Da PDFDocument11 pages6 Da PDFSaad LiaqatNo ratings yet
- 19 Co PDFDocument15 pages19 Co PDFSaad LiaqatNo ratings yet
- 3 Da PDFDocument14 pages3 Da PDFSaad LiaqatNo ratings yet
- 21 CoDocument26 pages21 CoSaad LiaqatNo ratings yet
- Bond Strength of Universal Adhesives: A Systematic Review and Meta-AnalysisDocument12 pagesBond Strength of Universal Adhesives: A Systematic Review and Meta-AnalysisPablo BenitezNo ratings yet
- 4 BaDocument18 pages4 BaSaad LiaqatNo ratings yet
- 16 CoDocument9 pages16 CoSaad LiaqatNo ratings yet
- 15 CoDocument9 pages15 CoSaad LiaqatNo ratings yet
- 14 CoDocument9 pages14 CoSaad LiaqatNo ratings yet
- Inlay Retained FPDDocument35 pagesInlay Retained FPDNikita AggarwalNo ratings yet
- Non Vital Pulp TherapyDocument23 pagesNon Vital Pulp TherapyAmit GaurNo ratings yet
- EosDocument33 pagesEosIonut TodericNo ratings yet
- LogbookBDS2 Melangell Corabelle 2206042602Document12 pagesLogbookBDS2 Melangell Corabelle 2206042602Melangell CorabelleNo ratings yet
- Laminates AND Veneers: Dr. Sakshi Rawal Department of Prosthodontics MDS II YearDocument76 pagesLaminates AND Veneers: Dr. Sakshi Rawal Department of Prosthodontics MDS II Yearsapna100% (2)
- Product Catalogue: Global EditionDocument19 pagesProduct Catalogue: Global EditionKhiro DbNo ratings yet
- 3M Single Bond 2 Adhesive (Phần Technique Guides)Document28 pages3M Single Bond 2 Adhesive (Phần Technique Guides)traubo158No ratings yet
- Cure Tooth Decay - Interview TranscriptDocument16 pagesCure Tooth Decay - Interview TranscripteisenreichNo ratings yet
- Biomedical Technology Lecture Notes 2015Document11 pagesBiomedical Technology Lecture Notes 2015Phi NguyenNo ratings yet
- Requirements of Dental Cements For Lining ApplicationsDocument28 pagesRequirements of Dental Cements For Lining ApplicationsShahzadi SamanaNo ratings yet
- Influence of Cervical Margin Relocation CMR On Periodonta - 2018 - Journal ofDocument7 pagesInfluence of Cervical Margin Relocation CMR On Periodonta - 2018 - Journal ofIvy MedNo ratings yet
- HathoDocument48 pagesHathotaitaNo ratings yet
- Direct Coronal restorations of frontal teeth: Stratification technique of veneersDocument18 pagesDirect Coronal restorations of frontal teeth: Stratification technique of veneersbubbiexo100% (1)
- Ceramics As Biomaterials For Dental RestorationDocument17 pagesCeramics As Biomaterials For Dental RestorationCatalina GómezNo ratings yet
- Lecture 2, Dental Amalgam II (Script)Document11 pagesLecture 2, Dental Amalgam II (Script)JustDen09No ratings yet
- 1Document134 pages1ghizlane berradaNo ratings yet
- Crown 2 QB: Put T&F. and Correct The False StatementDocument17 pagesCrown 2 QB: Put T&F. and Correct The False StatementMustafa SaßerNo ratings yet
- All Ceramic Crown: Materials & Fabrication TechniquesDocument13 pagesAll Ceramic Crown: Materials & Fabrication Techniquesbaqer hussainNo ratings yet
- Esthetic Rehabilitation of Anterior Teet PDFDocument8 pagesEsthetic Rehabilitation of Anterior Teet PDFsaulNo ratings yet
- Brilliant Crios: High Performance - Made BrilliantDocument10 pagesBrilliant Crios: High Performance - Made BrilliantmiauNo ratings yet
- 1664796812.190114 OptiBond eXTRa-Universal-Sales-Brochure REV0Document5 pages1664796812.190114 OptiBond eXTRa-Universal-Sales-Brochure REV0Ramy AmirNo ratings yet
- MKT 17 0612 Drcoleman Harmonize Ou EbookDocument7 pagesMKT 17 0612 Drcoleman Harmonize Ou EbookWirya PratamaNo ratings yet
- 1 11 Dent MatDocument33 pages1 11 Dent MatkrstnkyslNo ratings yet
- Dietschi D, Et Al. 2002. Marginal and Internal Adaptation of Class II Restorations After Immediate or Delayed Composite Placement.Document11 pagesDietschi D, Et Al. 2002. Marginal and Internal Adaptation of Class II Restorations After Immediate or Delayed Composite Placement.Ranulfo Castillo PeñaNo ratings yet
- Ebook: Bioactive Dental Materials: The Future Is NowDocument7 pagesEbook: Bioactive Dental Materials: The Future Is NowAli FaridiNo ratings yet
- Kode ICD XDocument764 pagesKode ICD XMade Surya DinathaNo ratings yet
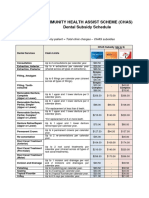
- CHAS Dental Subsidy ScheduleDocument1 pageCHAS Dental Subsidy ScheduleEugeneNo ratings yet
- Oral Galvanism and Electromagnetic FieldsDocument6 pagesOral Galvanism and Electromagnetic FieldsBernarda Mrak100% (1)
- CadcamDocument64 pagesCadcamnandani kumariNo ratings yet
- Selection of Dental Materials and Longevity of Replaced Restorations in Public Dental Health Clinics in Northern SwedenDocument6 pagesSelection of Dental Materials and Longevity of Replaced Restorations in Public Dental Health Clinics in Northern SwedenClara CarneiroNo ratings yet