You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Single Line DiagramDocument1 pageSingle Line DiagramGhanshyam Singh100% (2)
- Quick Zone-Xl User ManualDocument68 pagesQuick Zone-Xl User ManualThan Htike AungNo ratings yet
- 6 Zones Mixer Amplifier With Mp3 TI-1206S/TI-2406S/TI-3506S/TI-5006SDocument3 pages6 Zones Mixer Amplifier With Mp3 TI-1206S/TI-2406S/TI-3506S/TI-5006SThan Htike AungNo ratings yet
- Weatherproof Horn Speaker (7.5W-15W) : FeaturesDocument2 pagesWeatherproof Horn Speaker (7.5W-15W) : FeaturesThan Htike AungNo ratings yet
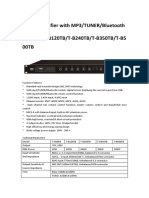
- Mixer Amplifier With MP3/TUNER/Bluetooth T-B60TB/T-B120TB/T-B240TB/T-B350TB/T-B5 00TBDocument2 pagesMixer Amplifier With MP3/TUNER/Bluetooth T-B60TB/T-B120TB/T-B240TB/T-B350TB/T-B5 00TBThan Htike AungNo ratings yet
- 6W Wooden Indoor Wall Mount Speaker: FeaturesDocument3 pages6W Wooden Indoor Wall Mount Speaker: FeaturesThan Htike AungNo ratings yet
- DH-IPC-HFW1220M-S-I2-S2: 2MP HD Network IR Bullet CameraDocument4 pagesDH-IPC-HFW1220M-S-I2-S2: 2MP HD Network IR Bullet CameraThan Htike AungNo ratings yet
- ssd1904 Quickzone Brochure Edition 4 v2 LRDocument8 pagesssd1904 Quickzone Brochure Edition 4 v2 LRThan Htike AungNo ratings yet
- Coaxial Cable Attenuation CalculatorDocument2 pagesCoaxial Cable Attenuation CalculatorThan Htike AungNo ratings yet
- User Manual DTM HD01 BlackDocument10 pagesUser Manual DTM HD01 BlackThan Htike AungNo ratings yet
- Kxns300 User ManualDocument388 pagesKxns300 User ManualTuhuk Ma'aritNo ratings yet
- Dell PowerEdge R820 Spec SheetDocument2 pagesDell PowerEdge R820 Spec SheetThan Htike AungNo ratings yet
- Conventional Smoke DetectorDocument1 pageConventional Smoke DetectorThan Htike AungNo ratings yet
- IPv6 Addressing and Subnetting Workbook - Student VersionDocument166 pagesIPv6 Addressing and Subnetting Workbook - Student VersionThan Htike AungNo ratings yet
- Huawei OptiX OSN 550Document2 pagesHuawei OptiX OSN 550farhanwaliNo ratings yet
- FTTH Magazine PDFDocument7 pagesFTTH Magazine PDFThan Htike AungNo ratings yet
- Guide To SATA Hard Disks Installation and RAID ConfigurationDocument15 pagesGuide To SATA Hard Disks Installation and RAID ConfigurationThan Htike AungNo ratings yet
- Honeywell Aquatrol 2000 PDFDocument60 pagesHoneywell Aquatrol 2000 PDFvsilickasNo ratings yet
- This Tutorial Will Help To Test The Throttle Position Sensor On Your 1989 To 1997 1Document7 pagesThis Tutorial Will Help To Test The Throttle Position Sensor On Your 1989 To 1997 1HERBERT SITORUS100% (1)
- Adaptation Fom Squirrels GamesDocument2 pagesAdaptation Fom Squirrels GamesDenny Boy MochranNo ratings yet
- Save Energy Save EarthDocument2 pagesSave Energy Save EarthMega Ayu100% (2)
- Suplayer Metal Working Sipil and Fabrication: Company ProfileDocument10 pagesSuplayer Metal Working Sipil and Fabrication: Company ProfileRuntian TeaNo ratings yet
- Bảo MậtDocument2 pagesBảo MậtMinh Nghia PhamNo ratings yet
- Oil and Gas Reloaded: Offshore ArgentinaDocument9 pagesOil and Gas Reloaded: Offshore ArgentinaMuhammad Fahmi AnbNo ratings yet
- Crude Palm OilDocument4 pagesCrude Palm OilpalmoilanalyticsNo ratings yet
- Tugas-MPSI-P1-P14 - Kelompok 2 - 19.4A.04Document29 pagesTugas-MPSI-P1-P14 - Kelompok 2 - 19.4A.04gilang putraNo ratings yet
- Information Technology and Telecommunications Services Agreement Between County of San Diego and Enterprise Services, LLC ContraDocument106 pagesInformation Technology and Telecommunications Services Agreement Between County of San Diego and Enterprise Services, LLC ContraJackkk FNo ratings yet
- ChinatownDocument1 pageChinatownAiken KomensenNo ratings yet
- Mortal Kombat XDocument24 pagesMortal Kombat XMindSpaceApocalypseNo ratings yet
- Autodesk Inventor Practice Part DrawingsDocument25 pagesAutodesk Inventor Practice Part DrawingsCiprian Fratila100% (1)
- Train TicketDocument2 pagesTrain TicketGautam KumarNo ratings yet
- White Paper - Data Communication in Substation Automation System SAS - Part 1 Original 23353Document5 pagesWhite Paper - Data Communication in Substation Automation System SAS - Part 1 Original 23353sabrahimaNo ratings yet
- Notes in Judicial AffidavitDocument11 pagesNotes in Judicial AffidavitguibonganNo ratings yet
- Om - 3M CaseDocument18 pagesOm - 3M CaseBianda Puspita Sari100% (1)
- Vbulletin 5 Connect: Quick Start Guide (Ver 1.0)Document21 pagesVbulletin 5 Connect: Quick Start Guide (Ver 1.0)dantevasquezNo ratings yet
- Battlab Report 12 FinalDocument48 pagesBattlab Report 12 FinalLianNo ratings yet
- Spice Board BBLDocument24 pagesSpice Board BBLvenkatpficoNo ratings yet
- Saraswathi 2018Document4 pagesSaraswathi 2018Daniel CoronelNo ratings yet
- No. 3 - Republic vs. DiazDocument7 pagesNo. 3 - Republic vs. DiazMark Gabriel MarangaNo ratings yet
- BS en 12285-1-2003 (2006)Document162 pagesBS en 12285-1-2003 (2006)dahzahNo ratings yet
- Taifun GT User GuideDocument5 pagesTaifun GT User GuidecarloslarumbeNo ratings yet
- Using Excel For Business AnalysisDocument5 pagesUsing Excel For Business Analysis11armiNo ratings yet
- Clark Hess1Document668 pagesClark Hess1Jeyner Chavez VasquezNo ratings yet
- Catalog Electrical Products en - 339 - 1Document20 pagesCatalog Electrical Products en - 339 - 1H 8CNo ratings yet
- HYD CCU: TICKET - ConfirmedDocument2 pagesHYD CCU: TICKET - ConfirmedRahul ValapadasuNo ratings yet
- 150 67-Eg1Document104 pages150 67-Eg1rikoNo ratings yet