Professional Documents
Culture Documents
The Science and Practice of Caries Prevention: Article 1
Uploaded by
Dariana JDOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
The Science and Practice of Caries Prevention: Article 1
Uploaded by
Dariana JDCopyright:
Available Formats
A D
A
J
✷ ✷
N
CON
IO
T
T
A
N
I
U C
IN U
G ED
ARTICLE 1
C O V E R S T O R Y
THE SCIENCE AND PRACTICE
OF CARIES PREVENTION
JOHN D.B. FEATHERSTONE, M.SC., PH.D.
lthough the prevalence of dental
A
A B S T R A C T
Background and Overview. Dental caries in children has declined
caries is a bacterially based disease. When markedly over the last 20 years in
it progresses, acid produced by bacterial
action on dietary fermentable carbohy-
most countries in the Western world,
drates diffuses into the tooth and dis- the disease continues to be a major problem for both adults
solves the carbonated hydroxyapatite min-
and children everywhere.
eral—a process called demineralization.
Pathological factors including acidogenic The trends in caries in U.S. children during the last 30
bacteria (mutans streptococci and lacto-
years were recently summarized1 on the basis of results of
bacilli), salivary dysfunction, and dietary
carbohydrates are related to caries pro- four national surveys.2-5 By the late 1980s, although
gression. Protective factors—which
approximately 75 percent of children aged 5 to 11 years
include salivary calcium, phosphate and
proteins, salivary flow, fluoride in saliva, were caries-free, about 70 percent of the 12- to 17-year-olds
and antibacterial components or agents—
still had caries. Approximately 25 percent of children and
can balance, prevent or reverse dental
caries. adolescents in the 5- to 17-year age range accounted for 80
Conclusions. Caries progression or percent of the caries in permanent teeth. By age 17 years,
reversal is determined by the balance
between protective and pathological fac- however, 40 percent of the population accounted for 80 per-
tors. Fluoride, the key agent in battling cent of the caries.1-6 These findings illustrate the need for
caries, works primarily via topical mech-
anisms: inhibition of demineralization, management of caries by individual risk assessment and
enhancement of remineralization and for measures more specifically directed to high-risk people
inhibition of bacterial enzymes.
Clinical Implications. Fluoride in drink- and populations.
ing water and in fluoride-containing Although these prevalence rates still leave much to be
products reduces caries via these topical
mechanisms. Antibacterial therapy must desired, the overall caries prevalence in children has
be used to combat a high bacterial chal- indeed declined in the United States. Smaller epidemiolog-
lenge. For practical caries management
and prevention or reversal of dental ic studies in recent years indicate, however, that the
caries, the sum of the preventive factors decline in caries has not continued during the 1990s and
must outweigh the pathological factors.
that it may have plateaued.6
JADA, Vol. 131, July 2000 887
Copyright ©1998-2001 American Dental Association. All rights reserved.
COVER STORY
The reasons for the reduc- plaque are acidogenic—that is, Any fermentable carbohy-
tions in caries prevalence dur- they produce acids when they drate (such as glucose, sucrose,
ing the last 20 years are diffi- metabolize fermentable carbo- fructose or cooked starch) can
cult to pinpoint. Strong evi- hydrates.12,14,15 These acids can be metabolized by the acido-
dence exists, however, that the dissolve the calcium phosphate genic bacteria and create the
near universal use of fluoride- mineral of the tooth enamel or aforementioned organic acids as
containing products such as dentin in a process known as byproducts.22 The acids diffuse
dentifrice, mouthrinses and top- demineralization.16-18 If this through the plaque and into the
ical gels applied in the dental process is not halted or re- porous subsurface enamel (or
office have been major contribu- versed via remineralization— dentin, if exposed), dissociating
tors.7,8 Earlier caries reductions the redeposition of mineral via to produce hydrogen ions as
of 40 to 70 percent (before the saliva—it eventually becomes a they travel.17,23 The hydrogen
1970s) had resulted from the frank cavity. ions readily dissolve the miner-
fluoridation of public water sup- Dental caries of the enamel al, freeing calcium and phos-
plies in many communities.9-12 typically is first observed clini- phate into solution, which can
Dental caries in adults also cally as a so-called “white-spot diffuse out of the tooth. Most
continues to be a major prob- lesion.” This is a small area of importantly, lactic acid dissoci-
lem, as illustrated by a recent subsurface demineralization ates more readily than the
U.S. survey.13 The survey beneath the dental plaque. The other acids, producing hydrogen
reported that 94 percent of all ions that rapidly lower the pH
dentate adults (aged 18 years in the plaque.17 As the pH is
or older) had evidence of treat- lowered, acids diffuse rapidly
ed or untreated coronal caries. The mutans into the underlying enamel or
Caries obviously still is a streptococci and dentin.
major problem in adults, as the lactobacilli, The two most important
well as children, and we need groups of bacteria that predom-
an improved approach to pre- either separately inantly produce lactic acid are
vention and therapy. This arti- or together, are the mutans streptococci and the
cle reviews and summarizes the the primary lactobacilli.14 Each group con-
scientific basis for and practice tains several species, each of
of successful intervention in causative agents of which is cariogenic. Mutans
the caries process. dental caries. streptococci include Strep-
tococcus mutans and S. sobri-
THE CARIES PROCESS
nus. The lactobacilli species
Bacterial plaque and acid also are prolific producers of
production. The caries process body of the subsurface lesion lactic acid and appear in plaque
is now well-understood; much of may have lost as much as 50 before caries is clinically
it has been described extensively percent of its original mineral observed.24,25 These two groups
in the dental literature. Some content and often is covered by of bacteria, either separately or
details of the caries process an “apparently intact surface together, are the primary
remain to be unraveled, but, in layer.”19 The surface layer forms causative agents of dental
general, we understand the by remineralization. The caries.
process well enough to initiate process of demineralization con-
HOW FLUORIDE
better-targeted methods of caries tinues each time there is carbo- COMBATS THE
prevention and intervention. hydrate taken into the mouth CARIES PROCESS
The mechanism of dental that is metabolized by the bac-
caries formation is essentially teria. The saliva has numerous The ability of fluoride to pre-
straightforward.1 Plaque on the roles, including buffering (neu- vent and arrest caries has been
surface of the tooth consists of a tralizing) the acid and reminer- researched extensively. Fluo-
bacterial film that produces alization by providing minerals ride has three principal topical
acids as a byproduct of its that can replace those dissolved mechanisms of action:
metabolism.14,15 To be specific, from the tooth during deminer- dinhibiting bacterial metabo-
certain bacteria within the alization.1,20,21 lism after diffusing into the
888 JADA, Vol. 131, July 2000
Copyright ©1998-2001 American Dental Association. All rights reserved.
COVER STORY
bacteria as the hydrogen fluo-
ride, or HF, molecule when the
plaque is acidified;
dinhibiting demineralization
when fluoride is present at the
crystal surfaces during an acid
challenge;
denhancing remineralization
and thereby forming a low-
solubility veneer similar to the
acid-resistant mineral fluorap-
atite, or FAP, on the remineral-
ized crystals.
Inhibiting bacterial
metabolism. Several investiga-
tors have studied the possible
A
effects of fluoride on oral bacte-
ria.26-28 The most significant
finding reported is that the ion-
ized form of fluoride, or F-, can-
not cross the cell wall and
membrane but can rapidly trav-
el into the cariogenic bacterial
cells in the unchanged form as
HF.26-28
When the pH in the plaque
falls as the bacteria produce
acids, a portion of the fluoride
present in the plaque fluid then
combines with hydrogen ions to
form HF and rapidly diffuses
into the cell, effectively drawing
more HF from the outside.1,26-28
Once inside the cell, the HF dis- B
sociates, acidifying the cell and
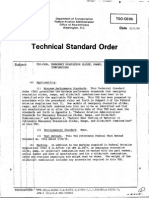
Figure 1. High-resolution electron microscope images (magnification
releasing fluoride ions that approximately ¥2,000,000) of individual enamel crystals. The black
interfere with enzyme activity lines are rows of calcium atoms, which are visualized by this tech-
in the bacterium. For example, nique. A. Normal enamel crystal showing white patches (arrows),
which are calcium-deficient and carbonate-rich defect regions.
fluoride inhibits enolase, an B. Demineralized crystal from the body of a natural caries lesion
enzyme necessary for the bacte- showing “large” hexagonal holes coinciding with the “small” defect
regions seen in normal enamel. (Adapted from Featherstone and col-
ria to metabolize carbohydrates. leagues30,31 with permission from Karger, Basel.)
As fluoride is trapped in the
cell, the process becomes cumu- and bones is a carbonated ing tooth development, with the
lative. hydroxyapatite29 that can be carbonate (CO3) ion in particu-
In summary, fluoride from approximately represented by lar causing major disturbances
topical sources is converted par- this simplified formula: in the regular array of ions in
tially to HF by the acid that the Ca10-x(Na)x(PO4)6-y(CO3)z the crystal lattice.30,31 During
bacteria produce and diffuses (OH)2-u(F)u demineralization, the carbonate
into the cell, thereby inhibiting The substitutions in the is lost, and during remineral-
essential enzyme activity. hydroxyapatite crystal lattice ization it is excluded from the
Inhibiting demineraliza- (the arrangement of atoms and newly formed mineral. The cal-
tion. The mineral of our teeth ions in the crystal) occur as the cium-deficient, carbonate-rich
(enamel, cementum, dentin) mineral is first laid down dur- regions of the crystal are espe-
JADA, Vol. 131, July 2000 889
Copyright ©1998-2001 American Dental Association. All rights reserved.
COVER STORY
tion than fluoride incorporated
8
into the crystals at the levels
▲
● ▲ ▲ ▲ ▲ ▲ ▲
● found in enamel.21,35 Ten Cate,21
7 ●
■ Nelson and colleagues35 and
●
6 ●
Featherstone and colleagues36,37
found no measurable reduction
5 ● ■
●
■ ■ ■ in the acid solubility of synthet-
■ ■
pH
ic CAP (3 percent CO3 by
4
weight, comparable to that of
3 dental enamel mineral) with
about 1,000 ppm fluoride incor-
2 porated. Importantly, this
means that fluoride incorporat-
1
ed during tooth mineral devel-
0
opment at normal levels of 20
0 5 10 15 20 25 30 to 100 ppm (even in areas that
have fluoridated drinking water
TIME (MINUTES)
or with the use of fluoride sup-
plements) does not measurably
● ■ ▲ alter the acid solubility of the
Subjects with Subjects with Subjects mineral. Even when the outer
normal salivary flow xerostomia who ingested
who ingested who ingested a sugar-free enamel has higher fluoride lev-
sucrose sucrose sweetened product
els, such as 1,000 ppm, it does
not measurably withstand acid-
Figure 2. Typical pH curves for normal subjects with normal salivary
flow and for subjects with xerostomia (mean for each group) after induced dissolution any better
ingestion of sucrose. A curve for ingestion of a sugar-free sweetened than enamel with lower levels
product is shown for comparison. (Reproduced from Featherstone1
with permission of the publisher. Copyright ©1999, Munksgaard.)
of fluoride. Only when fluoride
is concentrated into a new crys-
cially susceptible to attack by the OH- ion in pure hydroxyap- tal surface during remineraliza-
the acid hydrogen ions during atite is completely replaced by tion is it sufficient to beneficial-
demineralization, as has been an F- ion. The resulting mineral ly alter enamel solubility. The
shown by several investiga- FAP is highly resistant to disso- fluoride incorporated develop-
tors.21,29-33 High-resolution lat- lution by acid. mentally—that is, systemically
tice imaging, which images Fluoride inhibits demineral- into the normal tooth mineral—
crystals almost to atomic reso- ization. Sound enamel, except is insufficient to have a measur-
lution (viewed at about in its outer few micrometers, able effect on acid solubility.21,38
×2,000,000 magnification), was generally contains fluoride at In contrast to the lack of
used to illustrate the appear- levels of about 20 to 100 parts effect of fluoride incorporated
ance of hexagonal holes in the per million, or ppm, depending into the CAP crystals of tooth
early stages of enamel crystal on the fluoride ingestion during mineral developmentally, as lit-
dissolution in dental caries tooth development.34 Teeth in tle as 1 ppm in the acid solution
(Figure 1), which coincided with children who lived in areas reduced the dissolution rate of
the calcium-deficient, carbon- with fluoridated drinking water CAP to a rate equivalent to
ate-substituted regions of the during tooth development have that of HAP.36 Further increas-
crystal.30-33 fluoride content toward the es in fluoride in the acid solu-
The carbonated hydroxyap- higher end of this range. The tion in contact with the CAP
atite, or CAP, of our teeth is outer few micrometers of en- mineral surface decreased the
much more soluble in acid than amel can have fluoride levels of solubility rate logarithmically.
hydroxyapatite, or HAP 1,000 to 2,000 ppm.34 These results indicate that if
(HAP = Ca10(PO4)6(OH)2), and Fluoride in the solution sur- fluoride is present in the aque-
that in turn is much more solu- rounding CAP crystals has been ous solution surrounding the
ble than fluorapatite, or FAP shown to be much more effec- crystals, it is adsorbed strongly
(FAP = Ca10(PO4)6F2),21 in which tive in inhibiting demineraliza- to the surface of CAP carbonat-
890 JADA, Vol. 131, July 2000
Copyright ©1998-2001 American Dental Association. All rights reserved.
COVER STORY
ed apatite (enamel mineral)
crystals and thus acts as a
potent protection mechanism
against acid dissolution of the
crystal surface in the tooth’s
subsurface region. If fluoride is
in the plaque fluid at the time
that the bacteria generate acid,
it will travel with the acid into
the subsurface of the tooth and,
therefore, adsorb to the crystal
surface and protect it against
being dissolved.
In summary, fluoride present
in the water phase at low levels
among the enamel or dentin
crystals adsorbs to these crystal
surfaces and can markedly
inhibit dissolution of tooth min-
eral by acid.21,36 Fluoride that
A
acts in this way comes from the
plaque fluid via topical sources
such as drinking water and
fluoride products. Fluoride
incorporated during tooth
development is insufficient to
play a significant role in caries
protection. Fluoride is needed
regularly throughout life to pro-
tect teeth against caries.
Enhancing remineraliza-
tion. As the saliva flows over
the plaque and its components
neutralize the acid, raising the
pH (Figure 2), demineralization
is stopped and reversed. The
saliva is supersaturated with
calcium and phosphate, which
can drive mineral back into the
tooth.21,39 The partially deminer- B
alized crystal surfaces within
Figure 3. High-resolution electron microscope images (magnification
the lesion act as “nucleators,” approximately ×2,000,000) of individual enamel crystals that visualize
and new surfaces grow on the remineralization at the atomic level. The black lines are rows of calcium
atoms, which are visualized by this technique. A. Normal enamel crystal
crystals (Figure 3). These dissected from the inner region of enamel, showing “small” white
processes constitute remineral- patches of calcium-deficient, carbonate-rich regions. B. Crystal on
ization—the replacement of which a “remineralized” surface veneer has been grown after treat-
ment with fluoride, calcium and phosphate. (Adapted from Featherstone
mineral in the partially de- and colleagues, 198130 with permission from Karger, Basel.)
mineralized regions of the cari-
ous lesion of enamel or dentin um ions, followed by phosphate where between HAP and FAP
(including the tooth root).20,21 ions, leading to new mineral as described above (Figure 4).
Fluoride enhances remineral- formation. The newly formed FAP contains approximately
ization by adsorbing to the crys- “veneer” excludes carbonate 30,000 ppm F and has a very
tal surface and attracting calci- and has a composition some- low solubility in acid. The new
JADA, Vol. 131, July 2000 891
Copyright ©1998-2001 American Dental Association. All rights reserved.
COVER STORY
bacterial substances and
ACID
buffers.40 The saliva compo-
Enamel crystal = Partly dissolved nents neutralize the acids pro-
carbonated apatite crystal duced by bacterial metabolism
in the plaque, raise the pH and
reverse the diffusion gradient
Calcium +
Remineralization
phosphate
for calcium and phosphate.
+ fluoride Thereby, they return calcium
and phosphate to the subsur-
face lesion, where these ions
Ca10 (PO4)6 (F)2 =
fluorapatitelike can regrow new surfaces on the
coating on crystals Crystal crystal remnants that were pro-
nucleus duced by demineralization.
These so-called “remineralized”
crystals have a veneer of much
less soluble mineral. Saliva also
Figure 4. Schematic representation of demineralization followed by
clears carbohydrates and acids
remineralization in the caries process. If remineralization is successful, from the plaque.
the final result is a crystal with a surface veneer of “fluorapatitelike” In the case of salivary dys-
mineral of low solubility. (Reproduced from Featherstone1 with permis-
sion of the publisher. Copyright ©1999, Munksgaard.) function,41 all of the above bene-
fits of saliva are reduced or
eliminated (as is illustrated
partially in Figure 2 by the pH
Protective Factors Pathological Factors
profile of the subjects with
Salivary flow and components Reduced salivary function xerostomia).
Proteins, antibacterial components Bacteria: mutans streptococci,
and agents lactobacilli THE CARIES BALANCE
Fluoride, calcium and phosphate Dietary components: frequency
Dietary components: protective carbohydrates Fluoride’s three extensively
studied and documented princi-
pal mechanisms of action rely
on the presence of fluoride in
saliva, in the plaque at the
NO CARIES CARIES tooth surface and in the fluid
among the crystals in the sub-
surface of the enamel or dentin.
Figure 5. The caries balance: a schematic diagram of the balance
between pathological and protective factors in the caries process.
The clinical effects of fluoride,
(Reproduced from Featherstone1 with permission of the publisher. therefore, can be optimized by
Copyright ©1999, Munksgaard.) using delivery methods that
bring fluoride to the surface of
remineralized crystal now will ubility than the original CAP the tooth and into the plaque
behave like low-solubility FAP tooth mineral. Subsequent acid rather than incorporating fluo-
rather than the highly soluble challenges must be quite strong ride into the tooth mineral crys-
CAP of the original crystal and prolonged to dissolve the tals during tooth development.
surface.36 remineralized enamel. These topical delivery methods
In summary, fluoride in solu- Saliva and caries. Saliva has are equally applicable to adults
tion from topical sources en- a critical role in the prevention and children and include fluo-
hances remineralization by or reversal of the caries process; ride in beverages and foods,
speeding up the growth of a it provides calcium, phosphate, dental products and drinking
new surface on the partially proteins that maintain super- water. The benefits of continu-
demineralized subsurface crys- saturation of calcium in the ally providing low levels of fluo-
tals in the caries lesion. The plaque fluid, proteins and lipids ride in the saliva and plaque
new crystal surface veneer is that form a protective pellicle from the aforementioned topical
FAP-like, with much lower sol- on the surface of the tooth, anti- sources are described more fully
892 JADA, Vol. 131, July 2000
Copyright ©1998-2001 American Dental Association. All rights reserved.
COVER STORY
in a recent review article.1 showed the posteruptive (topi- um and phosphate, which are
Pathological and protec- cal) effects of fluoride in the derived primarily from saliva
tive factors in the caries bal- drinking water. Other studies and plaque fluid.
ance. Caries progression, as have illustrated the weak pre- Pathological factors. Patho-
opposed to reversal, consists of eruptive effects of fluoride. For logical factors obviously include
a delicate balance between the example, in two groups of cariogenic bacteria and the fre-
aforementioned factors—name- Okinawa nursing students aged quency of ingestion of ferment-
ly, a bacterially generated acid 18 to 22 years, there was no dif- able carbohydrates that sustain
challenge and a combination of ference in caries status between these bacteria. The importance
demineralization inhibition and those who had received fluori- of mutans streptococci (which
reversal by remineralization.1,42 dated water only until about 5 includes S. mutans and S.
The balance between pathologi- to 8 years of age (and none sobrinus) in the development of
cal factors (such as bacteria and thereafter) and those who had dental caries has been reviewed
carbohydrates) and protective never received fluoridated extensively.12,14,15,49,50 Numerous
factors (such as saliva, calcium, drinking water.44 cross-sectional studies in
phosphate and fluoride) is a The cariostatic effects of fluo- humans have shown that great-
delicate one that swings either ride are, in part, related to the er numbers of mutans strep-
way several times daily in most sustained presence of low con- tococci and lactobacilli in saliva
people (Figure 5). centrations of ionic fluoride in or plaque are associated with
Protective factors. Saliva is the oral environment,1,21,38 high caries rates.15,25,49,51-54
essential for the protection of Longitudinal studies have
the tooth against dental caries shown that an increase over
and provides many natural pro- There is the time in numbers of both of
tective factors summarized ear- these bacterial groups is
lier,40,41 including calcium, phos- mistaken belief associated with caries onset
phate, antibacterial components that drilling out and progression.24,55,56
and other proteins with various a caries lesion CARIES INTERVENTION
functions. Extrinsic antibacteri-
al agents such as chlorhexidine and placing a The methods of caries interven-
also can be considered as pro- restoration tion can be summarized by join-
tective factors in this balance, eliminates the ing the principal components of
as can fluoride from external the caries process with the
sources. The mechanisms of bacteria and interventional possibilities
action of fluoride described in thereby stops (Table).
this article apply primarily to caries Cariogenic bacteria and
fluoride from topical sources; high bacterial challenge.
systemically incorporated fluo- progression. Dental caries is a transmissible,
ride has only a minor role in bacterially generated disease.
protecting against dental caries. There is the mistaken belief
This conclusion is supported not derived from foods and bever- that drilling out a caries lesion
only by laboratory data as ages, drinking water and fluo- and placing a restoration elimi-
described previously, but also ride-containing dental products nates the bacteria and thereby
by epidemiologic studies. For such as toothpaste. Prolonged stops caries progression. Al-
example, a four-year study in and slightly elevated low con- though traditional restorative
England found a 27 percent centrations of fluoride in the work may eliminate the bacte-
lower caries incidence among saliva and plaque fluid decrease ria at the site of the restoration,
children who were 12 years old the rate of enamel demineral- the remainder of the mouth is
when water fluoridation began ization and enhance the rate of left untouched, caries continues
in their communities, relative remineralization.21,36,38,45-48 For unchecked in the remainder of
to the incidence in control sub- example, fluoride at 0.04 ppm the mouth and recolonization
jects of the same age in nonfluo- in saliva can enhance reminer- commences rapidly at the
ridated areas.43 This was a well- alization. Remineralization of margins.57
conducted study, and it clearly early lesions also requires calci- It is logical, therefore, to use
JADA, Vol. 131, July 2000 893
Copyright ©1998-2001 American Dental Association. All rights reserved.
COVER STORY
TABLE
SUMMARY: THE CARIES PROCESS AND METHODS OF CARIES INTERVENTION.
CARIES COMPONENT INTERVENTION METHOD
Bacteria Antibacterial therapy such as treatment with
chlorhexidine gluconate (see text)
Carbonated Hydroxyapatite Make the mineral less soluble by transforming
it to other crystalline forms such as hydroxy-
apatite without carbonate (future caries-
preventive treatments by specific laser irradia-
tion will enable this to be done69,70)
Fermentable Carbohydrates Reduce the frequency of ingestion; substitute
with noncariogenic sweeteners (this method is
well-accepted and used in patient education)
Recommend use of sugar-free chewing gum,
which reduces frequency of fermentable carbo-
hydrate ingestion and also enhances reminer-
alization
Organic Acids Produced by Neutralize the acid by providing extra buffer-
Oral Bacteria ing or enhancing saliva; sugar-free gum assists
in this as well
Saliva Enhance the saliva flow and function
Fluoride Exploit its known effects on bacteria, inhibi-
tion of demineralization and enhancement of
remineralization by using “topical” fluoride
delivery by means of dental products, drinking
water, beverages and foods
antibacterial therapy—such as one-to-one direct correlation tors are in balance, caries does
treatment with chlorhexidine between levels of these bacteria not progress. If they are out of
gluconate rinse—as a caries- and caries progression.24,49 balance, caries either progresses
preventive measure. Although However, it now is well-estab- or reverses.
this has been proposed for lished that high levels of Antibacterial therapy for
many years58-60 and used in sev- mutans streptococci, high levels caries control. Currently, the
eral European countries, an of lactobacilli or both constitute most successful antibacterial
antibacterial approach almost a “high bacterial challenge.”24 therapy against cariogenic bac-
never is used in the United This bacterial challenge can be teria is treatment by chlorhexi-
States for the prevention of the balanced by the protective fac- dine gluconate rinse or gel.47,61
progression of dental caries. tors described earlier, which Chlorhexidine is available by
One of the difficulties in per- include salivary components— prescription in the United
suading clinicians to use the especially calcium, phosphate States. Studies have shown that
antibacterial approach is that and fluoride—and the amount a daily dose of chlorhexidine
there have not been rapid and of saliva present.42 rinse for two weeks can
accurate methods of determin- Figure 5 illustrates the bal- markedly reduce the cariogenic
ing the levels of cariogenic bac- ance between pathological fac- bacteria in the mouth and that,
teria in the mouth. Further- tors (including cariogenic bacte- as a result, recolonization takes
more, although numerous ria, reduced salivary function place in three to six months
studies have indicated that and frequency of use of fer- rather than immediately.58 In
mutans streptococci and lacto- mentable carbohydrates) and patients with high levels of bac-
bacilli definitely are risk factors protective factors. If these teria, therefore, chlorhexidine
for dental caries, there is no pathological and protective fac- treatments at three-month
894 JADA, Vol. 131, July 2000
Copyright ©1998-2001 American Dental Association. All rights reserved.
COVER STORY
intervals are indicated. probes will be available com- assess the level of risk of
The problem faced by clini- mercially in the near future, caries progression in individ-
cians is how to determine, in a and that clinicians will be able ual patients. Studies still are
timely fashion, whether the to use them chairside and under way, and there is no
bacterial challenge is high, obtain results within a few definitive formula yet avail-
medium or low. For many minutes. This will enable clini- able. The status of risk assess-
years, commercial “dip slides” cians to determine the quanti- ment was summarized, how-
have been available in Europe, tative levels of bacteria in a ever, by the authors of a spe-
and they recently became patient’s mouth while he or cial supplement to The
available in the United she is in the operatory and to Journal of the American
States.58 A saliva sample is factor these numbers into an Dental Association in 1995;
taken from the patient and overall risk assessment of this publication can be used as
incubated on the dip slide; two caries for that patient. It is a guide until more definitive
days later, a result is provided envisaged that computer pro- information is available.64
of the levels of S. mutans and grams will be available that Figure 5 represents a basis for
lactobacilli bacteria in the will include the assay num- determining caries risk with
mouth.58 Although these slides bers, as well as other data. the information currently
are a major advance in conven- The practitioner will receive available.
ience and are the best tools guidance as to the level of It has been established that
available at the time of this high-risk patients include
writing, it has been shown those who have a high bacteri-
that this technology is not Methods of al challenge, which may con-
well-correlated with tradition- sist of a combination of high
rapid chairside
al bacterial plating. It is antic- numbers of mutans streptococ-
ipated that methods of rapid assessment of ci, lactobacilli or both.
chairside assessment of bacter- bacterial Although fluoride has excel-
ial challenge, based on molecu- lent properties in terms of bal-
challenge, based
lar biology, will be available in ancing caries challenge, if the
the future. on molecular challenge is too high, then
Several investigators have biology, will be fluoride—even at increased
explored the possibility of concentrations, with increased
available in the
using modern molecular biolo- use or both—cannot balance
gy for better and more rapid future. that challenge. Therefore, in
methods of bacterial assess- the case of high bacterial chal-
ment,62 but they were unable lenge, the bacterial infection
to overcome a number of com- caries risk and what regimen must be dealt with, typically
plications. An exciting devel- or regimens to use to prevent with a chlorhexidine rinse, as
opment is work by Shi and col- further caries and to reduce well as the enhancement of
leagues,63 who recently pub- the bacterial challenge. With salivary action by topical
lished a method using species- the new monoclonal antibody delivery of fluoride. These
specific monoclonal antibodies probes, the levels of bacteria principles apply equally well
that recognize the surface of and success of the intervention to adults and children.
cariogenic bacteria. With this could readily be followed over Accurate detection of early
technology, it is not necessary time. This is an exciting, inno- caries can increase the relia-
to split open the bacterial cells vative tool that may become bility of caries risk assess-
to assess the internal DNA or widely used and accepted ment, particularly if those
RNA. These probes can be within a few years. measurements are made at
tagged either with a fluo- three- or six-month intervals
CARIES RISK
rescent molecule or with a ASSESSMENT
and caries progression can be
marker that can be measured measured. In the case of caries
quantitatively in a simple Several studies have attempt- progression, obviously, inter-
spectrophotometer. ed to determine risk factors vention is needed either anti-
It is anticipated that these that can be reliably used to bacterially, with fluoride or
JADA, Vol. 131, July 2000 895
Copyright ©1998-2001 American Dental Association. All rights reserved.
COVER STORY
many years is an immuniza-
Pulsed laser light with high tion against caries. There are
absorption coefficient many obstacles to the success
of immunization, as caries is
Removes carious tissue; not a systemic infection that
minimal heat deposition
can be dealt with simply by
Walls of preparation heated administering a specific anti-
Enamel to 800-900 C biotic. The infection must be
dealt with in the mouth, where
Heat conduction the internal body fluids do not
Dentin pass and, therefore, the normal
Pulp temperature rise < 4 C immune response is not rele-
Pulp
vant. However, IgA that is pro-
duced by the saliva naturally
Figure 6. Schematic diagram showing the potential use of specific can interfere with the coloniza-
lasers for precise removal of carious enamel and modification of the tion of the surface of the tooth
surrounding enamel for prevention of further caries progression after
restoration. The laser would be set first to remove a minimum of cari-
by specific bacteria.
ous tissue. Then the walls and base of the cavity preparation would be Recent studies by Ma and
treated with the laser to inhibit subsequent caries progression. colleagues 65,66 have illustrated
(Reproduced from Featherstone71 with the permission of the publisher.
Copyright © 2000 Indiana University School of Dentistry.) the effectiveness of specific IgA
in the inhibition of recoloniza-
with other techniques, some of will become less and less tion of mutans streptococci.
which are described in the fol- desirable as a treatment and The next logical step is to use
lowing material. will be used only as a final this technology as one of the
Caries management by resort when new intervention tools for caries intervention. It
risk assessment. As the measures have failed or when is possible to use genetically
caries risk assessment people have not participated engineered plants, such as
methodologies are refined, we in caries intervention pro- tobacco or alfalfa, to produce
will have more definitive bio- grams such as those indicated immunoglobulins.66.67 A study is
logical and chemical risk previously. in progress at the University of
assessment measures to guide California, San Francisco, to
CARIES MANAGEMENT
clinical decision making. TOOLS FOR THE FUTURE
test IgA that has been pro-
These measures form the duced using genetically engi-
basis for assessing the direc- Several technological advance- neered tobacco plants. At press
tion in which the caries bal- ments are currently close to time, the results were not
ance is likely to move for a clinical reality and will be known, but if the trial is suc-
particular patient. Early embraced if they are proven cessful, this IgA can be applied
caries detection, especially in successful. to the teeth after chlorhexidine
occlusal surfaces, is an essen- Assessment of bacterial treatment has removed the car-
tial part of caries management challenge by chairside iogenic bacteria, with the aim
by risk assessment. molecular probes. The use of inhibiting future recoloniza-
Caries management by risk of chairside bacterial probes tion by mutans streptococci.
assessment now is receiving for assessing a patient’s cario- Early caries detection
considerable attention, and genic bacterial challenge will and intervention. Successful
software programs are being be an essential component of use of the innovative methods
developed that will aid practi- caries management by risk described here for caries inter-
tioners in assessing risk and assessment. vention will require accurate
lead them to the use of cur- Caries immunization. In methods for the early detection
rent and new technologies by a program of caries manage- of dental caries in enamel
specifying treatments recom- ment by risk assessment, it is and dentin. Early-detection
mended for the various risk logical that all available tools methods such as fluorescence,
categories.59,60 As we move into should be used. One such tool optical coherence tomography,
the future, tooth restorations that has been investigated for electrical impedance and
896 JADA, Vol. 131, July 2000
Copyright ©1998-2001 American Dental Association. All rights reserved.
COVER STORY
ultrasonography are likely to laser for use on teeth. This was mineralization-remineraliza-
become available for use by cli- the first approval for laser use tion model in the laboratory by
nicians in the near future.68 It on dental hard tissues. This up to 85 percent. They have
will be possible to detect approval by the FDA was for demonstrated that carbonate is
lesions in the occlusal surface this particular laser to be used lost from the CAP mineral of
and to determine whether they for the removal of dental caries the tooth during specific laser
have progressed into the dentin and the cutting of sound tissue irradiation, making the miner-
and, if so, how far. This is not before the placement of restora- al highly resistant to dissolu-
possible with current radio- tions. This event has ushered tion by acid. Although they
graphic technology. in a new era for lasers in den- have demonstrated in the labo-
Once new methods are intro- tistry. Since then, other lasers ratory, using pH cycling mod-
duced for the early detection of have been approved for the els, that as little as 20 pulses of
caries, they can be used in two same purpose, and additional 100 microseconds each can pro-
opposing fashions. Clinicians hard-tissue uses are likely to duce a preventive effect similar
with traditional training are be approved in the future, to daily use of fluoride denti-
likely to use these methods to including the use of lasers for frice, these promising and
intervene physically at an ear- the inhibition of progression of exciting results have not yet
lier stage with carious dental caries by altering the been tested in human mouths.70
lesions—drilling, filling and composition of surface enamel For practical purposes, it
placing restorations. This out- would be desirable to develop a
come is of concern, as many laser that can remove carious
more restorations would be As innovative tissue and subsequently be
placed than may be necessary, used to treat the walls of the
which weakens the tooth struc- methods for area from which carious tissue
ture. Early detection and inter- early caries is removed to make them
vention by placing a restoration intervention resistant to subsequent caries
also does not take advantage of challenge71 (Figure 6). Fried
the body’s natural protective are introduced, and colleagues72 recently pub-
mechanisms of inhibition of the need for lished a report on a new CO2
demineralization and enhance- restorations may laser that efficiently removes
ment of remineralization via carious tissue. After caries and
saliva. be eliminated for a minimal amount of surround-
Alternatively, early detection many patients. ing tissue are removed, it will
of caries can be used as an be possible to change the laser
opportunity to promote re- parameters to perform caries-
mineralization via salivary or dentin mineral. preventive treatment on the
enhancement, use of topical Kantorowitz and colleagues 69 same area. This would be fol-
fluoride and chlorhexidine and and Featherstone and col- lowed by placement of a resin-
meticulous oral hygiene. In leagues 70 have studied the based composite restoration,
addition, as innovative meth- effects of lasers on hard tissues thereby inhibiting subsequent
ods for early caries interven- for almost 20 years. The overall caries around that restoration.
tion are introduced, the need objective of these studies is to For example, if an early oc-
for restorations may be elimi- establish the scientific basis for clusal lesion was detected (by
nated for many patients, there- the choice of laser parameters the new methods described pre-
by preserving the tooth struc- that can be used clinically for viously) that was deemed to be
ture and halting or reversing the prevention, removal or beyond hope of remineraliza-
progression of dental caries. treatment of caries lesions. tion, this lesion could be con-
Caries prevention by Their studies have demonstrat- servatively removed with an
laser treatment. In May 1997, ed that specific pulsed carbon appropriate laser. Then the
the U.S. Food and Drug dioxide, or CO2, laser treat- surrounding cavity preparation
Administration approved the ment of dental enamel can walls could be treated for caries
use of an erbium:yttrium- inhibit subsequent carieslike prevention by the laser and a
aluminum-garnet, or Er:YAG, progression in a severe de- small conservative restoration
JADA, Vol. 131, July 2000 897
Copyright ©1998-2001 American Dental Association. All rights reserved.
COVER STORY
placed. The cavity walls will be health of their patients. ■ 15. Loesche WJ, Hockett RN, Syed SA. The
predominant cultivable flora of tooth surface
highly resistant to acid attack plaque removed from institutionalized sub-
Dr. Featherstone is a professor and the
and therefore resistant to sec- chair, Department of Preventive and
jects. Arch Oral Biol 1972;17(9):1311-25.
16. Featherstone JD. An updated under-
ondary caries. Providing bacter- Restorative Dental Sciences and Department standing of the mechanism of dental decay
of Dental Public Health and Hygiene,
ial intervention via chlorhexi- University of California, San Francisco, 707
and its prevention. Nutr Q 1990;14:5-11.
17. Featherstone JD, Rodgers BE. Effect of
dine rinse was also part of the Parnassus Ave., Box 0758, San Francisco, acetic, lactic and other organic acids on the
Calif. 94143, e-mail “jdbf@itsa.ucsf.edu”.
treatment in the same patient, Address reprint requests to Dr.
formation of artificial carious lesions. Caries
Res 1981;15(5):377-85.
future caries would be unlikely. Featherstone. 18. Featherstone JD, Mellberg JR. Relative
rates of progress of artificial carious lesions
SUMMARY AND The author sincerely acknowledges contri- in bovine, ovine and human enamel. Caries
CONCLUSIONS butions from numerous colleagues over many Res 1981;15(1):109-14.
years to much of the work reviewed here. 19. Silverstone LM. Structure of carious
enamel, including the early lesion. Oral Sci
The mechanism of dental caries 1. Featherstone JD. Prevention and rever- Rev 1973;3:100-60.
is well-established to the point sal of dental caries: role of low level fluoride. 20. ten Cate JM, Duijsters PP. Influence of
Community Dent Oral Epidemiol 1999; fluoride in solution on tooth demineralization.
where new approaches are 27(1):31-40. II. Microradiographic data. Caries Res 1983;
being made for caries preven- 2. Kaste LM, Selwitz RH, Oldakowski RJ, 17(6):513-9.
Brunelle JA, Winn DM, Brown LJ. Coronal 21. ten Cate JM, Featherstone JD.
tion based on a scientific under- caries in the primary and permanent denti- Mechanistic aspects of the interactions
standing of the processes tion of children and adolescents 1-17 years of between fluoride and dental enamel. Crit Rev
age: United States, 1988-1991. J Dent Res Oral Biol Med 1991;2(3):283-96.
involved. Several existing 1996;75:631-41. 22. Geddes DA. Acids produced by human
methodologies are available to 3. National Institute of Dental Research, dental plaque metabolism in situ. Caries Res
Epidemiology and Oral Disease Prevention 1975;9(2):98-109.
enable successful management Program. Oral health of United States chil- 23. Featherstone JD. Diffusion phenomena
of dental caries by risk assess- dren: The National Survey of Dental Caries and enamel caries development. In:
in U.S. School Children, 1986-1987—national Guggenheim B, ed. Proceedings of the
ment. Understanding the bal- and regional findings. Bethesda, Md.: U.S. Cariology Today International Congress,
ance between pathological fac- Department of Health and Human Services, September 1983, Zurich, Switzerland. Basel,
Public Health Service, National Institutes of Switzerland: Karger; 1984:259-68.
tors and protective factors is Health; 1989. NIH publication 89-2247. 24. Leverett DH, Proskin HM, Featherstone
the key. Beyond the well- 4. The prevalence of dental caries in United JD, et al. Caries risk assessment in a longitu-
States children 1979-1980: The National dinal discrimination study. J Dent Res
established and currently used Dental Caries Prevalence Survey. Bethesda, 1993;72(2):538-43.
methods, some innovative and Md.: U.S. Department of Health and Human 25. Leverett DH, Featherstone JD, Proskin
Services, Public Health Service, National HM, et al. Caries risk assessment by a cross-
exciting techniques have shown Institutes of Health; 1981. NIH publication sectional discrimination model. J Dent Res
early research successes that 82-2245. 1993;72(2):529-37.
5. National Center for Health Statistics. 26. Hamilton IR, Bowden GH. Fluoride
most likely will be used for Decayed, missing and filled teeth among effects on oral bacteria. In: Fejerskov O,
early caries intervention in the youths, 12-17 years: United States, 1974. Ekstrand J, Burt BA, eds. Fluoride in den-
Vital and Health Statistics, Series 11-No. tistry. Copenhagen, Denmark: Munksgaard;
future. These methods include 144. Washington: Government Printing 1996:230-51.
fluoride therapy for inhibition of Office; 1974. DHEW publication (HRA) 27. Whitford GM, Schuster GS, Pashley
75-1626. DH, Venkateswarlu P. Fluoride uptake by
demineralization and enhance- 6. Speechley M, Johnston DW. Some evi- Streptococcus mutans 6715. Infect Immunol
ment of remineralization, mole- dence from Ontario, Canada, of a reversal in 1977;18(3):680-7.
the dental caries decline. Caries Res 1996; 28. Van Louveren C. The antimicrobial
cular probes for the quantita- 30(6):423-7. action of fluoride and its role in caries inhibi-
tive detection of cariogenic bac- 7. Jenkins GN. Recent changes in dental tion. J Dent Res 1990;69:676-81.
caries. Br Med J 1985;291(6505):1297-8. 29. LeGeros RZ. Calcium phosphates in oral
teria at chairside, computerized 8. Hargreaves JA, Thompson GW, Wagg biology and medicine. In: Myers HM, ed.
caries risk assessment pro- BJ. Changes in caries prevalence in Isle of Monographs in oral science. Basel,
Lewis children between 1971 and 1981. Switzerland: Karger; 1991:1-201.
grams, genetically engineered Caries Res 1983;17(6):554-9. 30. Featherstone JD, Nelson DG, McLean
IgA for inhibition of recoloniza- 9. Burt BA, Fejerskov O. Water fluorida- JD. An electron microscope study of modifica-
tion. In: Fejerskov O, Ekstrand J, Burt BA, tions to defect regions in dental enamel and
tion of cariogenic bacteria, spe- eds. Fluoride in dentistry. Copenhagen, synthetic apatites. Caries Res 1981;15(4):
cific lasers for conservative Denmark: Munksgaard; 1996:275-90. 278-88.
10. Murray JJ. Fluorides in caries preven- 31. Featherstone JD, Goodman P, McLean
removal of carious tissue and tion. 3rd ed. Oxford, England; Boston: JD. Electron microscope study of defect zones
specific lasers for the preven- Butterworth-Heinemann; 1991. in dental enamel. J Ultrastruc Res 1979;67:
11. Newbrun E. Effectiveness of water fluo- 117-23.
tion of caries progression. ridation. J Public Health Dent 1989;49: 32. Nelson DG, McLean JD. High-resolution
The use of these technologies 279-89. electron microscopy of octacalcium phosphate
12. Newbrun E. Cariology. 3rd ed. Chicago: and its hydrolysis products. Calcif Tissue Int
will require extensive retraining Quintessence; 1989:63-87, 331-49. 1984;36(2):219-32.
of clinical dentists. But it will 13. Winn DM, Brunelle JA, Selwitz RH, et 33. Nelson DG, McLean JD. Direct observa-
al. Coronal and root caries in the dentition of tion of near-atomic details in synthetic and
dramatically alter the way in adults in the United States, 1988-1991. J biological apatite crystallites. In: Fearnhead
which dentists diagnose, inter- Dent Res 1996;75:642-51. RW, Suga S, ed. Tooth enamel IV:
14. Loesche WJ. Role of Streptococcus Proceedings of the Fourth International
vene, treat and manage caries, mutans in human dental decay. Microbiol Symposium on the Composition, Properties,
with major benefits to the oral Rev 1986;50(4):353-80. and Fundamental Structure of Tooth Enamel.
898 JADA, Vol. 131, July 2000
Copyright ©1998-2001 American Dental Association. All rights reserved.
COVER STORY
Amsterdam, Netherlands: Elsevier Science frices. In: Embery G, Rolla R, eds. Clinical Dent Educ 1997;61(11):895-905.
Publishers; 1984:47-51. and biological aspects of dentifrices. Oxford, 61. Lagerlof F, Oliveby A. Clinical implica-
34. Robinson C, Kirkham J, Weatherell JA. England: Oxford University Press; 1992: tions: new strategies for caries treatment. In:
Fluoride in teeth and bone. In: Fejerskov O, 41-50. Stookey GH, Beiswanger B, eds. Indiana
Ekstrand J, Burt BA, eds. Fluoride in den- 48. Arends J, Nelson DG, Dijkman AG, Conference 1996: Early Detection of Dental
tistry. Copenhagen, Denmark: Munksgaard; Jongebloed WL. Effect of various fluorides on Caries. Indianapolis: Indiana University
1996:69-87. enamel structure and chemistry. In: School of Dentistry; 1996.
35. Nelson DG, Featherstone JD, Duncan Guggenheim B, ed. Proceedings of the 62. Cangelosi GA, Iversen JM, Zuo Y,
JF, Cutress TW. Effect of carbonate and fluo- Cariology Today International Congress, Oswald TK, Lamont RJ. Oligonucleotide
ride on the dissolution behaviour of synthetic September 1983, Zurich, Switzerland. Basel, probes for mutans streptococci. Mol Cell
apatites. Caries Res 1983;17(3):200-11. Switzerland: Karger; 1984:245-58. Probes 1994;8(1):73-80.
36. Featherstone JD, Glena R, Shariati M, 49. Krasse B. Biological factors as indica- 63. Shi W, Jewett A, Hume WR. Rapid and
Shields CP. Dependence of in vitro deminer- tors of future caries. Int Dent J 1988;38(4): quantitative detection of Streptococcus
alization of apatite and remineralization of 219-25. mutans with species-specific monoclonal anti-
dental enamel on fluoride concentration. J 50. Ellen RP. Microbiological assays for bodies. Hybridoma 1998;17(4):365-71.
Dent Res 1990;69:620-5. dental caries and periodontal disease suscep- 64. Caries diagnosis and risk assessment: a
37. Featherstone JD, Shields CP, tibility. Oral Sci Rev 1976;(8):3-23. review of preventive strategies and manage-
Khademazad B, Oldershaw MD. Acid reactiv- 51. Alaluusua S, Kleemola-Kujala E, ment. JADA 1995;126(suppl):1-24S.
ity of carbonated apatites with strontium and Nystrom M, Evalahti M, Gronroos L. Caries 65. Ma JK, Hunjan M, Smith R, Lehner T.
fluoride substitutions. J Dent Res 1983; in the primary teeth and salivary Strep- Specificity of monoclonal antibodies in local
62(10):1049-53. tococcus mutans and lactobacillus levels as passive immunization against Streptococcus
38. Fejerskov O, Thylstrup A, Larsen MJ. indicators of caries in permanent teeth. mutans. Clin Exp Immunol 1989;77(3):331-7.
Rational use of fluorides in caries prevention. Pediatr Dent 1987;9(2):126-30. 66. Ma JK, Hikmat BY, Wycott K, et al.
A concept based on possible cariostatic mech- 52. Klock B, Krasse B. Microbial and sali- Characterization of a recombinant plant mon-
anisms. Acta Odont Scand 1981;39(4):241-9. vary conditions in 9- to 12-year-old children. oclonal secretory antibody and preventive
39. Moreno EC, Kresak M, Zahradnick RT. Scand J Dent Res 1977;85(1):56-63. immunotherapy in humans. Nat Med
Physicochemical aspects of fluoride-apatite 53. Klock B, Emilson CG, Lind SO, 1998;4(5):601-6.
systems relevant to the study of dental Gustavsdotter M, Olhede-Westerlund AM. 67. Ma JK, Lehner T, Stabila P, Fux CI,
caries. Caries Res 1977;11:142-71. Prediction of caries activity in children with Hiatt A. Assembly of monoclonal antibodies
40. Lamkin MS, Oppenheim FG. Structural today’s low caries incidence. Community Dent with IgG1 and IgA heavy chain domains in
features of salivary function. Crit Rev Oral Oral Epidemiol 1989;17(6):285-8. transgenic tobacco plants. Eur J Immunol
Biol Med 1993;4:251-9. 54. Seppa L, Hausen H. Frequency of initial 1994;24(1):131-8.
41. Mandel ID. Relation of saliva and caries lesions as predictor of future caries 68. Stookey GK. Practical applications of
plaque to caries. J Dent Res 1974;53(2): increment in children. Scand J Dent Res early caries detection methods. In: Stookey
246-66. 1988;96(1):9-13. GK, ed. Early detection of dental caries II:
42. Featherstone JD. Clinical implications: 55. Loesche WJ, Eklund S, Earnest R, Burt 1999. Indianapolis: Indiana University School
New strategies for caries prevention. In: B. Longitudinal investigation of bacteriology of Dentistry (in press).
Stookey GK, ed. Indiana Conference 1996: of human fissure decay: epidemiological stud- 69. Kantorowitz Z, Featherstone JD, Fried
Early Detection of Dental Caries. Indianapo- ies in molars shortly after eruption. Infect D. Caries prevention by CO2 laser treatment:
lis: Indiana University School of Dentistry; Immunol 1984;46(3):765-72. dependency on the number of pulses used.
1996:287-95. 56. Kingman A, Little W, Gomez I, et al. JADA 1998;129:585-91.
43. Harwick JL, Teasdale J, Bloodworth G. Salivary levels of Streptococcus mutans and 70. Featherstone JD, Barrett-Vespone NA,
Caries increments over 4 years in children lactobacilli and dental caries experiences in a Fried D, Kantorowitz Z, Seka W. CO2 laser
aged 12 at the start of water fluroridation. Br U.S. adolescent population. Community Dent inhibitor of artificial caries-like lesion pro-
Dent J 1982;153:217-22. Oral Epidemiol 1988;16(2):98-103. gression in dental enamel. J Dent Res 1998;
44. Kobayashi S, Kawasaki K, Takagi O, et 57. Wright JT, Cutter GR, Dasanayake AP, 77(6):1397-403.
al. Caries experience in subjects 18-22 years Stiles HM, Caufield PW. Effect of convention- 71. Featherstone JD. Innovative methods
of age after 13 years’ discontinued water al dental restorative treatment on bacteria in for early caries intervention. In: Stookey GK,
fluoridation in Okinawa. Community Dent saliva. Community Dent Oral Epidemiol ed. Early detection of dental caries II: 1999.
Oral Epidemiol 1992;20:81-3. 1992;20(3):138-43. Indianapolis: Indiana University School of
45. ten Cate JM, Mundorff-Shrestha SA. 58. Anderson MH, Bales DJ, Omnell KA. Dentistry (in press).
Working group report: laboratory models for Modern management of dental caries: the 72. Fried D, Murray MW, Featherstone JD,
caries (in vitro and animal models). Adv Dent cutting edge is not the dental bur. JADA et al. Dental hard tissue modification and
Res 1995;9:332-4. 1993;124(6):37-44. removal using sealed TEA lasers operating at
46. Zero DT. In situ caries models. Adv 59. Anusavice KJ. Treatment regimens in λ = 9.6 and 10.6 µm. Proceedings of Lasers in
Dent Res 1995;9:214-30. preventive and restorative dentistry. JADA Dentistry V: Jan. 24-25, 1999, San Jose,
47. Featherstone JD, Zero DT. Laboratory 1995;126(6):727-43. Calif. Bellingham, Wash.: SPIE Press;
and human studies to elucidate the mecha- 60. Anusavice KJ. Efficacy of nonsurgical 1999:196-203.
nism of action of fluoride-containing denti- management of the initial caries lesion. J
JADA, Vol. 131, July 2000 899
Copyright ©1998-2001 American Dental Association. All rights reserved.
You might also like
- The Ultimate Nikon SLR Handbook Vol 3Document19 pagesThe Ultimate Nikon SLR Handbook Vol 3Katie Freeman50% (4)
- Theory of Knowledge - Key Concepts - Marija Uzunova Dang and Arvin Singh Uzunov Dang - Oxford 2020Document15 pagesTheory of Knowledge - Key Concepts - Marija Uzunova Dang and Arvin Singh Uzunov Dang - Oxford 2020Rex Wong50% (2)
- An Updated Review of Hypertensive Emergencies and Urgencies: Katalin Makó, Corina Ureche, Zsuzsanna JeremiásDocument11 pagesAn Updated Review of Hypertensive Emergencies and Urgencies: Katalin Makó, Corina Ureche, Zsuzsanna JeremiásiganuryantiNo ratings yet
- Integral Mechanical Attachment A Resurgence of The Oldest Method of JoiningDocument427 pagesIntegral Mechanical Attachment A Resurgence of The Oldest Method of JoiningGabriel LópezNo ratings yet
- Spring Suspension Physics FrequencyDocument2 pagesSpring Suspension Physics Frequencygkovacsds100% (1)
- Diploma in Cyber Security - Data Communication and NetworkingDocument57 pagesDiploma in Cyber Security - Data Communication and Networkingsrikant.singh62583No ratings yet
- The Glossary of Prosthodontic Terms 2005 (GPT 8°)Document83 pagesThe Glossary of Prosthodontic Terms 2005 (GPT 8°)pedrali7150% (2)
- The Glossary of Prosthodontic Terms 2005 (GPT 8°)Document83 pagesThe Glossary of Prosthodontic Terms 2005 (GPT 8°)pedrali7150% (2)
- Packaging Approval Form 1121ADocument8 pagesPackaging Approval Form 1121ASudhaNo ratings yet
- IE 337 Metal Casting Processes & TerminologyDocument48 pagesIE 337 Metal Casting Processes & TerminologylinkinunNo ratings yet
- 10 14219@jada Archive 2000 0394Document7 pages10 14219@jada Archive 2000 0394DavidNo ratings yet
- Maxillary Midline Diastemas - A Look at The CausesDocument10 pagesMaxillary Midline Diastemas - A Look at The CausesIrene Pérez MartínezNo ratings yet
- Myths of Dental Surgery in Patients Receiving Anticoagulant PDFDocument6 pagesMyths of Dental Surgery in Patients Receiving Anticoagulant PDFAlexandra MartinezNo ratings yet
- Assessing Dentin Color Changes From Nightguard Vital Bleaching McCaslin, JADA 1999Document6 pagesAssessing Dentin Color Changes From Nightguard Vital Bleaching McCaslin, JADA 1999EugenioNo ratings yet
- Treating Obstructive Sleep Apnea and Snoring: Assessment of An Anterior Mandibular Positioning DeviceDocument7 pagesTreating Obstructive Sleep Apnea and Snoring: Assessment of An Anterior Mandibular Positioning Device陈延珑No ratings yet
- Senestraro 2013Document10 pagesSenestraro 2013Silvina EscobarNo ratings yet
- Jada Archive 2008 0160Document11 pagesJada Archive 2008 0160Indah PermatasariNo ratings yet
- Creating Videos With Confidence WorkbookDocument29 pagesCreating Videos With Confidence Workbookvero baudensNo ratings yet
- Dental Disease Prevalence Among Methamphetamine and Heroin Users in An Urban SettingDocument10 pagesDental Disease Prevalence Among Methamphetamine and Heroin Users in An Urban SettingNancy Amelia RosaNo ratings yet
- Campodonico 2011Document8 pagesCampodonico 2011patel keralNo ratings yet
- Cuest DiscriminaiónJADA2010Document9 pagesCuest DiscriminaiónJADA2010Miguel Walter Ramón NeyraNo ratings yet
- CPCHILD English Parent 5.0 WatermarkedDocument9 pagesCPCHILD English Parent 5.0 WatermarkedAz-Zahraa NaasNo ratings yet
- Procedimientos y Cirugía en ORL ZurdosDocument1 pageProcedimientos y Cirugía en ORL ZurdosMarco Antonio FigueroaNo ratings yet
- Annual Implementationplan Schoolyear 2021: 0% Drop Out RateDocument6 pagesAnnual Implementationplan Schoolyear 2021: 0% Drop Out RateRaymond TumaponNo ratings yet
- Wms Gold 2017 FinalDocument139 pagesWms Gold 2017 FinalJeja JaraweeNo ratings yet
- Standards of Internal ControlsDocument71 pagesStandards of Internal Controlsnga8vu-2No ratings yet
- Bruxismo e Fratura VerticalDocument8 pagesBruxismo e Fratura VerticalCaioSelaimenNo ratings yet
- SC 9Document12 pagesSC 9khamilatusyNo ratings yet
- 2017 GINA Report, Global Strategy For Asthma Management and Prevention PDFDocument159 pages2017 GINA Report, Global Strategy For Asthma Management and Prevention PDFNalemi JT100% (1)
- Doromal, MF Moceno, EM Gervacio, C Jovita, J Cale, J Mercado, M Bugas, E Amistad, ZDocument27 pagesDoromal, MF Moceno, EM Gervacio, C Jovita, J Cale, J Mercado, M Bugas, E Amistad, ZJesnefa JovitaNo ratings yet
- Esthetics and Smile Characteristics From The Layperson's PerspectiveDocument10 pagesEsthetics and Smile Characteristics From The Layperson's PerspectivegeraldineNo ratings yet
- Wms Gold 2017 FinalDocument139 pagesWms Gold 2017 Finalapi-366968894No ratings yet
- Cross Section STA.22+560 CS/ 4 OF 12: Republica Democratica de Timor LesteDocument1 pageCross Section STA.22+560 CS/ 4 OF 12: Republica Democratica de Timor Leste4jhe Di4sNo ratings yet
- 7 Caves 22+500-22+700 RW - 1Document1 page7 Caves 22+500-22+700 RW - 14jhe Di4sNo ratings yet
- Cross Section STA.22+540 CS/ 3 OF 12: Republica Democratica de Timor LesteDocument1 pageCross Section STA.22+540 CS/ 3 OF 12: Republica Democratica de Timor Leste4jhe Di4sNo ratings yet
- 7 Caves 22+500 - PLAN & PROFILE 1Document1 page7 Caves 22+500 - PLAN & PROFILE 14jhe Di4sNo ratings yet
- U SAFE-Presentation_13.04.2023Document20 pagesU SAFE-Presentation_13.04.2023yance.hereNo ratings yet
- AYL Audience Insight InfographicDocument1 pageAYL Audience Insight InfographicAmbaNo ratings yet
- Book International Financial ManagementDocument201 pagesBook International Financial ManagementasadNo ratings yet
- Do Well 2007Document7 pagesDo Well 2007Nguyen Phuong HangNo ratings yet
- The Use of Dental Radiographs: Update and RecommendationsDocument9 pagesThe Use of Dental Radiographs: Update and RecommendationsAudry ArifinNo ratings yet
- Financial Forecasts and Determination of Financial Feasibility BTLED STUDDocument23 pagesFinancial Forecasts and Determination of Financial Feasibility BTLED STUDjared catanguiNo ratings yet
- Religion of Ancient EgyptDocument3 pagesReligion of Ancient EgyptDania UsmamNo ratings yet
- Anime AshDocument7 pagesAnime Ashsureshparekh023No ratings yet
- Coursera R8734DY5S3E6Document1 pageCoursera R8734DY5S3E6crisandra062683No ratings yet
- IMPACT SOLAR LIMITED 45th Floor, The Offices at Central World 999/9 Rama 1 Road, Patumwan, Bangkok 10330, ThailandDocument1 pageIMPACT SOLAR LIMITED 45th Floor, The Offices at Central World 999/9 Rama 1 Road, Patumwan, Bangkok 10330, ThailandTashin WongprasertsiriNo ratings yet
- CONJUNTODocument1 pageCONJUNTOAbigail RuízNo ratings yet
- October The Following Resources Related To This Article Are AvailableDocument10 pagesOctober The Following Resources Related To This Article Are Availableorthodonticlit orthodonticlitNo ratings yet
- Technical Support Fundamentals - Google - Coursera: November 2020Document2 pagesTechnical Support Fundamentals - Google - Coursera: November 2020Jayakrishna IJNo ratings yet
- A Review of The Diagnosis and Management of Impacted Maxillary CaninesDocument11 pagesA Review of The Diagnosis and Management of Impacted Maxillary CaninesSankurnia HariwijayadiNo ratings yet
- Coursera Computer Network Certificate Cse 307 PDFDocument1 pageCoursera Computer Network Certificate Cse 307 PDFstacyNo ratings yet
- Peter Paul CatalogDocument112 pagesPeter Paul Catalogcristian cendejasNo ratings yet
- Chapter 2Document41 pagesChapter 2Wardina SaffiyaNo ratings yet
- Generic Medicinre: Generic Medicine Generic Medicine Generic Medicine Generic MedicineDocument5 pagesGeneric Medicinre: Generic Medicine Generic Medicine Generic Medicine Generic MedicineganeshNo ratings yet
- Graphics MayureshDocument2 pagesGraphics Mayureshsunitaraje16No ratings yet
- Faculty of Engineering, Technology Applied Design and Fine ArtDocument48 pagesFaculty of Engineering, Technology Applied Design and Fine Artmuhammedssebatindira3No ratings yet
- Wms GINA 2018 Strategy Report V1.1 PDFDocument161 pagesWms GINA 2018 Strategy Report V1.1 PDFEdson ArmandoNo ratings yet
- Technical Support Fundamentals - Google - Coursera: November 2020Document2 pagesTechnical Support Fundamentals - Google - Coursera: November 2020Chep27 CelltriNo ratings yet
- Cavallaro2011 REPORTE DE IMPLANTE ANGULADODocument9 pagesCavallaro2011 REPORTE DE IMPLANTE ANGULADOXiomara Reyes palominoNo ratings yet
- Coursera Drug Developement PDFDocument1 pageCoursera Drug Developement PDFVasilis TsinterisNo ratings yet
- Genin 2017Document8 pagesGenin 2017BetoNo ratings yet
- Canine Protected OccDocument6 pagesCanine Protected OccDariana JDNo ratings yet
- Diagnostic Terms For Pulp Conditions - JoE 2009Document13 pagesDiagnostic Terms For Pulp Conditions - JoE 2009Bicho Angel LisseaNo ratings yet
- Anesthesia For Off-Floor Dental and Oral Surgery: ReviewDocument7 pagesAnesthesia For Off-Floor Dental and Oral Surgery: ReviewDariana JDNo ratings yet
- AAE Consensus Conference Recommended Diagnostic TerminologyDocument1 pageAAE Consensus Conference Recommended Diagnostic TerminologyAlice Isabella Torres ReyesNo ratings yet
- Anesthesia For Off-Floor Dental and Oral Surgery: ReviewDocument7 pagesAnesthesia For Off-Floor Dental and Oral Surgery: ReviewDariana JDNo ratings yet
- AAE Consensus Conference Recommended Diagnostic TerminologyDocument1 pageAAE Consensus Conference Recommended Diagnostic TerminologyAlice Isabella Torres ReyesNo ratings yet
- AAE Consensus Conference Recommended Diagnostic TerminologyDocument1 pageAAE Consensus Conference Recommended Diagnostic TerminologyAlice Isabella Torres ReyesNo ratings yet
- Course Assignment: Language Analysis and Language Learning 681 Assignment 1Document11 pagesCourse Assignment: Language Analysis and Language Learning 681 Assignment 1Đinh Lan KhánhNo ratings yet
- Multi Answer Multiple Choice QuestionsDocument1 pageMulti Answer Multiple Choice Questionsrakibdx001No ratings yet
- GL Poseidon User ManualDocument256 pagesGL Poseidon User ManualIrina MaltopolNo ratings yet
- Behavior of RC Shallow and Deep Beams WiDocument26 pagesBehavior of RC Shallow and Deep Beams WiSebastião SimãoNo ratings yet
- 4EA1 01R Que 20180606Document20 pages4EA1 01R Que 20180606Shriyans GadnisNo ratings yet
- 2 - Class UnpackingDocument22 pages2 - Class UnpackingPhuong Linh ToNo ratings yet
- Alayo, M. Internationalization and Entrepreneurial Orientation of Family SMEs The Influence of The Family CharacterArticle 2019Document12 pagesAlayo, M. Internationalization and Entrepreneurial Orientation of Family SMEs The Influence of The Family CharacterArticle 2019Riezz MauladiNo ratings yet
- Ang Pang - Ukol-WPS OfficeDocument18 pagesAng Pang - Ukol-WPS OfficeRiza Manalo LorenzoNo ratings yet
- BBC Learning English 6 Minute English Day-Trip With A DifferenceDocument4 pagesBBC Learning English 6 Minute English Day-Trip With A DifferenceAsefeh KianiNo ratings yet
- Eco Industrial DevelopmentDocument16 pagesEco Industrial DevelopmentSrinivas ThimmaiahNo ratings yet
- TSO C69bDocument28 pagesTSO C69btotololo78No ratings yet
- Lecture 1 (Production, Trade, Losses, & Causes)Document12 pagesLecture 1 (Production, Trade, Losses, & Causes)Ana Mae AquinoNo ratings yet
- Tutorial HMM CIDocument14 pagesTutorial HMM CITrương Tiểu PhàmNo ratings yet
- Klein After BachelardDocument13 pagesKlein After Bachelardyupengw122No ratings yet
- CCR Control System Interface Handbook - 6jun2012Document17 pagesCCR Control System Interface Handbook - 6jun2012Tomuta StefanNo ratings yet
- First Principle Applications in RoRo-Ship Design PDFDocument7 pagesFirst Principle Applications in RoRo-Ship Design PDFFerdy Fer DNo ratings yet
- Project Plan For Implementation of ISO 20000 20000academy ENDocument7 pagesProject Plan For Implementation of ISO 20000 20000academy ENit20645984 Imashi H.M.G.G.M.No ratings yet
- VI. 07. Synchronous Machine PDFDocument16 pagesVI. 07. Synchronous Machine PDFDesi HertianiNo ratings yet
- Factors Affecting Online Grocery Shopping Experience: Dhinda Siti Mustikasari, Rifelly Dewi AstutiDocument7 pagesFactors Affecting Online Grocery Shopping Experience: Dhinda Siti Mustikasari, Rifelly Dewi AstutiSiddharth Singh TomarNo ratings yet
- Autotrol PerformaLOGIX 740 760 ManualDocument68 pagesAutotrol PerformaLOGIX 740 760 ManualHyacinthe KOSSINo ratings yet
- Pure ChangelogDocument42 pagesPure ChangelogarmandytNo ratings yet
- Self Healing ConcreteDocument20 pagesSelf Healing ConcreteshivangNo ratings yet
- MCE 244 Course OutlineDocument1 pageMCE 244 Course OutlineKaren DavisNo ratings yet
- 1976 Murphy Psychiatric Labeling in Cross-Cultural PerspectiveDocument10 pages1976 Murphy Psychiatric Labeling in Cross-Cultural Perspectiveana stegaruNo ratings yet
- List of Technical Documents: IRB Paint Robots TR-500 / TR-5000Document16 pagesList of Technical Documents: IRB Paint Robots TR-500 / TR-5000Weberth TeixeiraNo ratings yet