You might also like
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Biochemic TissueDocument28 pagesBiochemic TissueAzad Ansari100% (2)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Orthostatic HypotensionDocument9 pagesOrthostatic HypotensionأحمدالشحاتNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Qbase MCQs For The Part B MRCPCHDocument8 pagesQbase MCQs For The Part B MRCPCHMateen ShukriNo ratings yet
- Acupressure Points To Stay FitDocument6 pagesAcupressure Points To Stay FitWafaa Abdel AzizNo ratings yet
- 50 One Liners - Neet PG PDFDocument3 pages50 One Liners - Neet PG PDFNivya Mary0% (1)
- E-Book BOPTDocument38 pagesE-Book BOPTMalina PetcuNo ratings yet
- Body Systems NotesDocument2 pagesBody Systems NotesAndrea González MercadoNo ratings yet
- Hosneara Begum - Herceptin 600mg InvoicesDocument5 pagesHosneara Begum - Herceptin 600mg InvoicesAbul HasnatNo ratings yet
- Health AssessmentDocument4 pagesHealth AssessmentKristine AcasioNo ratings yet
- Sample of Med CertDocument1 pageSample of Med CertRegineDagumanFuellasNo ratings yet
- Practical Use of The MDS-UPDRS EditDocument56 pagesPractical Use of The MDS-UPDRS EditSafitri MuhlisaNo ratings yet
- Jurnal Critical Patient MonitoringDocument10 pagesJurnal Critical Patient MonitoringKhiyarotul laeli100% (1)
- Midterm Micro-2 Virology Lesson-2Document3 pagesMidterm Micro-2 Virology Lesson-2MYLENE POSTREMONo ratings yet
- Labreportnew - 2022-12-17T172351.750Document1 pageLabreportnew - 2022-12-17T172351.750Himanshu MaheshwariNo ratings yet
- Ecg Kiss 2022 HandoutDocument3 pagesEcg Kiss 2022 HandoutCiara EnriquezNo ratings yet
- Supply Disruption AlertDocument5 pagesSupply Disruption AlertM Teresa LeivaNo ratings yet
- FibroscanDocument2 pagesFibroscanpaulica1985No ratings yet
- Sy 52 ZoologyDocument5 pagesSy 52 ZoologySajeev S Chadayamangalam SajNo ratings yet
- Oral Manifestations of Chronic Kidney Disease-An OverviewDocument4 pagesOral Manifestations of Chronic Kidney Disease-An OverviewrinakartikaNo ratings yet
- Histology of Lower GITDocument27 pagesHistology of Lower GITArwa100% (2)
- Spanish Flu: 1918 Flu Pandemic or La Pesadilla (Spanish For "TheDocument28 pagesSpanish Flu: 1918 Flu Pandemic or La Pesadilla (Spanish For "TheFaithNo ratings yet
- Acute Renal Failure: Vimar A. Luz, MD, FPCP, DPSNDocument32 pagesAcute Renal Failure: Vimar A. Luz, MD, FPCP, DPSNHemanath SinnathambyNo ratings yet
- The Cell Cycle and Cancer 2011Document28 pagesThe Cell Cycle and Cancer 2011Rajesh BalakrishnanNo ratings yet
- Medical OncologyDocument41 pagesMedical Oncologylavadey2No ratings yet
- ThyroidectomyDocument11 pagesThyroidectomySherina W. EddingNo ratings yet
- Antipsychotic Drugs in EpilepsyDocument5 pagesAntipsychotic Drugs in EpilepsyAttaufiq IrawanNo ratings yet
- 5 02 Acute Abdominal PainDocument17 pages5 02 Acute Abdominal PainNereida LechugaNo ratings yet
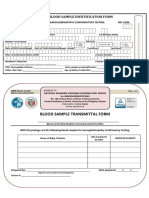
- HEM-FO-01&02, Rev.02 - ID FormsDocument1 pageHEM-FO-01&02, Rev.02 - ID FormsHazelle karren ManabatNo ratings yet
- Icp MonitoringDocument6 pagesIcp Monitoringfarhanfarwani familyNo ratings yet
- Amphotericin B: Component Mg/liter Mol. Wt. Mol. (MM)Document7 pagesAmphotericin B: Component Mg/liter Mol. Wt. Mol. (MM)Echa Alifyanty SyarifNo ratings yet