You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Risk Assessment Form: Zibran Anwar SayyadDocument2 pagesRisk Assessment Form: Zibran Anwar SayyadMufid SatamkarNo ratings yet
- Insertion of An Intra-Aortic Balloon Catheter: PurposeDocument4 pagesInsertion of An Intra-Aortic Balloon Catheter: PurposeGloria KartikaNo ratings yet
- Contoh Surat SponsorDocument1 pageContoh Surat SponsorGloria KartikaNo ratings yet
- Survival Analysis, Part 3: Cox Regression: Statistics and Research DesignDocument2 pagesSurvival Analysis, Part 3: Cox Regression: Statistics and Research DesignGloria KartikaNo ratings yet
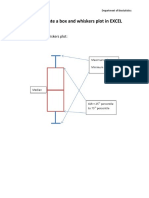
- How To Create A Box and Whiskers Plot in EXCELDocument9 pagesHow To Create A Box and Whiskers Plot in EXCELGloria KartikaNo ratings yet
- MC GowanDocument13 pagesMC GowanGloria KartikaNo ratings yet
- Cardiology Board Review - Carlquist - PT. 1 PDFDocument40 pagesCardiology Board Review - Carlquist - PT. 1 PDFGloria KartikaNo ratings yet
- CLN 66 01 107 PDFDocument5 pagesCLN 66 01 107 PDFGloria KartikaNo ratings yet
- QTinterval Changes During The Management of DHFDocument7 pagesQTinterval Changes During The Management of DHFGloria KartikaNo ratings yet
- Prevalensi Ventricular HypertrophyDocument8 pagesPrevalensi Ventricular HypertrophyGloria KartikaNo ratings yet
- 24 Newsletter Hypertension and ArrhythmiaDocument2 pages24 Newsletter Hypertension and ArrhythmiaGloria KartikaNo ratings yet
- WHO LadderDocument2 pagesWHO LaddertelorkodokNo ratings yet
- 6.21.10 Rose-Jones Board ReviewDocument50 pages6.21.10 Rose-Jones Board ReviewGloria KartikaNo ratings yet
- Clinical Management 07Document22 pagesClinical Management 07Fauzi SatriaNo ratings yet
- Vision2020 ReportDocument97 pagesVision2020 ReportAdelaida Castro NavarreteNo ratings yet
- WHO Blindness Action An 2014-2019Document28 pagesWHO Blindness Action An 2014-2019Gloria KartikaNo ratings yet
- Staining and Tooth DiscolorationDocument14 pagesStaining and Tooth DiscolorationGloria KartikaNo ratings yet
- Kuliah: Renjatan Hipovolemi Pada Anak (Hypovolemic Shock in Children)Document17 pagesKuliah: Renjatan Hipovolemi Pada Anak (Hypovolemic Shock in Children)DillaNo ratings yet
- WHO Clinical Management 0f Avian InfluenzaDocument83 pagesWHO Clinical Management 0f Avian InfluenzaGloria KartikaNo ratings yet
- Degeneratif Copy 2Document7 pagesDegeneratif Copy 2Gloria KartikaNo ratings yet
- CH 06Document11 pagesCH 06kavitasibalNo ratings yet
- Infeksi Marginalis NadaDocument48 pagesInfeksi Marginalis NadaGloria KartikaNo ratings yet
- Hypertension: H.) or May Be Associated With Other Diseases - Dorland'sDocument1 pageHypertension: H.) or May Be Associated With Other Diseases - Dorland'sGloria KartikaNo ratings yet
- Kuliah: Renjatan Hipovolemi Pada Anak (Hypovolemic Shock in Children)Document17 pagesKuliah: Renjatan Hipovolemi Pada Anak (Hypovolemic Shock in Children)DillaNo ratings yet
- European Psychiatry: Emma Kinnaird, Catherine Stewart, Kate TchanturiaDocument10 pagesEuropean Psychiatry: Emma Kinnaird, Catherine Stewart, Kate TchanturiaJenderal BesarNo ratings yet
- 2019 Nclex RN Cram SheetDocument7 pages2019 Nclex RN Cram Sheetpjhay93% (82)
- Pathcare Labs Antenatal Test ReportDocument8 pagesPathcare Labs Antenatal Test ReportTrilok TripathiNo ratings yet
- Pearls in Medicine For Students PDFDocument303 pagesPearls in Medicine For Students PDFGabriela Cordova Goicochea100% (2)
- Drug StudyDocument2 pagesDrug Studykev mondaNo ratings yet
- Knowledge and Hygiene Practice of Prisoners Towards Dermatophytosis - A Study in Nakkhu Prison, NepalDocument15 pagesKnowledge and Hygiene Practice of Prisoners Towards Dermatophytosis - A Study in Nakkhu Prison, Nepalbibek karkiNo ratings yet
- Dermatitis and HomoeopathyDocument18 pagesDermatitis and HomoeopathyDr. Rajneesh Kumar Sharma MD Hom100% (1)
- Leukemia in Children: 1 Rahul Dhaker, Asst. Professor, RCNDocument41 pagesLeukemia in Children: 1 Rahul Dhaker, Asst. Professor, RCNRahul DhakerNo ratings yet
- COVID-19 MRNA Vaccine MRNA-1273 ModernaDocument4 pagesCOVID-19 MRNA Vaccine MRNA-1273 ModernawalkrogNo ratings yet
- The Early Identification of Autism: The Checklist For Autism in Toddlers (CHAT)Document43 pagesThe Early Identification of Autism: The Checklist For Autism in Toddlers (CHAT)melaniNo ratings yet
- Manajemen Asuhan Kebidanan Pada Ibu Hamil Dengan Hiperemesis Gravidarum Tingkat IDocument8 pagesManajemen Asuhan Kebidanan Pada Ibu Hamil Dengan Hiperemesis Gravidarum Tingkat IErni ChanNo ratings yet
- Hiv PresentationDocument10 pagesHiv Presentationapi-534814911No ratings yet
- COVID-19: Dr. Moe Yee Soe Assistant Lecturer Department of Microbiology UM1Document42 pagesCOVID-19: Dr. Moe Yee Soe Assistant Lecturer Department of Microbiology UM1Naing Lin SoeNo ratings yet
- Basic Pharmacology: NTA Level 4 Semester 2Document16 pagesBasic Pharmacology: NTA Level 4 Semester 2MabusiNo ratings yet
- Allied Health ProfessionalsDocument19 pagesAllied Health ProfessionalsReihnard RosariioNo ratings yet
- Pedh ExamDocument12 pagesPedh ExamJames100% (2)
- Critical Values List: Arterial Blood GasesDocument3 pagesCritical Values List: Arterial Blood Gasesiq_dianaNo ratings yet
- Welcome To The Morning SessionDocument20 pagesWelcome To The Morning SessionGENERAL sharpNo ratings yet
- Internal DiseaseDocument55 pagesInternal Diseaseshilpa sekhar278No ratings yet
- The Prevalence of Stroke and Associated DisabilityDocument6 pagesThe Prevalence of Stroke and Associated DisabilityRaymond LinatocNo ratings yet
- Anesthesia For Patients With Diabetes Mellitus - UpToDateDocument31 pagesAnesthesia For Patients With Diabetes Mellitus - UpToDateEduardoNo ratings yet
- Statistical Analysis On Risk Factors of Prevalence of Malaria in Z/ Dugda Woreda, Oromia, East ArsiDocument31 pagesStatistical Analysis On Risk Factors of Prevalence of Malaria in Z/ Dugda Woreda, Oromia, East Arsitewodrosmolalign19No ratings yet
- Case Presentation Non-Hodgkin's LymphomaDocument13 pagesCase Presentation Non-Hodgkin's LymphomaMau Gallevo100% (4)
- User Manual: (High Intensity Focused Ultrasound)Document11 pagesUser Manual: (High Intensity Focused Ultrasound)Agha SoroushNo ratings yet
- Laws in HealthDocument1 pageLaws in Healthrouya100% (3)
- Utilizing Battling Rope Exercises For HIIT and SMITDocument50 pagesUtilizing Battling Rope Exercises For HIIT and SMITJaydaa Kamel EL ArabyNo ratings yet
- Personality DisordersDocument125 pagesPersonality DisordersDevendra Singh Baryah100% (2)
- Professional-grade dermatoscope for early skin cancer detectionDocument2 pagesProfessional-grade dermatoscope for early skin cancer detectionHemkerovner Keresztszegh von Kolowrat-KrakowskyNo ratings yet
- Skin CancerDocument24 pagesSkin CancerMister David anthonyNo ratings yet