You might also like
- Mental Health ResourceDocument130 pagesMental Health ResourceBernardo Linares50% (2)
- Gad-7 Questionnaire SpanishDocument86 pagesGad-7 Questionnaire Spanishrowanpurdy100% (1)
- Good Housekeeping - Easy KetoDocument98 pagesGood Housekeeping - Easy KetoStefan HNo ratings yet
- Eng PDFDocument447 pagesEng PDFPuteri AyuNo ratings yet
- Public Health Nursing: Scope and Standards of PracticeFrom EverandPublic Health Nursing: Scope and Standards of PracticeRating: 5 out of 5 stars5/5 (1)
- Importance of VegetablesDocument9 pagesImportance of VegetablesRitwik Thakur100% (1)
- Science 8 Summative Exam Q4Document4 pagesScience 8 Summative Exam Q4Kelvin Jason ArellanoNo ratings yet
- Community Health NursingDocument7 pagesCommunity Health NursingRosafe E. PeraltaNo ratings yet
- Case Investing Public HealthDocument40 pagesCase Investing Public Healthabbas salihiNo ratings yet
- COMMUNITY HEALTH NURSING (Continuation)Document18 pagesCOMMUNITY HEALTH NURSING (Continuation)Angel Joy Catalan100% (2)
- The Science of Wellness Programs: A SynopsisDocument53 pagesThe Science of Wellness Programs: A SynopsisPartnership to Fight Chronic Disease100% (1)
- The Health Care Delivery SystemDocument34 pagesThe Health Care Delivery SystemFritzie Buquiron67% (3)
- Safe and Clean Care: Infection Prevention and Control for Health and Social Care StudentsFrom EverandSafe and Clean Care: Infection Prevention and Control for Health and Social Care StudentsNo ratings yet
- Functions of Public HealthDocument30 pagesFunctions of Public Healthteklay100% (1)
- Revised BSC Nursing SyllabusDocument218 pagesRevised BSC Nursing SyllabusManjunatha HR86% (7)
- Iec SemininarDocument27 pagesIec SemininarRavina Patel100% (1)
- Curriculum in NursingDocument53 pagesCurriculum in NursingsakshiwiproNo ratings yet
- NRSG 780 - Health Promotion and Population Health: Module 8: Program Planning Essentials and ModelsDocument12 pagesNRSG 780 - Health Promotion and Population Health: Module 8: Program Planning Essentials and ModelsjustdoyourNo ratings yet
- Health Promotion Evaluation: Recommendations To Policy-MakersDocument12 pagesHealth Promotion Evaluation: Recommendations To Policy-MakersEdgar MirandaNo ratings yet
- Sol 743.urgentDocument4 pagesSol 743.urgentUjjwal MaharjanNo ratings yet
- Improving Health and Reducing Inequalities A Practical Guide To HIA - WAG Wales - 2004Document36 pagesImproving Health and Reducing Inequalities A Practical Guide To HIA - WAG Wales - 2004PublicHealthbyDesignNo ratings yet
- What Are The Main Factors That Influence The Implementation of Disease Prevention and Health Promotion Programmes in Children and Adolescents?Document18 pagesWhat Are The Main Factors That Influence The Implementation of Disease Prevention and Health Promotion Programmes in Children and Adolescents?HarjotBrarNo ratings yet
- Assessment of Population Health Risks of Policies: Gabriel Guliš Odile Mekel Balázs Ádám Liliana Cori EditorsDocument282 pagesAssessment of Population Health Risks of Policies: Gabriel Guliš Odile Mekel Balázs Ádám Liliana Cori EditorsRenata BrudascaNo ratings yet
- Report of Knowledge and Use of A Nutrition Care ProcessDocument36 pagesReport of Knowledge and Use of A Nutrition Care ProcessSalsabila WindarjatNo ratings yet
- SGPP Bestpracticescriteria en 0Document11 pagesSGPP Bestpracticescriteria en 0testNo ratings yet
- Health Systems Health Wealth and Societal Well-Being A Triangular RelationshipDocument80 pagesHealth Systems Health Wealth and Societal Well-Being A Triangular RelationshipMaria Belen Coca MogroNo ratings yet
- Promoting Health Preventing Disease: Is There An Economic Case?Document84 pagesPromoting Health Preventing Disease: Is There An Economic Case?johnsonkk125No ratings yet
- Marsh Farm Central Area Regeneration Masterplanning HIA SummaryDocument42 pagesMarsh Farm Central Area Regeneration Masterplanning HIA SummarySalim VohraNo ratings yet
- Public Health Future EngDocument19 pagesPublic Health Future EngKiros Tilahun BentiNo ratings yet
- Primary Health Care 2007 enDocument42 pagesPrimary Health Care 2007 enAC GanadoNo ratings yet
- Defining Societal Health Needs: Royal College Definition and GuideDocument12 pagesDefining Societal Health Needs: Royal College Definition and Guidejairo silveiraNo ratings yet
- Job Responsibilities of Health Education OfficersDocument6 pagesJob Responsibilities of Health Education OfficersKailash NagarNo ratings yet
- Monev WHO 1Document12 pagesMonev WHO 1MhilaaNo ratings yet
- How Can Health Systems Respond To Population Ageing?: Bernd Rechel, Yvonne Doyle, Emily Grundy, Martin MckeeDocument43 pagesHow Can Health Systems Respond To Population Ageing?: Bernd Rechel, Yvonne Doyle, Emily Grundy, Martin MckeeYantoNo ratings yet
- Review of Social Determinants and The Health Divide in The WHO European RegionDocument234 pagesReview of Social Determinants and The Health Divide in The WHO European RegionAdrian ArizmendiNo ratings yet
- Sister Blessing Project.Document41 pagesSister Blessing Project.ayanfeNo ratings yet
- Community Health Nursing ModelsDocument20 pagesCommunity Health Nursing ModelsRamzen Raphael DomingoNo ratings yet
- Module Health10 Q4 W8Document6 pagesModule Health10 Q4 W8Rosa Mia MarzanNo ratings yet
- Constructing A General Competency Model For Chinese Public Health Physicians: A Qualitative and Quantitative StudyDocument7 pagesConstructing A General Competency Model For Chinese Public Health Physicians: A Qualitative and Quantitative StudyClumsyNo ratings yet
- FPH PH Practitioner 09 20-v2Document8 pagesFPH PH Practitioner 09 20-v2Tim ChifNo ratings yet
- 3-MeasuringOralHealth-HowCanThe ICF HelpDocument30 pages3-MeasuringOralHealth-HowCanThe ICF HelppepeNo ratings yet
- Mid Exam For Nursery EnglishDocument8 pagesMid Exam For Nursery EnglishYunisNo ratings yet
- Principles of Public Health: Dr. Shagufta ShahjahanDocument16 pagesPrinciples of Public Health: Dr. Shagufta ShahjahanAmar Wadood KhanNo ratings yet
- Research Methods & Reporting: Consolidated Health Economic Evaluation Reporting Standards (CHEERS) StatementDocument6 pagesResearch Methods & Reporting: Consolidated Health Economic Evaluation Reporting Standards (CHEERS) StatementMuhammadNoorIfansyahNo ratings yet
- Jpi HDHL SraDocument64 pagesJpi HDHL SraDogDylanNo ratings yet
- Urban HEP in Ethiopia XDocument19 pagesUrban HEP in Ethiopia Xበተግባር ግዛቸውNo ratings yet
- PM Assignment 2Document20 pagesPM Assignment 2ManuNo ratings yet
- Gender Dalam Pelayanan KesehatanDocument10 pagesGender Dalam Pelayanan KesehatanIzzatul ArifahNo ratings yet
- Concept of CHNDocument34 pagesConcept of CHNACERET, IVAN LAURENTINE G.No ratings yet
- Skills Partnership For The Health Ecosystem - FinalDocument8 pagesSkills Partnership For The Health Ecosystem - FinalErNo ratings yet
- KIT Development Policy & Practice Advanced Courses 2012Document12 pagesKIT Development Policy & Practice Advanced Courses 2012sumith_sNo ratings yet
- BUTALON Assessment 1Document7 pagesBUTALON Assessment 1Kc Cassandra ButalonNo ratings yet
- MPH-Model Course CurriculumDocument24 pagesMPH-Model Course CurriculumRyan WootenNo ratings yet
- Continuing Professional Development (CPD) Guideline For Health Professionals in EthiopiaDocument35 pagesContinuing Professional Development (CPD) Guideline For Health Professionals in EthiopiaWakjira debalaNo ratings yet
- Core Competencies For Health Promotion PractitionersDocument8 pagesCore Competencies For Health Promotion PractitionersImamNo ratings yet
- Evidence Based Public Health Lecture 2Document49 pagesEvidence Based Public Health Lecture 2Queen SofiaNo ratings yet
- WP 42Document27 pagesWP 42Dr.Pradeep JNANo ratings yet
- Health Workforce IncentiveDocument44 pagesHealth Workforce IncentiveMasrun FatanahNo ratings yet
- Health and Environmental Impact AssessmentDocument18 pagesHealth and Environmental Impact AssessmentIslam FarragNo ratings yet
- Health Equity Assessment Tool Guide1Document49 pagesHealth Equity Assessment Tool Guide1Ariana TushinNo ratings yet
- Module 1: Community Health Nursing ConceptsDocument4 pagesModule 1: Community Health Nursing ConceptsAno NymousNo ratings yet
- Nursing Module 1Document26 pagesNursing Module 1louisemaemaglalangNo ratings yet
- PQCNC 2023 Nutrition in PregnancyDocument12 pagesPQCNC 2023 Nutrition in PregnancykcochranNo ratings yet
- Nursing Care Plan for Post-Surgical Bleeding RiskDocument10 pagesNursing Care Plan for Post-Surgical Bleeding RiskRyan MirandaNo ratings yet
- How To Teach Canada's Food Guide PresentationDocument18 pagesHow To Teach Canada's Food Guide PresentationSevak SinghNo ratings yet
- Digestive Tract Detoxification GI Health Depends PDFDocument20 pagesDigestive Tract Detoxification GI Health Depends PDFPablo CrespoNo ratings yet
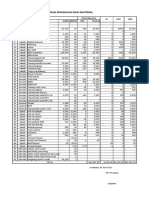
- Laporan Mingguan Raw Material: Stock Opname IN OUT Sisa Jenis Raw Material Buffer Kg/koli Koli Total KGDocument4 pagesLaporan Mingguan Raw Material: Stock Opname IN OUT Sisa Jenis Raw Material Buffer Kg/koli Koli Total KGAlfa ArnantoNo ratings yet
- 821566642727unit-2 - Nutrition and DieteticsDocument12 pages821566642727unit-2 - Nutrition and DieteticsGaganpreet Kaur Fashion DesigningNo ratings yet
- 3Q (WEEK 6 ACT 2) Principles in Preparing SoupDocument1 page3Q (WEEK 6 ACT 2) Principles in Preparing SoupJoyce Dela Rama JulianoNo ratings yet
- Hurom Juice: Recipe BookDocument17 pagesHurom Juice: Recipe BookMaraNo ratings yet
- Dozova NAD+ Vitamin Supplement Supports Healthy Aging, Energy - Sehetna-EgDocument4 pagesDozova NAD+ Vitamin Supplement Supports Healthy Aging, Energy - Sehetna-EgaliNo ratings yet
- Proposal of MulumebetDocument40 pagesProposal of MulumebetMulumebet EshetuNo ratings yet
- Life Sciences p1 Memo Gr11 Nov 2020 Eng DDocument10 pagesLife Sciences p1 Memo Gr11 Nov 2020 Eng Dmokoenakoketso018No ratings yet
- Antonia-Leda Matalas, Antonis Zampelas, Vassilis Stavrinos - The Mediterranean Diet - Constituents and Health Promotion-CRC Press (2001)Document379 pagesAntonia-Leda Matalas, Antonis Zampelas, Vassilis Stavrinos - The Mediterranean Diet - Constituents and Health Promotion-CRC Press (2001)Новковић АњаNo ratings yet
- Mushroom SoupDocument48 pagesMushroom SoupJennifer FerraoNo ratings yet
- Physicochemical Characteristics of Citrus Jelly With Non CariogenicDocument9 pagesPhysicochemical Characteristics of Citrus Jelly With Non CariogenicPrasad BhadaneNo ratings yet
- Harusdewi 2018Document7 pagesHarusdewi 2018Izzuddin AhmadNo ratings yet
- Grimble 2017 - The Physiology of Nutrient Digestion AbsorptionDocument27 pagesGrimble 2017 - The Physiology of Nutrient Digestion AbsorptionJUAN ESTEBAN CELIS QUINTERONo ratings yet
- Dissertation Topics in Food ScienceDocument7 pagesDissertation Topics in Food ScienceBuyCheapPaperOnlineEugene100% (1)
- Sports Nutrition: Trainer: Matt PargeterDocument99 pagesSports Nutrition: Trainer: Matt PargeterAnkit SharmaNo ratings yet
- Topic 6-Nutrition Education and Communication Strategies in Different Groups-1Document39 pagesTopic 6-Nutrition Education and Communication Strategies in Different Groups-1Wahab KhanNo ratings yet
- Food and Nutrition MarikaDocument21 pagesFood and Nutrition Marikammeemz360No ratings yet
- Banana starch and flour food applications reviewDocument13 pagesBanana starch and flour food applications reviewZenaw AntenbiyeNo ratings yet
- Tuscan Nutella and Meringue Tart - Juls' KitchenDocument2 pagesTuscan Nutella and Meringue Tart - Juls' KitchenMaria TurnerNo ratings yet
- Lifelong Vitality BrochureDocument24 pagesLifelong Vitality BrochureJosefina LarreateguiNo ratings yet
- 04 D.S.penaranda Research in Biofloc at University of ValenciaDocument22 pages04 D.S.penaranda Research in Biofloc at University of ValenciaMayank VaitiNo ratings yet
- Nutrition Education and CounsellingDocument31 pagesNutrition Education and CounsellingMaryam100% (1)
- Equine Colic - Causes, Symptoms, Treatment and PreventionDocument4 pagesEquine Colic - Causes, Symptoms, Treatment and PreventionasddafadNo ratings yet
- Communication and Nutrional EducationDocument11 pagesCommunication and Nutrional EducationSabrina PanjaitanNo ratings yet