You might also like
- Frank Hammond - List of DemonsDocument3 pagesFrank Hammond - List of DemonsJavico392% (84)
- Trauma-Focused ACT - Extra Bits - Russ Harris - November 2021Document6 pagesTrauma-Focused ACT - Extra Bits - Russ Harris - November 2021psiho2024No ratings yet
- Enneagram Type 7 DescriptionDocument20 pagesEnneagram Type 7 DescriptionimperiallightNo ratings yet
- The Elements of Applied Psychological Practice in ... - (6 Part I. 100 National Psychology Examination-Like Multiple-Choice Que... ) 1Document44 pagesThe Elements of Applied Psychological Practice in ... - (6 Part I. 100 National Psychology Examination-Like Multiple-Choice Que... ) 1Kaz AmosNo ratings yet
- Three Theories Commonly Cited To Explain The Origin of Anxiety DisordersDocument13 pagesThree Theories Commonly Cited To Explain The Origin of Anxiety DisordersNor-aina Edding AbubakarNo ratings yet
- Robert Greene's The 50th Law SummaryDocument5 pagesRobert Greene's The 50th Law SummaryJyoti KaleNo ratings yet
- Cavallaro - The Gothic Vision PDFDocument241 pagesCavallaro - The Gothic Vision PDFTony Alcala100% (2)
- Eating Disorders Information Sheet - 03 - Body Checking and AvoidanceDocument1 pageEating Disorders Information Sheet - 03 - Body Checking and Avoidanceletitia2hintonNo ratings yet
- Brain in The Palm of The HanDocument3 pagesBrain in The Palm of The HanIftikhar AliNo ratings yet
- Dissociative DisordersDocument17 pagesDissociative Disordersapi-3797941100% (4)
- Fred Gallo PHD and Harry VincenziEdD Energy TappingDocument203 pagesFred Gallo PHD and Harry VincenziEdD Energy Tappingthomist36100% (1)
- Thinking Errors Characteristic of The CriminalDocument4 pagesThinking Errors Characteristic of The Criminalmathoni100% (1)
- Children's Emotional Development Is Built Into The Architecture of Their BrainsDocument12 pagesChildren's Emotional Development Is Built Into The Architecture of Their BrainsChelsea Leigh Musee TrescottNo ratings yet
- The Science of NeglectDocument20 pagesThe Science of NeglectdrdrtsaiNo ratings yet
- From Perception To Action: The Role of Auditory and Visual Information in Perceiving and Performing Complex MovementsDocument239 pagesFrom Perception To Action: The Role of Auditory and Visual Information in Perceiving and Performing Complex MovementsN SchaffertNo ratings yet
- Complex Child TraumaDocument5 pagesComplex Child TraumaAdela Carolina Ruiz BravoNo ratings yet
- Manual 2day Anxiety Certification CourseDocument121 pagesManual 2day Anxiety Certification Coursemartin1978pb100% (1)
- Attention Deficit Hyperactivity Disorder: Judith Axelrod, M.D. Developmental-Behavioral PediatricianDocument49 pagesAttention Deficit Hyperactivity Disorder: Judith Axelrod, M.D. Developmental-Behavioral PediatricianKennedy CalvinNo ratings yet
- Attachment TheoryDocument4 pagesAttachment TheoryMohammedseid AhmedinNo ratings yet
- Growth and Development: Infancy Early Childhood Middle Childhood AdolescentDocument42 pagesGrowth and Development: Infancy Early Childhood Middle Childhood AdolescentJohn Ervin AgenaNo ratings yet
- Psychological Needs: Love and AffectionDocument4 pagesPsychological Needs: Love and AffectionFrancis LukeNo ratings yet
- Asperger SyndromeDocument13 pagesAsperger SyndromedrsantosguptaNo ratings yet
- Increased Sensitivity To Mirror Symmetry in AutismDocument5 pagesIncreased Sensitivity To Mirror Symmetry in AutismRadek JohnNo ratings yet
- Dyspraxia and ExaminationsDocument3 pagesDyspraxia and ExaminationsAngus KirkNo ratings yet
- What's Next? A Digital Planner For Children With AutismDocument51 pagesWhat's Next? A Digital Planner For Children With Autism'Inti MansourNo ratings yet
- Expressions of the Mind in Words: Writings by a 9 year old kidFrom EverandExpressions of the Mind in Words: Writings by a 9 year old kidNo ratings yet
- Design and Development of A Virtual Dolphinarium For Children With AutismDocument10 pagesDesign and Development of A Virtual Dolphinarium For Children With AutismAlexander JagannathanNo ratings yet
- Ot Pre-Referral Form: Intervention Strategies: Poor Posture/ Falls Out of Chair/ Slumps Significantly (All Ages)Document15 pagesOt Pre-Referral Form: Intervention Strategies: Poor Posture/ Falls Out of Chair/ Slumps Significantly (All Ages)maria vasquezNo ratings yet
- Wechsler Intelligence Scale For Children - 5 Edition (WISC-V)Document1 pageWechsler Intelligence Scale For Children - 5 Edition (WISC-V)LevanNo ratings yet
- Drawing The Ideal Self: Session PR Ompt SheetDocument5 pagesDrawing The Ideal Self: Session PR Ompt SheetTEOFILO PALSIMON JR.No ratings yet
- Trauma Informed ApproachDocument111 pagesTrauma Informed Approachalejandra sarmientoNo ratings yet
- Visual Supports GuideDocument20 pagesVisual Supports GuideKathleen EdwardsNo ratings yet
- Circles SexualityDocument1 pageCircles SexualityMaika NarcisoNo ratings yet
- Parenting and ADHD Presentation Feb 24 2021 FINALDocument67 pagesParenting and ADHD Presentation Feb 24 2021 FINALAyman ZyanNo ratings yet
- Living with Hearing Difficulties: The process of enablementFrom EverandLiving with Hearing Difficulties: The process of enablementNo ratings yet
- Anxiety ResoursesDocument1 pageAnxiety ResoursesKarla M. Febles BatistaNo ratings yet
- Designing For Young Children With Autism Spectrum DisorderDocument14 pagesDesigning For Young Children With Autism Spectrum Disorderapi-415110604No ratings yet
- PencilGraspInterventions2017 REVISEDDocument34 pagesPencilGraspInterventions2017 REVISEDmaria vasquezNo ratings yet
- FAT - Newsletter - V3N4 Normal Childhood Sexual DevelopmentDocument4 pagesFAT - Newsletter - V3N4 Normal Childhood Sexual DevelopmentJackNo ratings yet
- Communication Guide EnglishDocument8 pagesCommunication Guide Englishblen92No ratings yet
- Parenting - AsdDocument9 pagesParenting - Asdapi-391945267No ratings yet
- Concepts in Occupational Therapy in Relation To The ICFDocument16 pagesConcepts in Occupational Therapy in Relation To The ICFmarjan 01No ratings yet
- Child Dev WorkbookDocument29 pagesChild Dev WorkbookDominic Bonkers StandingNo ratings yet
- CCG Book PDFDocument235 pagesCCG Book PDFMistor Dupois WilliamsNo ratings yet
- Star Conference Feeling Buddies - Our JourneyDocument27 pagesStar Conference Feeling Buddies - Our JourneyfernandapazNo ratings yet
- Early Years Study 3 - Full ReportDocument128 pagesEarly Years Study 3 - Full Reportnick_logan9361No ratings yet
- Sensory Enrichment TherapyDocument3 pagesSensory Enrichment TherapySanjay NavaleNo ratings yet
- Guide to Young Children's Learning and Development from Birth to Kindergarten ΑΑΑΑΑΑΑDocument156 pagesGuide to Young Children's Learning and Development from Birth to Kindergarten ΑΑΑΑΑΑΑΒασίλης ΒασιλείουNo ratings yet
- Aphasia ADocument305 pagesAphasia ANinoska OrtizNo ratings yet
- Sensitive PracticeDocument122 pagesSensitive PracticeFederica FarfallaNo ratings yet
- Dokumen - Pub - Sensory Integration and Learning Disorders Hardcovernbsped 0874243033 9780874243031 - Compressed 10Document30 pagesDokumen - Pub - Sensory Integration and Learning Disorders Hardcovernbsped 0874243033 9780874243031 - Compressed 10Pablo Rodríguez HernándezNo ratings yet
- Neuro-Arts Education - The Brain and DisabilitiesDocument27 pagesNeuro-Arts Education - The Brain and DisabilitiesneuroaNo ratings yet
- PACE Behaviour Management StrategyDocument17 pagesPACE Behaviour Management StrategyRachael GoninanNo ratings yet
- Clinical GuidelineDocument86 pagesClinical GuidelineJae MedinaNo ratings yet
- Task CardsDocument7 pagesTask CardsJeni CucuNo ratings yet
- Comparison of Functional AssessmentDocument14 pagesComparison of Functional AssessmentDaniela BerceaNo ratings yet
- Brain Facts - A Primer On The Brain and Nervous System 6th Edition (Malestrom) PDFDocument80 pagesBrain Facts - A Primer On The Brain and Nervous System 6th Edition (Malestrom) PDFnumuaiNo ratings yet
- What Is Dyslexia?Document4 pagesWhat Is Dyslexia?Ashiwn PanchalNo ratings yet
- The Teenage Guide To StressDocument188 pagesThe Teenage Guide To StressMs Euphraxia100% (1)
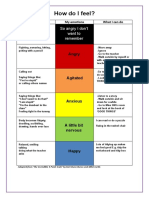
- How Do I Feel?: So Angry I Don't Want To RememberDocument2 pagesHow Do I Feel?: So Angry I Don't Want To RememberBill Mackay100% (1)
- School Refusal Assessment ScaleDocument6 pagesSchool Refusal Assessment Scaleamrut muzumdarNo ratings yet
- Talkabout Theory of Mind Teaching Theory of Mind To Improve Social Skills and Relationships by Katherine Wareham, Alex KellyDocument304 pagesTalkabout Theory of Mind Teaching Theory of Mind To Improve Social Skills and Relationships by Katherine Wareham, Alex KellyFORMALEJO, FE PATRIA F.No ratings yet
- Premonitory Urge For Tics Scale (PUTS)Document2 pagesPremonitory Urge For Tics Scale (PUTS)dnutter012576No ratings yet
- Dir - Floortime Model - Using Relationship-Based Intervention To IncDocument33 pagesDir - Floortime Model - Using Relationship-Based Intervention To IncAndreia SilvaNo ratings yet
- Echolalia ..What To Do About It: June 2, 2008 byDocument6 pagesEcholalia ..What To Do About It: June 2, 2008 byAmalia PreoteasaNo ratings yet
- CAMHS WorkbookDocument48 pagesCAMHS WorkbookMHRED_UOLNo ratings yet
- Understanding My Panic: Information HandoutDocument4 pagesUnderstanding My Panic: Information HandoutRhio Abendan100% (1)
- Connie’s Gifts- Interactive Books and Collectibles. Got Parenting Challenges? Book 1From EverandConnie’s Gifts- Interactive Books and Collectibles. Got Parenting Challenges? Book 1No ratings yet
- Arthur PaperDocument13 pagesArthur Paperハイロ ナルバエスNo ratings yet
- How To Overcome FearDocument8 pagesHow To Overcome Fearmclaren9150% (2)
- In The Wake of 911 The Psychology of TerrorDocument229 pagesIn The Wake of 911 The Psychology of TerrorDavid McGaugheyNo ratings yet
- Mental ToughnessDocument30 pagesMental Toughnessapi-3164455890% (1)
- The Most Epic Character Chart EverDocument12 pagesThe Most Epic Character Chart EverrisetoyosoapNo ratings yet
- New Horizon MagazineDocument35 pagesNew Horizon MagazinePrabhakar SastriNo ratings yet
- Training and Supervision in Specialized Cognitive Behavior2022Document447 pagesTraining and Supervision in Specialized Cognitive Behavior2022sevenqiu7777100% (1)
- Benefits of Facing Fear English ProjectDocument23 pagesBenefits of Facing Fear English ProjectXyz PqrNo ratings yet
- Welfare in Dog TrainingDocument13 pagesWelfare in Dog TrainingNicholay AtanassovNo ratings yet
- NCP Actual and PotentialDocument4 pagesNCP Actual and PotentialKristian Karl Bautista Kiw-isNo ratings yet
- Arousal and Anxiety - Boxing WebinarDocument25 pagesArousal and Anxiety - Boxing WebinarAmol PatilNo ratings yet
- Attack BehavioursDocument3 pagesAttack BehavioursKrithiga RNo ratings yet
- Literature Review On EmotionsDocument9 pagesLiterature Review On Emotionsfyh0kihiwef2100% (1)
- MfA Leadership ExperienceDocument49 pagesMfA Leadership ExperienceAlex MoralesNo ratings yet
- Human Persons As Oriented Towards Their Impendeing DeathDocument28 pagesHuman Persons As Oriented Towards Their Impendeing DeathMaxwell LaurentNo ratings yet
- Rationale and Background of The StudyDocument72 pagesRationale and Background of The StudyAzzia Morante LopezNo ratings yet
- Quizzes Questionnaires and PuzzlesDocument316 pagesQuizzes Questionnaires and PuzzlesDANIELA SIMONELLI100% (1)
- Human Behavior and VictimologyDocument78 pagesHuman Behavior and VictimologyAnnielyn IgnesNo ratings yet
- Denial of Death Chapter 5Document18 pagesDenial of Death Chapter 5RobKirkNo ratings yet
- HK AssessmentsDocument22 pagesHK Assessmentsايه مهديNo ratings yet
- Abnormal Behavior (Written Report)Document11 pagesAbnormal Behavior (Written Report)Shara Joy B. ParaynoNo ratings yet
- Abnormal Psychology Nolen Hoeksema 6th Edition Test BankDocument54 pagesAbnormal Psychology Nolen Hoeksema 6th Edition Test BankStevenRichardsdesk100% (40)