You might also like
- Etiology of Thyroid Cancer (C73) in Central and South AmericaDocument9 pagesEtiology of Thyroid Cancer (C73) in Central and South AmericaRum Afida RasfaNo ratings yet
- Papillary Thyroid CarcinomaDocument17 pagesPapillary Thyroid CarcinomaEster Sibarani100% (2)
- 1 s2.0 S2405844020304485 MainDocument5 pages1 s2.0 S2405844020304485 MainSome LaNo ratings yet
- Male circumcision reduces risk of penile cancer: systematic review and meta-analysisDocument14 pagesMale circumcision reduces risk of penile cancer: systematic review and meta-analysisyongky sugandaNo ratings yet
- Current Status of Knowledge, Attitude and Practice (KAP) and Screening For Cervical Cancer in Countries at Different Levels of DevelopmentDocument7 pagesCurrent Status of Knowledge, Attitude and Practice (KAP) and Screening For Cervical Cancer in Countries at Different Levels of DevelopmentHuzaifa SaeedNo ratings yet
- 2 Erewrf 242Document5 pages2 Erewrf 242supaidi97No ratings yet
- 1 s2.0 S092375341935241X MainDocument8 pages1 s2.0 S092375341935241X MainMaria PalNo ratings yet
- AtomDocument13 pagesAtomapi-3821924No ratings yet
- Idosr Journal of Biochemistry, Biotechnology and Allied Fields 8 (3) : 101-118, 2023Document18 pagesIdosr Journal of Biochemistry, Biotechnology and Allied Fields 8 (3) : 101-118, 2023KIU PUBLICATION AND EXTENSIONNo ratings yet
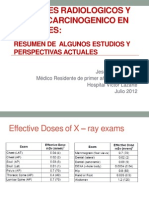
- Examenes Radiologicos y Riesgo de Cancer en PacientesDocument27 pagesExamenes Radiologicos y Riesgo de Cancer en PacientesMaría Isabel Clara Aponte OrtizNo ratings yet
- Risk Factors for Cervical Cancer StudyDocument7 pagesRisk Factors for Cervical Cancer StudyIntania RosatiNo ratings yet
- Thyroid Disorders: Evaluation and Management of Thyroid NodulesDocument13 pagesThyroid Disorders: Evaluation and Management of Thyroid NodulesГулпе АлексейNo ratings yet
- Factors Affecting the Approaches and Complications of Surgery InDocument8 pagesFactors Affecting the Approaches and Complications of Surgery InAlin VázquezNo ratings yet
- Head Neck Cancer DR P.KDocument32 pagesHead Neck Cancer DR P.KshitalsuranaNo ratings yet
- Kuipersetal CRC NRDP2015Document26 pagesKuipersetal CRC NRDP2015Robert ChristevenNo ratings yet
- Factors Delaying Cancer Care and Outcomes in Tamil NaduDocument22 pagesFactors Delaying Cancer Care and Outcomes in Tamil NaduPrasanna ShanNo ratings yet
- Mobile Phone Use and Risk of Thyroid Gland Lesions Detected by UltrasonographyDocument8 pagesMobile Phone Use and Risk of Thyroid Gland Lesions Detected by UltrasonographyLannydchandraNo ratings yet
- BMC Cancer: Prognostic Factors Associated With The Survival of Oral and Pharyngeal Carcinoma in TaiwanDocument11 pagesBMC Cancer: Prognostic Factors Associated With The Survival of Oral and Pharyngeal Carcinoma in TaiwanLinaena MericyNo ratings yet
- Early Detection Saves Lives: ManagementDocument2 pagesEarly Detection Saves Lives: Managementsharu4291No ratings yet
- Problem Statement WORLD Cancer Afflicts All Communities WorldwideDocument30 pagesProblem Statement WORLD Cancer Afflicts All Communities Worldwidesalma0430100% (2)
- UV CANCER STUDYDocument10 pagesUV CANCER STUDYAlexander HunterNo ratings yet
- APBIDocument28 pagesAPBIWindy HardiyantyNo ratings yet
- Knowledge, Attitude and Practice Toward Cervical Cancer and Cervical Cancer Screening and Its Associated Factors Among Women in The City of Bamenda, CameroonDocument17 pagesKnowledge, Attitude and Practice Toward Cervical Cancer and Cervical Cancer Screening and Its Associated Factors Among Women in The City of Bamenda, CameroonEditor IJTSRDNo ratings yet
- Caca GuidelinesDocument42 pagesCaca GuidelinescsaralatNo ratings yet
- Tumor Laring MedscapeDocument19 pagesTumor Laring Medscapemegayani santosoNo ratings yet
- Lubitz Et Al - The Changing Landscape of Papillary Thyroid Cancer Epidemiology, Management, and The Implications For PatientsDocument6 pagesLubitz Et Al - The Changing Landscape of Papillary Thyroid Cancer Epidemiology, Management, and The Implications For PatientsDedy AditiaNo ratings yet
- Author's Accepted Manuscript: Free Radical Biology and MedicineDocument26 pagesAuthor's Accepted Manuscript: Free Radical Biology and MedicineMerlin MuktialiNo ratings yet
- Health-Related Quality of Life and Needs of Careand Support of Adult Tanzanians With Cancer:a Mixed-Methods StudyDocument11 pagesHealth-Related Quality of Life and Needs of Careand Support of Adult Tanzanians With Cancer:a Mixed-Methods StudyDave LokaleNo ratings yet
- Thyroid Cancer Diagnosis and TreatmentDocument6 pagesThyroid Cancer Diagnosis and TreatmentBastiaanNo ratings yet
- Critical Reviews in Oncology / HematologyDocument11 pagesCritical Reviews in Oncology / HematologyAhmad aNo ratings yet
- Articol2 1Document6 pagesArticol2 1Smaranda GavrilNo ratings yet
- Epidem Cancer ColorectalDocument5 pagesEpidem Cancer ColorectalAna MîndrilăNo ratings yet
- Semb 57 287Document18 pagesSemb 57 287samruizayalaNo ratings yet
- Article Review: Disease and Economic Burden of Prostate Cancer in Malaysia: A ReviewDocument8 pagesArticle Review: Disease and Economic Burden of Prostate Cancer in Malaysia: A ReviewMeiselAdeliaNo ratings yet
- Colorectal Cancer Screening English 2007 PDFDocument18 pagesColorectal Cancer Screening English 2007 PDFtanjudinNo ratings yet
- ESGOESTROESP Guidelines for the Management of Patients With Cervical Cancer – Update 2023Document32 pagesESGOESTROESP Guidelines for the Management of Patients With Cervical Cancer – Update 2023Limbert Rodríguez TiconaNo ratings yet
- New Study Finds That Taking Supplements Halves The Risk of Breast Cancer (Pan 2011)Document12 pagesNew Study Finds That Taking Supplements Halves The Risk of Breast Cancer (Pan 2011)EMFsafetyNo ratings yet
- Project Proposal Charera CPDocument27 pagesProject Proposal Charera CPClifford ChareraNo ratings yet
- Worldwide Burden of Colorectal Cancer: A ReviewDocument5 pagesWorldwide Burden of Colorectal Cancer: A ReviewRomário CerqueiraNo ratings yet
- Journal Pmed 1000337Document9 pagesJournal Pmed 1000337Kristine BradyNo ratings yet
- ESMO Guideline 2019 - Early Breast Cancer TreatmentDocument27 pagesESMO Guideline 2019 - Early Breast Cancer Treatmentrahma watiNo ratings yet
- Manejo de Neoplasia Intraepitelial AnalDocument10 pagesManejo de Neoplasia Intraepitelial AnalLibertad DíazNo ratings yet
- Epidemiological Profile of Gynecologic Breast Cancer inDocument3 pagesEpidemiological Profile of Gynecologic Breast Cancer indomi kalondaNo ratings yet
- Kuipers 2015Document25 pagesKuipers 2015Fahmi RizalNo ratings yet
- Genotypes and Associated Risk Levels of Human Papilloma Virus Among Female Patients Attending Rabuor Sub County Hospital, KisumuDocument13 pagesGenotypes and Associated Risk Levels of Human Papilloma Virus Among Female Patients Attending Rabuor Sub County Hospital, KisumuMJBAS JournalNo ratings yet
- BMJ 2013 346:F2360 (: Free Full-Text BMJ Article PDF Pubmed® AbstractDocument3 pagesBMJ 2013 346:F2360 (: Free Full-Text BMJ Article PDF Pubmed® AbstractintrascribdNo ratings yet
- Viel2008 Article DioxinEmissionsFromAMunicipalSDocument8 pagesViel2008 Article DioxinEmissionsFromAMunicipalSJefersson TiqueNo ratings yet
- Epidemiology and Screening For Renal CancerDocument14 pagesEpidemiology and Screening For Renal CancermicozaaaNo ratings yet
- Childhood Cancer Literature ReviewDocument4 pagesChildhood Cancer Literature Reviewafmzjbxmbfpoox100% (1)
- Prospects and Potential For Expanding Women's Oncofertility Options - Gabriella TranDocument18 pagesProspects and Potential For Expanding Women's Oncofertility Options - Gabriella TrannurjNo ratings yet
- Testicular Cancer Cure Saves $150M AnnuallyDocument26 pagesTesticular Cancer Cure Saves $150M AnnuallyFeddyFebriyantoManurungNo ratings yet
- Paper Environmental Risk of Cancer (Lectura)Document7 pagesPaper Environmental Risk of Cancer (Lectura)Claudio ManríquezNo ratings yet
- 1 s2.0 S2666679022000040 MainDocument14 pages1 s2.0 S2666679022000040 MainRahmayantiYuliaNo ratings yet
- Anal Cancer Guidelines 2014Document12 pagesAnal Cancer Guidelines 2014Alfredo Alfaro CarvajalNo ratings yet
- The Status of Colorectal Cancer Care in The Netherlands: Past, Present and FutureDocument6 pagesThe Status of Colorectal Cancer Care in The Netherlands: Past, Present and FutureIlija TripkovićNo ratings yet
- Breast TBDocument9 pagesBreast TBSehrish SiddiqueNo ratings yet
- Knowledge of Cancer Risk Factors, Symptoms, and Barriers To Seeking Medical Help Among Omani AdolescentsDocument12 pagesKnowledge of Cancer Risk Factors, Symptoms, and Barriers To Seeking Medical Help Among Omani AdolescentsAnak Agung Bagus WirayudaNo ratings yet
- PG Art 34580-10Document15 pagesPG Art 34580-10Horia MineaNo ratings yet
- Close, But Still Too Far. The Experience of Australian People With Cancer Commuting From A Regional To A Capital City For Radiotherapy TreatmentDocument8 pagesClose, But Still Too Far. The Experience of Australian People With Cancer Commuting From A Regional To A Capital City For Radiotherapy TreatmentyouldenaNo ratings yet
- CADCAM and Digital Impression PDFDocument11 pagesCADCAM and Digital Impression PDFEm EryNo ratings yet
- Cone Beam Computerized Tomography-Based Dental Imaging For Implant Planning and Surgical Guidance, Part 1 - Single Implant in The Mandibular Molar RegionDocument5 pagesCone Beam Computerized Tomography-Based Dental Imaging For Implant Planning and Surgical Guidance, Part 1 - Single Implant in The Mandibular Molar RegionEm EryNo ratings yet
- Dental Imaging in Implant Treatment PlanningDocument11 pagesDental Imaging in Implant Treatment PlanningEm EryNo ratings yet
- Virtual Planning of ImplantDocument6 pagesVirtual Planning of ImplantChekkarraj Sharanya KeshapurNo ratings yet
- ProteticaDocument13 pagesProteticaNico LucaciNo ratings yet
- The Science and Art of Tooth WhiteningDocument11 pagesThe Science and Art of Tooth WhiteningEm EryNo ratings yet
- Innovation in Dentistry - CADCAM Restorative Procedures PDFDocument14 pagesInnovation in Dentistry - CADCAM Restorative Procedures PDFEm EryNo ratings yet
- CADCAM Dentistry and Chair Digital Impression Making PDFDocument12 pagesCADCAM Dentistry and Chair Digital Impression Making PDFEm EryNo ratings yet
- What'sup With WhiteningDocument10 pagesWhat'sup With WhiteningEm EryNo ratings yet
- THYROID AND PERIODONTAL DISEASEDocument10 pagesTHYROID AND PERIODONTAL DISEASEEm EryNo ratings yet
- A Clinical Report On Chairside WhiteningDocument11 pagesA Clinical Report On Chairside WhiteningEm EryNo ratings yet
- CAMBRA - Best Practices in Dental Caries PDFDocument15 pagesCAMBRA - Best Practices in Dental Caries PDFEm Ery100% (1)
- Thyroid Disorders Part III Neoplastic Thyroid Disease LIttle 2006Document6 pagesThyroid Disorders Part III Neoplastic Thyroid Disease LIttle 2006Jing XueNo ratings yet
- 2019 Aldulaijan Relationship Between Hypothryoidism and Periodontitis - A Scoping ReviewDocument11 pages2019 Aldulaijan Relationship Between Hypothryoidism and Periodontitis - A Scoping ReviewEm EryNo ratings yet
- 2015 Monea Oral - Health - Status - in - Patients - With - Thyroid Disorders PDFDocument3 pages2015 Monea Oral - Health - Status - in - Patients - With - Thyroid Disorders PDFEm EryNo ratings yet
- 2016 Lee Management of Hyperthyroid Patients in Dental Emergencies - A Case ReportDocument4 pages2016 Lee Management of Hyperthyroid Patients in Dental Emergencies - A Case ReportEm EryNo ratings yet
- 2015 Dental Management of Patients With Thyroid DysfunctionDocument8 pages2015 Dental Management of Patients With Thyroid DysfunctionEm EryNo ratings yet
- Denture Duplication and Implant Stent FabricationDocument6 pagesDenture Duplication and Implant Stent FabricationEm EryNo ratings yet
- 2012 So Hypothyroidism Investigation and Management PDFDocument7 pages2012 So Hypothyroidism Investigation and Management PDFEm EryNo ratings yet
- 2011 Chandna Oral Manifestations of Thyroid Disorders and Its ManagementDocument4 pages2011 Chandna Oral Manifestations of Thyroid Disorders and Its ManagementEm EryNo ratings yet
- Dental Management of Hypothyroidism Patient - Risks and Safety MeasuresDocument4 pagesDental Management of Hypothyroidism Patient - Risks and Safety MeasuresEm EryNo ratings yet
- 2012 Hosur Study of Thyroid Hormones fT3, fT4 and TSH in Subjects With Dental FluorosisDocument7 pages2012 Hosur Study of Thyroid Hormones fT3, fT4 and TSH in Subjects With Dental FluorosisEm EryNo ratings yet
- Self-Assessment Tool For Infection Control: First EditionDocument34 pagesSelf-Assessment Tool For Infection Control: First EditionEm EryNo ratings yet
- Thyroid and DentalDocument10 pagesThyroid and DentalRajah Kano100% (1)
- 9089286Document7 pages9089286Ahmad AlawnehNo ratings yet
- 1981 Mueller Management of A Hyperthyroid Dental Patient Utilizing General Anaesthesia PDFDocument3 pages1981 Mueller Management of A Hyperthyroid Dental Patient Utilizing General Anaesthesia PDFEm EryNo ratings yet
- Evaluating the Temporomandibular Joint with Radiographic TechniquesDocument10 pagesEvaluating the Temporomandibular Joint with Radiographic TechniquesEm EryNo ratings yet
- Success With Occlusal SplintsDocument8 pagesSuccess With Occlusal SplintsEm EryNo ratings yet
- DentureDocument11 pagesDenturedrgayen6042No ratings yet
- 1 Administering OxygenDocument6 pages1 Administering OxygentlokingNo ratings yet
- Ob History Taking and Physical Exam Guide QuestionsDocument3 pagesOb History Taking and Physical Exam Guide QuestionsRaquel PagdangananNo ratings yet
- Cardiovascular Exam GuideDocument4 pagesCardiovascular Exam GuidearchanaNo ratings yet
- CBG Cannabinoid Benefits and EffectsDocument10 pagesCBG Cannabinoid Benefits and EffectsjohnnemanicNo ratings yet
- Neurorehabilitation in Neuro-Oncology 2019 E-BookDocument254 pagesNeurorehabilitation in Neuro-Oncology 2019 E-BookWoffe SoloNo ratings yet
- Seminar: Sinéad M Langan, Alan D Irvine, Stephan WeidingerDocument16 pagesSeminar: Sinéad M Langan, Alan D Irvine, Stephan WeidingerMaria Paulina EstradaNo ratings yet
- Nursing Care Plan - Docx For CVD (Midterm Case Study)Document8 pagesNursing Care Plan - Docx For CVD (Midterm Case Study)Charisma NecesarioNo ratings yet
- Nutrition Diagnosis and Plan of CareDocument115 pagesNutrition Diagnosis and Plan of CareJulian PapinaNo ratings yet
- Shea Dorsey CV 07-Apr-2023Document3 pagesShea Dorsey CV 07-Apr-2023api-668697374No ratings yet
- Pyloric StenosisDocument14 pagesPyloric Stenosisgangguan hepatobilierNo ratings yet
- Clinical Manifestations and Diagnosis of Vitamin B12 and Folate Deficiency - UpToDateDocument63 pagesClinical Manifestations and Diagnosis of Vitamin B12 and Folate Deficiency - UpToDateHuỳnh Thị Khả DuyNo ratings yet
- Health and Privacy PDFDocument40 pagesHealth and Privacy PDFMonika NegiNo ratings yet
- Scoliosis Clinical & ExerciseDocument14 pagesScoliosis Clinical & ExercisePurohit_RNo ratings yet
- CDC 2017 0019 0010 - ContentDocument156 pagesCDC 2017 0019 0010 - ContentTrey Martin-EllisNo ratings yet
- ClavusDocument4 pagesClavusargie3333No ratings yet
- Nursing Care Plan Ineffective Tissue PerfusionDocument1 pageNursing Care Plan Ineffective Tissue Perfusionderic83% (29)
- Six Tiered HMDocument21 pagesSix Tiered HMDoctors NewsNo ratings yet
- Acute Rheumatic FeverDocument39 pagesAcute Rheumatic Fevernikhil00007100% (1)
- S2 Session 1Document3 pagesS2 Session 1s9419No ratings yet
- Cinnamon Contact Stomatitis: A Case Report and ReviewDocument2 pagesCinnamon Contact Stomatitis: A Case Report and ReviewDwiNo ratings yet
- Gender Sensitivity in the PhilippinesDocument46 pagesGender Sensitivity in the PhilippinesMedardo BombitaNo ratings yet
- Areeb Organics Tri-Fold BrochureDocument6 pagesAreeb Organics Tri-Fold Brochurerubana reazNo ratings yet
- CLINPR 100331 Edit ReportDocument8 pagesCLINPR 100331 Edit Reportjohnysalem88No ratings yet
- NCP - LeprosyDocument3 pagesNCP - LeprosyKevin DareNo ratings yet
- Z-03 Digest Part EVDocument50 pagesZ-03 Digest Part EVXaveer AzadNo ratings yet
- Disusun Untuk Memenuhi Sebagian Syarat Kepaniteraan Klinik Dibagian Ilmu Penyakit Anak RSUD MuntilanDocument3 pagesDisusun Untuk Memenuhi Sebagian Syarat Kepaniteraan Klinik Dibagian Ilmu Penyakit Anak RSUD MuntilanAdistha TofanoNo ratings yet
- Radionics - Lowe Chronically IllDocument6 pagesRadionics - Lowe Chronically IllE Paty VázquezNo ratings yet
- WHO - Adherence ReportDocument211 pagesWHO - Adherence Reportscratch9100% (1)
- Shakespeare's Sonnet 147: Obsessive Love as SicknessDocument1 pageShakespeare's Sonnet 147: Obsessive Love as SicknessItrumas SinghNo ratings yet
- Asssessment Nursing Diagnosis Plan of Care Interventions Rationale EvaluationDocument5 pagesAsssessment Nursing Diagnosis Plan of Care Interventions Rationale EvaluationRoldan VidadNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (14)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)