You might also like
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- NSAIDs and DMARDs - Dr. FabilaDocument9 pagesNSAIDs and DMARDs - Dr. FabilaDylan MansillaNo ratings yet
- Anti-Thyroid and Thyroid DrugsDocument36 pagesAnti-Thyroid and Thyroid DrugsDylan MansillaNo ratings yet
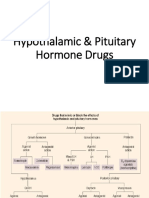
- Hypothalamic & Pituitary Hormone DrugsDocument29 pagesHypothalamic & Pituitary Hormone DrugsDylan MansillaNo ratings yet
- Agents For BoneDocument43 pagesAgents For BoneDylan MansillaNo ratings yet
- Surgery Block 2.1 - Abdominal, Rectal Injury (Dr. Lozada) - 2Document6 pagesSurgery Block 2.1 - Abdominal, Rectal Injury (Dr. Lozada) - 2Dylan MansillaNo ratings yet
- Dystocia Due To Abnormalities of The Bony and Soft Parts PassagesDocument4 pagesDystocia Due To Abnormalities of The Bony and Soft Parts PassagesDylan MansillaNo ratings yet
- Block 2.2 - Mental/Defense MechanismDocument6 pagesBlock 2.2 - Mental/Defense MechanismDylan MansillaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Quiz Chapter 62 63Document2 pagesQuiz Chapter 62 63Amelie AvenidoNo ratings yet
- InflammationDocument49 pagesInflammationGAURAV100% (1)
- The Immune System - Test QuestionsDocument4 pagesThe Immune System - Test QuestionsflorinNo ratings yet
- New Microsoft Office Word DocumentDocument6 pagesNew Microsoft Office Word DocumentAkanksha SharmaNo ratings yet
- Major Histocompatibility Complex Part 1 TranscriptDocument24 pagesMajor Histocompatibility Complex Part 1 Transcriptapi-273068056No ratings yet
- Infection Strategies of Bacterial and Viral Pathogens Through Pathogen-Human Protein-Protein InteractionsDocument11 pagesInfection Strategies of Bacterial and Viral Pathogens Through Pathogen-Human Protein-Protein InteractionssumitbitbtNo ratings yet
- Respiratory Syncytial Virus Infection in CattleDocument10 pagesRespiratory Syncytial Virus Infection in CattleDayanna MorenoNo ratings yet
- PARASITIC NEMATODES Molecular Biology, Biochemistry and ImmunologyDocument498 pagesPARASITIC NEMATODES Molecular Biology, Biochemistry and Immunologydouglasman100% (3)
- Crossm: Incipient and Subclinical Tuberculosis: A Clinical Review of Early Stages and Progression of InfectionDocument24 pagesCrossm: Incipient and Subclinical Tuberculosis: A Clinical Review of Early Stages and Progression of InfectionCharles SandyNo ratings yet
- Us5676977 PDFDocument4 pagesUs5676977 PDFAmirul TechnoTeenzNo ratings yet
- NEET UG Biology Human Health and DiseasesDocument18 pagesNEET UG Biology Human Health and DiseasesMansoor MalikNo ratings yet
- DrMercola SiimLandandJamesDiNicolantonio TheImmunityFixDocument28 pagesDrMercola SiimLandandJamesDiNicolantonio TheImmunityFixRocco LamponeNo ratings yet
- Phagocytic Immuno DefficienciesDocument38 pagesPhagocytic Immuno Defficienciesصدام حسینNo ratings yet
- Urticaria and AngioedemaDocument40 pagesUrticaria and AngioedemaDea LeeteukNo ratings yet
- Hema 2 WBCDocument30 pagesHema 2 WBCAngge Aquino OfficialNo ratings yet
- The Periodontal Health Status of Invisalign Patients A Clinical StudyDocument72 pagesThe Periodontal Health Status of Invisalign Patients A Clinical Studyplayer osamaNo ratings yet
- Kapita Selekta The King B.Inggris 12 SMADocument10 pagesKapita Selekta The King B.Inggris 12 SMAFathimah AuliaNo ratings yet
- Smolen 2016Document16 pagesSmolen 2016downloadcmpNo ratings yet
- Lec 9 Antihuman Globulin TestingDocument9 pagesLec 9 Antihuman Globulin TestingMelaine Grace Gemoranion GeopanoNo ratings yet
- Aabb Antibody Id ApproachDocument127 pagesAabb Antibody Id ApproachRounak Dubey29% (7)
- ΕΙΔΟΣ 4Document6 pagesΕΙΔΟΣ 4Julia ZorlouNo ratings yet
- B. SC Nursing Syllabus INC PDFDocument183 pagesB. SC Nursing Syllabus INC PDFSathya Palanisamy75% (28)
- Immunesera ProductionDocument22 pagesImmunesera Productionnilima nikaljeNo ratings yet
- USMLE Road Map Immunology (001-102) PDFDocument102 pagesUSMLE Road Map Immunology (001-102) PDFJonathan B Gutierrez LeyvaNo ratings yet
- F2 SC PBD Plus C3-4Document14 pagesF2 SC PBD Plus C3-4Teck WeeNo ratings yet
- The Role of IgADocument3 pagesThe Role of IgAullifannuriNo ratings yet
- Bio PoemDocument3 pagesBio Poemapi-4039173890% (1)
- Amniofix Injectable Data SheetDocument2 pagesAmniofix Injectable Data Sheetapi-235072265100% (2)
- Grand Coaching: Medical Surgical NursingDocument22 pagesGrand Coaching: Medical Surgical NursingEsarpy (Nana)No ratings yet
- Clinicopathologic Principles For Veterinary MedicineDocument449 pagesClinicopathologic Principles For Veterinary Medicineoviang100% (1)