You might also like
- Advances in Vestibular Schwannoma Microneurosurgery: Improving Results with New TechnologiesFrom EverandAdvances in Vestibular Schwannoma Microneurosurgery: Improving Results with New TechnologiesLuciano MastronardiNo ratings yet
- An Atypical Esthesioneuroblastoma of The Sphenoid Sinus A Case ReportDocument4 pagesAn Atypical Esthesioneuroblastoma of The Sphenoid Sinus A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Squamous Cell Carcinoma of Tympanomastoid Region - A Rare and Often Misdiagnosed EntityDocument4 pagesSquamous Cell Carcinoma of Tympanomastoid Region - A Rare and Often Misdiagnosed EntitymawarmelatiNo ratings yet
- An External Auditory Canal Lesion: Lobular Capillary HemangiomaDocument2 pagesAn External Auditory Canal Lesion: Lobular Capillary HemangiomaKsh Kim Sohyun INo ratings yet
- Lawrence Et Al 2021 Contralateral Transmaxillary Approach For Resection of Chondrosarcoma of The Petrous Apex A CaseDocument4 pagesLawrence Et Al 2021 Contralateral Transmaxillary Approach For Resection of Chondrosarcoma of The Petrous Apex A CaseSourabh PatroNo ratings yet
- Non-Cholesteatomatous Chronic Otitis Media Complicated With Suppurative LabyrinthitisDocument4 pagesNon-Cholesteatomatous Chronic Otitis Media Complicated With Suppurative LabyrinthitisLarasati Gilang Fuzi AstutiNo ratings yet
- Case Report: A Case of Conservatively Managed Invasive Ceruminoma and A Review of The LiteratureDocument4 pagesCase Report: A Case of Conservatively Managed Invasive Ceruminoma and A Review of The Literaturesaffrin syedNo ratings yet
- Cerebellar Abscess and Sigmoid Sinus Thrombosis from Chronic Ear InfectionDocument3 pagesCerebellar Abscess and Sigmoid Sinus Thrombosis from Chronic Ear Infectionmuthiadewi31No ratings yet
- Imaging The Temporal Bone: NeuroradiologyDocument15 pagesImaging The Temporal Bone: NeuroradiologyMaulidianaIndahNo ratings yet
- BIBL 12 Liver MetastasisDocument3 pagesBIBL 12 Liver Metastasisstoia_sebiNo ratings yet
- Cholesteatoma of External Auditory CanalDocument5 pagesCholesteatoma of External Auditory CanallolNo ratings yet
- A Case of Maxillary Sinus CarcinomaDocument3 pagesA Case of Maxillary Sinus CarcinomajasmniaNo ratings yet
- International Journal Orthodontics 3Document11 pagesInternational Journal Orthodontics 3helmysiswantoNo ratings yet
- Frontal Sinus CholesteatomaDocument6 pagesFrontal Sinus CholesteatomaasiyazaidiaNo ratings yet
- Adenoma 2020Document11 pagesAdenoma 2020Residentes AudiologiaNo ratings yet
- Ghan em 2005Document5 pagesGhan em 2005asfwegereNo ratings yet
- External CholesteatomDocument5 pagesExternal CholesteatomIvana SupitNo ratings yet
- Medial Orbital Epidermoid Cyst: Case ReportDocument3 pagesMedial Orbital Epidermoid Cyst: Case ReportTeodorNo ratings yet
- Jurnal Case Report Carcinoma Maxillaris PDFDocument3 pagesJurnal Case Report Carcinoma Maxillaris PDFEnvhy WinaNo ratings yet
- Journal of Oral and Maxillofacial Surgery, Medicine, and PathologyDocument7 pagesJournal of Oral and Maxillofacial Surgery, Medicine, and PathologyOMFS FKG UnimusNo ratings yet
- (10920684 - Neurosurgical Focus) Olfactory Groove MeningiomasDocument5 pages(10920684 - Neurosurgical Focus) Olfactory Groove Meningiomasnithin shenoiNo ratings yet
- Otogenic Deep Neck Abscess: A Rare Complication of Cholesteatoma With Acute MastoiditisDocument6 pagesOtogenic Deep Neck Abscess: A Rare Complication of Cholesteatoma With Acute MastoiditisGondo RukemNo ratings yet
- Combined Treatment of Surgery and Sclerotherapy For Sinus PericraniiDocument5 pagesCombined Treatment of Surgery and Sclerotherapy For Sinus Pericranii相壮壮No ratings yet
- American Journal of OtolaryngologyDocument4 pagesAmerican Journal of OtolaryngologyDear Farah SielmaNo ratings yet
- SAARC ENT Conference - Leison Maharjan - External Auditory Canal CholesteatomaDocument1 pageSAARC ENT Conference - Leison Maharjan - External Auditory Canal CholesteatomaAshokNo ratings yet
- Unsafe Chronic Suppurative Otitis Media With Cerebellar AbscessDocument5 pagesUnsafe Chronic Suppurative Otitis Media With Cerebellar Abscessary wisma dewiNo ratings yet
- Prevention and Management of Vascular Complications in Middle Ear and Cochlear Implant SurgeryDocument10 pagesPrevention and Management of Vascular Complications in Middle Ear and Cochlear Implant SurgerySiska HarapanNo ratings yet
- Ijcmr 692 Jun 14Document2 pagesIjcmr 692 Jun 14Jeyachandran MariappanNo ratings yet
- Meningoencephalocele of The Temporal Bone-A Case Report: DR.B.V.N Muralidhar Reddy, DR K.V.V.RamjiDocument6 pagesMeningoencephalocele of The Temporal Bone-A Case Report: DR.B.V.N Muralidhar Reddy, DR K.V.V.RamjiNityaNo ratings yet
- NMCCRJ 5 111Document3 pagesNMCCRJ 5 111WildaHanimNo ratings yet
- Radiological Study of The Temporal Bone in Chronic Otitis Media: Prospective Study of 50 CasesDocument8 pagesRadiological Study of The Temporal Bone in Chronic Otitis Media: Prospective Study of 50 CasesReni Wahyu NoviantiNo ratings yet
- Recurrent Aneurysmal Bone Cyst of The Mandibular Condyle With Soft Tissue ExtensionDocument5 pagesRecurrent Aneurysmal Bone Cyst of The Mandibular Condyle With Soft Tissue ExtensionlalajanNo ratings yet
- Low-Grade Chondrosarcoma of The Posterior Cricoid Plate: Corresponding Author: Christy M. Moen, Christy@moen - Co.ukDocument4 pagesLow-Grade Chondrosarcoma of The Posterior Cricoid Plate: Corresponding Author: Christy M. Moen, Christy@moen - Co.ukLizbeth QuinteroNo ratings yet
- SS ArticleDocument8 pagesSS ArticleWhite Feather Dental GurgaonNo ratings yet
- Diagnosis and Management of Silent Sinus SyndromeDocument2 pagesDiagnosis and Management of Silent Sinus SyndromeRaja Fauzan FahleviNo ratings yet
- Anatomy and Its Variations For Endoscopic Sinus Surgery: 10.5005/jp-Journals-10013-1122Document8 pagesAnatomy and Its Variations For Endoscopic Sinus Surgery: 10.5005/jp-Journals-10013-1122opi akbarNo ratings yet
- Sinonasal Imaging PDFDocument17 pagesSinonasal Imaging PDFBelanny DwiNo ratings yet
- 12 Juvenile NasopharyngealDocument5 pages12 Juvenile NasopharyngealkhairanifahmaNo ratings yet
- Case Report: Olfactory Loss and Unrelated Chronic RhinosinusitisDocument4 pagesCase Report: Olfactory Loss and Unrelated Chronic RhinosinusitisRegina Dwindarti DarostyNo ratings yet
- Unusual Presentation of Adamantinoma With Synchronous 2024 International JouDocument5 pagesUnusual Presentation of Adamantinoma With Synchronous 2024 International JouRonald QuezadaNo ratings yet
- Case ReportDocument8 pagesCase Reportarief ardaNo ratings yet
- Role of CT Scan in Diagnosis and Management of Otogenic Intracranial AbscessDocument5 pagesRole of CT Scan in Diagnosis and Management of Otogenic Intracranial AbscessayundariprimaraniNo ratings yet
- Coronectomy: Indications, Outcomes, and Description of TechniqueDocument6 pagesCoronectomy: Indications, Outcomes, and Description of TechniqueHélio FonteneleNo ratings yet
- Brain AbsesDocument4 pagesBrain Absesmuthiadewi31No ratings yet
- Journal of Cranio-Maxillo-Facial Surgery: Yehuda Zadik, Alper Aktas, Scott Drucker, Dorrit W. NitzanDocument6 pagesJournal of Cranio-Maxillo-Facial Surgery: Yehuda Zadik, Alper Aktas, Scott Drucker, Dorrit W. Nitzan刘雨樵No ratings yet
- Unicystic AmeloblastomaDocument5 pagesUnicystic AmeloblastomaayuNo ratings yet
- Angiomyolipoma of The Hard Palate: Clinical ReportDocument2 pagesAngiomyolipoma of The Hard Palate: Clinical ReportKezia Rachellea MustakimNo ratings yet
- Glomus Tympanicum Type III-with Delayed Postoperative Facial Palsy: Our ExperienceDocument4 pagesGlomus Tympanicum Type III-with Delayed Postoperative Facial Palsy: Our ExperienceAdriani HartantoNo ratings yet
- Transcanal Endoscopic Mastoid Surgery With Tympanoplasty For The Management of CholesteatomaDocument8 pagesTranscanal Endoscopic Mastoid Surgery With Tympanoplasty For The Management of CholesteatomaShawkat Kamal100% (1)
- Bilateral Bleeding from Ears After Trauma Often Caused by Facial FracturesDocument4 pagesBilateral Bleeding from Ears After Trauma Often Caused by Facial FracturesJubea DoinaNo ratings yet
- Ojolns-11 Issue-II F Color - P 11-14-Solitary Fibrous Tumors of The Nose and Paranasal Sinuses-Our ExperienceDocument4 pagesOjolns-11 Issue-II F Color - P 11-14-Solitary Fibrous Tumors of The Nose and Paranasal Sinuses-Our ExperienceDipak Ranjan NayakNo ratings yet
- Medip, IJRMS-7729 ODocument7 pagesMedip, IJRMS-7729 ORagupathi MNo ratings yet
- Skullbasesurg00039 0009Document7 pagesSkullbasesurg00039 0009subratarobinNo ratings yet
- Neha CR Patho PDFDocument3 pagesNeha CR Patho PDFmanish agrawalNo ratings yet
- J.Operative Approaches To The Pineal Region Tumors.1998Document4 pagesJ.Operative Approaches To The Pineal Region Tumors.1998Kysy CodonNo ratings yet
- Effectiveness of Immediate Primary Correction and Medial Canthopexy in Bilateral Naso-Orbito-Ethmoid FractureDocument7 pagesEffectiveness of Immediate Primary Correction and Medial Canthopexy in Bilateral Naso-Orbito-Ethmoid FracturealexanderNo ratings yet
- Meningioma of The Internal Auditory Canal Case ReportDocument4 pagesMeningioma of The Internal Auditory Canal Case ReportStanley KambeyNo ratings yet
- Incidental Reportzaharopoulos2000Document4 pagesIncidental Reportzaharopoulos2000maglangitmarvincNo ratings yet
- Case Report on Chondrosarcoma of the Temporomandibular JointDocument9 pagesCase Report on Chondrosarcoma of the Temporomandibular JointCatalina Soler LioiNo ratings yet
- Unsatisfactory Results After Tympanoplasty Surgery in Patients With Chronic Purulent Otitis MediaDocument4 pagesUnsatisfactory Results After Tympanoplasty Surgery in Patients With Chronic Purulent Otitis MediaAcademic JournalNo ratings yet
- 10 BESAR PENYAKIT THT RJ 2023Document1 page10 BESAR PENYAKIT THT RJ 2023muhammadNo ratings yet
- LUTS OABDocument32 pagesLUTS OABmuhammadNo ratings yet
- DATA MPPDS YANG MENANGANI PASIEN COVID-19 DI RSUP DR. WAHIDIN SUDIROHUSODO MAKASSARDocument25 pagesDATA MPPDS YANG MENANGANI PASIEN COVID-19 DI RSUP DR. WAHIDIN SUDIROHUSODO MAKASSARmuhammadNo ratings yet
- MR MUHAMMAD ANWAR (4)Document2 pagesMR MUHAMMAD ANWAR (4)muhammadNo ratings yet
- Management of LUTS with BPH-1Document39 pagesManagement of LUTS with BPH-1muhammadNo ratings yet
- Usada+vol +2+no +1+JANUARI+2024+Hal+15-29Document15 pagesUsada+vol +2+no +1+JANUARI+2024+Hal+15-29muhammadNo ratings yet
- COVID-19 Vaccine Breakthrough by SlidesgoDocument49 pagesCOVID-19 Vaccine Breakthrough by SlidesgoAnnisa NurainiNo ratings yet
- Cerebellar Venous Infarction in Chronic Suppurative Otitis MediaDocument4 pagesCerebellar Venous Infarction in Chronic Suppurative Otitis MediamuhammadNo ratings yet
- 4 Dubey2010Document5 pages4 Dubey2010muhammadNo ratings yet
- Rare Fungal Brain Infection PresentationDocument4 pagesRare Fungal Brain Infection PresentationmuhammadNo ratings yet
- Morbid Complications of Otitic Hydrocephalus: Case ReportDocument6 pagesMorbid Complications of Otitic Hydrocephalus: Case ReportmuhammadNo ratings yet
- Brief Report of Special Case Abscess-A Rare Fourth Ventricular MassDocument3 pagesBrief Report of Special Case Abscess-A Rare Fourth Ventricular MassmuhammadNo ratings yet
- Jadwal Rotasi Residen Departemen Ilmu Kesehatan T.H.T.K.L FK - Unhas September 2021Document1 pageJadwal Rotasi Residen Departemen Ilmu Kesehatan T.H.T.K.L FK - Unhas September 2021muhammadNo ratings yet
- Morbid Complications of Otitic Hydrocephalus: Case ReportDocument6 pagesMorbid Complications of Otitic Hydrocephalus: Case ReportmuhammadNo ratings yet
- Jurnal2 AnwarDocument5 pagesJurnal2 AnwarmuhammadNo ratings yet
- P73-Deficient Mice Have Neurological, Pheromonal and Inflammatory DefectsbutlackspontaneoustumoursDocument5 pagesP73-Deficient Mice Have Neurological, Pheromonal and Inflammatory DefectsbutlackspontaneoustumoursmuhammadNo ratings yet
- Baca Nasional Anwar FixDocument30 pagesBaca Nasional Anwar FixmuhammadNo ratings yet
- Diagnostic Criteria For Menière's DiseaseDocument17 pagesDiagnostic Criteria For Menière's DiseasemuhammadNo ratings yet
- YozologDocument2 pagesYozologmuhammadNo ratings yet
- 2 Bhat2007Document3 pages2 Bhat2007muhammadNo ratings yet
- Baca Nasional Anwar FixDocument30 pagesBaca Nasional Anwar FixmuhammadNo ratings yet
- CRP and PCT as biomarkers in distinguishing CAP and COPD exacerbationsDocument5 pagesCRP and PCT as biomarkers in distinguishing CAP and COPD exacerbationsmuhammadNo ratings yet
- ApoptosisDocument2 pagesApoptosiskml21No ratings yet
- Jurnal Hubungan Tingkat Kebisingan Terhadap Penurunan Ambang Dengar Pada NelayanDocument9 pagesJurnal Hubungan Tingkat Kebisingan Terhadap Penurunan Ambang Dengar Pada NelayanRaisha Klinik Vaksinasi YogyakartaNo ratings yet
- Sertifikat Webinar Series 2 Bedah Unhas Dr. Muhammad AnwarDocument2 pagesSertifikat Webinar Series 2 Bedah Unhas Dr. Muhammad AnwarmuhammadNo ratings yet
- Allergic Rhinitis and its Impact on Asthma (ARIA) 2008 UpdateDocument153 pagesAllergic Rhinitis and its Impact on Asthma (ARIA) 2008 UpdateincaudasemperNo ratings yet
- YozologDocument2 pagesYozologmuhammadNo ratings yet
- 1 6 PDFDocument7 pages1 6 PDFmuhammadNo ratings yet
- Noise Induced Hearing Loss (Nihl) : Bsuir Scientific Conference APRIL 2015Document21 pagesNoise Induced Hearing Loss (Nihl) : Bsuir Scientific Conference APRIL 2015muhammadNo ratings yet
- DHO Chapter 1Document2 pagesDHO Chapter 1Victoria SosaNo ratings yet
- Lophomonas Blattarum Infection or Just The Movement of Ciliated Epithelial Cells?Document4 pagesLophomonas Blattarum Infection or Just The Movement of Ciliated Epithelial Cells?AxelWarnerNo ratings yet
- REVISI (Adelita Setiawan 2)Document7 pagesREVISI (Adelita Setiawan 2)Adelita SetiawanNo ratings yet
- Therapeutic Monoclonal Antibodies Approved by FDA in 2019 (Mini Review)Document2 pagesTherapeutic Monoclonal Antibodies Approved by FDA in 2019 (Mini Review)asclepiuspdfsNo ratings yet
- HIV/Syphilis StudiesDocument2 pagesHIV/Syphilis StudiesYusuf Arif SalamNo ratings yet
- NCP (Fatigue)Document1 pageNCP (Fatigue)student_019100% (1)
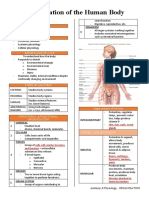
- Organization of the Human BodyDocument8 pagesOrganization of the Human BodyAly HannahNo ratings yet
- Zubiaga, R-Jeane S. - BSN 3 - For PlagscanDocument41 pagesZubiaga, R-Jeane S. - BSN 3 - For PlagscanR-Jeane ZubiagaNo ratings yet
- Witches HerbsDocument3 pagesWitches HerbsAM PNo ratings yet
- Mock Up Test 1Document3 pagesMock Up Test 1Mateusz Radwański100% (1)
- Portfolio PDF Model 9c3265aa 3d4b 4d5d 8ef3 9c888a92a3e5Document53 pagesPortfolio PDF Model 9c3265aa 3d4b 4d5d 8ef3 9c888a92a3e5Guadalupe Rojas100% (1)
- How Do You Know It's TrueDocument36 pagesHow Do You Know It's TrueAANo ratings yet
- Assignment in 118 (Lecture) : C: Compressions A: Airway B: Breathing Compressions: Restore Blood FlowDocument10 pagesAssignment in 118 (Lecture) : C: Compressions A: Airway B: Breathing Compressions: Restore Blood FlowJean ReyesNo ratings yet
- LEGIT 62 Ako 1RST Quarter Exam PDEV 111 1Document23 pagesLEGIT 62 Ako 1RST Quarter Exam PDEV 111 1Mylen Noel Elgincolin Manlapaz50% (2)
- International Journal of Health Sciences and Research: Fetal Umbilical Cord Circumference Measurement and Birth WeightDocument6 pagesInternational Journal of Health Sciences and Research: Fetal Umbilical Cord Circumference Measurement and Birth WeightFatma ElzaytNo ratings yet
- Tendon Injuries of Hand: DR Saumya AgarwalDocument101 pagesTendon Injuries of Hand: DR Saumya AgarwaltesfahuntekletilahunNo ratings yet
- IDSA - Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in WomenDocument7 pagesIDSA - Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in Womenamalia puspita dewiNo ratings yet
- Allergic RhinitisDocument27 pagesAllergic Rhinitispaningbatan.kristine.bNo ratings yet
- DENGUE VIRUS STRAINS AND VECTORSDocument2 pagesDENGUE VIRUS STRAINS AND VECTORSImee Claire PacisNo ratings yet
- Mental Health Consequences of Exercise WithdrawalDocument8 pagesMental Health Consequences of Exercise WithdrawaljasonNo ratings yet
- Gender-Dysphoric-Incongruene Persons, Guidelines JCEM 2017Document35 pagesGender-Dysphoric-Incongruene Persons, Guidelines JCEM 2017Manel EMNo ratings yet
- Bab Vii Daftar PustakaDocument5 pagesBab Vii Daftar Pustaka19 110 Setya Maharani KadirNo ratings yet
- Guia para El Manejo de La Anemia Por Deficiencia de Hierro 2017Document9 pagesGuia para El Manejo de La Anemia Por Deficiencia de Hierro 2017Walther YepesNo ratings yet
- NCM101 TransesDocument6 pagesNCM101 TransesRonel ResurricionNo ratings yet
- Medicine: The Effectiveness of Tai Chi For Postpartum DepressionDocument4 pagesMedicine: The Effectiveness of Tai Chi For Postpartum DepressionNisa RohmatinNo ratings yet
- New Bilibid Prison Medical MissionDocument2 pagesNew Bilibid Prison Medical MissionBenjamin SantiagoNo ratings yet
- NCLEX-RN - REVIEW - NOTES.2018-2019 by Saeid AskariDocument150 pagesNCLEX-RN - REVIEW - NOTES.2018-2019 by Saeid Askarireza babaAli100% (1)
- 2019 BerryDocument15 pages2019 BerrybryaneatscamerasNo ratings yet
- Eotc Camp Permission Form PDFDocument3 pagesEotc Camp Permission Form PDFapi-238963120No ratings yet
- Epistaksis Pada Polip Nasal: September 2022Document10 pagesEpistaksis Pada Polip Nasal: September 2022FitrianiNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (14)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)