You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Personal Financial Literacy: Madura Casey RobertsDocument337 pagesPersonal Financial Literacy: Madura Casey RobertsGrantt ChristianNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Business Plan Aunt NewwwDocument10 pagesBusiness Plan Aunt NewwwpushpamaliNo ratings yet
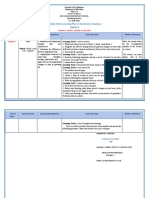
- Weekly Home Learning Plan in Homeroom Guidance Grade 4Document2 pagesWeekly Home Learning Plan in Homeroom Guidance Grade 4JOSEFINA P. LLAMADO86% (7)
- Religious Vrindavan PDFDocument3 pagesReligious Vrindavan PDFanuj sethNo ratings yet
- Other Plant Feasibility Report PDFDocument36 pagesOther Plant Feasibility Report PDFsvvsnrajuNo ratings yet
- 32 Ayala Land Inc Vs ASB Realty Corp GR 210043Document3 pages32 Ayala Land Inc Vs ASB Realty Corp GR 210043Ruben100% (1)
- D Souza Et Al 2023 Menstrual Cycle Hormones and Oral Contraceptives A Multimethod Systems Physiology Based Review ofDocument16 pagesD Souza Et Al 2023 Menstrual Cycle Hormones and Oral Contraceptives A Multimethod Systems Physiology Based Review ofDario GerpeNo ratings yet
- (2017) High-Speed Running and Sprinting As An Injury Risk FactorDocument21 pages(2017) High-Speed Running and Sprinting As An Injury Risk FactorDario GerpeNo ratings yet
- (2014) Applied Physiology of Female SoccerDocument24 pages(2014) Applied Physiology of Female SoccerDario GerpeNo ratings yet
- (2012) Mechanical Work Accounts For Sex Differences in FatigueDocument8 pages(2012) Mechanical Work Accounts For Sex Differences in FatigueDario GerpeNo ratings yet
- (2013) Bruton, Sex Differences in Landing Review, JEK, 2013Document12 pages(2013) Bruton, Sex Differences in Landing Review, JEK, 2013Dario GerpeNo ratings yet
- (2002) The Effect of The Menstrual Cycle On ACL Injuries in Women As Determined by Hormone LevelsDocument2 pages(2002) The Effect of The Menstrual Cycle On ACL Injuries in Women As Determined by Hormone LevelsDario GerpeNo ratings yet
- Perceived Impact of Non-Contact Boxing On Daily Life and OccupatiDocument2 pagesPerceived Impact of Non-Contact Boxing On Daily Life and OccupatiDario GerpeNo ratings yet
- Heart Rate Variability Measurement and Emerging UsDocument11 pagesHeart Rate Variability Measurement and Emerging UsDario GerpeNo ratings yet
- The Relationship Between Running Power and RunningDocument10 pagesThe Relationship Between Running Power and RunningDario GerpeNo ratings yet
- Betty Neuman: The System ModelDocument32 pagesBetty Neuman: The System ModelVincent PolicarNo ratings yet
- Food Waste in School Day 1 Your Name: Jaqueline Pearson Title of Lesson: Food Waste Grade: 2nd StandardsDocument3 pagesFood Waste in School Day 1 Your Name: Jaqueline Pearson Title of Lesson: Food Waste Grade: 2nd StandardsJackiePearsonNo ratings yet
- Journal ReadingDocument21 pagesJournal ReadingRettyNo ratings yet
- SmartStudio User ManualDocument73 pagesSmartStudio User ManualAhmad GustoniNo ratings yet
- Japanese LessonDocument12 pagesJapanese LessonVin CentNo ratings yet
- Remuneration ProformaDocument1 pageRemuneration Proformagirdhargopal87No ratings yet
- PDFDocument5 pagesPDFdhanu1434No ratings yet
- JRY A Quick StudyDocument5 pagesJRY A Quick StudyrkjhunjhunNo ratings yet
- Descriptive TextDocument13 pagesDescriptive Text산이야No ratings yet
- Exams Briefing For Final Year Students Spring 2021Document30 pagesExams Briefing For Final Year Students Spring 2021Van TeaNo ratings yet
- AllahabadDocument2,687 pagesAllahabadRudra MishraNo ratings yet
- Lab Manual 3Document4 pagesLab Manual 3Nazmul Shikder RiyadhNo ratings yet
- Accommodation Costs 2023-2024 With Lease DatesDocument1 pageAccommodation Costs 2023-2024 With Lease DatesMadalongipolahaNo ratings yet
- IRC Publication - Revised Catalogue - 2020Document15 pagesIRC Publication - Revised Catalogue - 2020Shashank VermaNo ratings yet
- Ver Intr 5 PDFDocument9 pagesVer Intr 5 PDFAlina LăzăroiuNo ratings yet
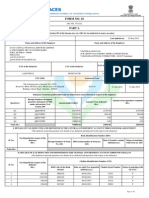
- NSE - National Stock Exchange of India LTDDocument1 pageNSE - National Stock Exchange of India LTDsharath HpNo ratings yet
- General Preprocessing: Chapter ThreeDocument66 pagesGeneral Preprocessing: Chapter ThreeShamik ChowdhuryNo ratings yet
- 002-Annex-3.-Declaration-of-Anti-Plagiarism-and-Absence-of-Conflict-of-Interest MGNSDocument2 pages002-Annex-3.-Declaration-of-Anti-Plagiarism-and-Absence-of-Conflict-of-Interest MGNSDanny R. SalvadorNo ratings yet
- 9-Heirs of Sadhwani v. Sadhwani20210424-12-1h435wjDocument15 pages9-Heirs of Sadhwani v. Sadhwani20210424-12-1h435wjBernadith RectoNo ratings yet
- MicromanufacturingDocument20 pagesMicromanufacturingVishwajeet GuptaNo ratings yet
- Numerical Logic 2Document98 pagesNumerical Logic 2Rafe ANo ratings yet
- Topo Notch Examen Numero 1Document10 pagesTopo Notch Examen Numero 1Jorge Tedesqui EyzaguirreNo ratings yet
- 5 Tips For Effective Resume ScreeningDocument2 pages5 Tips For Effective Resume ScreeningEmonics LLCNo ratings yet
- Listeningpracticetest4 v9 18866574 Trang 2 6,2 8Document12 pagesListeningpracticetest4 v9 18866574 Trang 2 6,2 8Thanh Sang DuNo ratings yet