You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
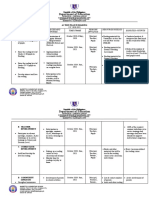
- Lesson Plan FormDocument3 pagesLesson Plan Formapi-377615055No ratings yet
- With Sample On Activities of TBL PDFDocument145 pagesWith Sample On Activities of TBL PDFHaya MonaNo ratings yet
- Lesson Number 7. Audio Video Responsible Safe ManerDocument4 pagesLesson Number 7. Audio Video Responsible Safe ManerBenz CadiongNo ratings yet
- Cornelia Melcu, Etwinning Ambassador, Școala Gimnazială Nr. 9 Nicolae Adriana Lefter, Etwinning Ambassador, Școala Gimnazială ElenaDocument11 pagesCornelia Melcu, Etwinning Ambassador, Școala Gimnazială Nr. 9 Nicolae Adriana Lefter, Etwinning Ambassador, Școala Gimnazială ElenaDaniela BalcanNo ratings yet
- Recomendation Letter For Ms Samone RobinsonDocument2 pagesRecomendation Letter For Ms Samone Robinsonapi-517983133No ratings yet
- Accomplishment Report LilianDocument4 pagesAccomplishment Report LilianDjenela MabagosNo ratings yet
- I. Objectives: Reviewing Previous Lesson or Presenting The New LessonDocument3 pagesI. Objectives: Reviewing Previous Lesson or Presenting The New LessonGenus LuzaresNo ratings yet
- Edtpa Lesson PlanDocument5 pagesEdtpa Lesson Planapi-340408921No ratings yet
- Department of Education: Republic of The PhilippinesDocument3 pagesDepartment of Education: Republic of The PhilippinesJaycel Obina Palang100% (1)
- Learning Online: Veletsianos, GeorgeDocument11 pagesLearning Online: Veletsianos, GeorgePsico XavierNo ratings yet
- Anti-Bullying: A Psychological Support Lesson Plan On The TopicDocument4 pagesAnti-Bullying: A Psychological Support Lesson Plan On The TopicАндрей СГNo ratings yet
- List of Accommodations/Modifications For Classroom Environment For Children With (C) APDDocument3 pagesList of Accommodations/Modifications For Classroom Environment For Children With (C) APDMaria Guy Del DucaNo ratings yet
- Final Supervisor ObservationDocument7 pagesFinal Supervisor Observationapi-270781963No ratings yet
- ABR 311 Study Guide 2024Document45 pagesABR 311 Study Guide 2024mosianetshepo5No ratings yet
- Letter To ParentsDocument1 pageLetter To Parentsapi-373811073No ratings yet
- Assessment On The Efficiency of Technology Use in Teaching and Learning Process at Emilio Aguinaldo College Cavite. ResponsesDocument14 pagesAssessment On The Efficiency of Technology Use in Teaching and Learning Process at Emilio Aguinaldo College Cavite. ResponsesZAMORA REYMARNo ratings yet
- Dr. Thomas Armstrong - Multiple IntelligencesDocument4 pagesDr. Thomas Armstrong - Multiple IntelligencesNicolás FalconeNo ratings yet
- Test, Measurement & EvaluationDocument38 pagesTest, Measurement & EvaluationLeonard Patrick Faunillan BaynoNo ratings yet
- Dewey & VygotskyDocument2 pagesDewey & VygotskyMakunaimaNo ratings yet
- Evaluation Checklist For Technology Integrated LessonDocument3 pagesEvaluation Checklist For Technology Integrated LessonmiksmatiasNo ratings yet
- Vygotsky's Socio-Cultural Theory: Republic of The Philippines Main Campus C.P.G. North Avenue, Tagbilaran CityDocument1 pageVygotsky's Socio-Cultural Theory: Republic of The Philippines Main Campus C.P.G. North Avenue, Tagbilaran Cityrica97No ratings yet
- Clarence Cover LetterDocument1 pageClarence Cover Letterapi-354018402No ratings yet
- Process and Models of Curriculum DevelopmentDocument5 pagesProcess and Models of Curriculum DevelopmentDiana Morilla Azna100% (1)
- THE MEANINGFUL UNITS OF LANGUAGE - RevisedDocument14 pagesTHE MEANINGFUL UNITS OF LANGUAGE - RevisedJoshua DexieNo ratings yet
- Social 8 Course Outline 2021 2022 HSDocument3 pagesSocial 8 Course Outline 2021 2022 HSCole GrundnerNo ratings yet
- The Essential Role of Love in Learning and TeachingDocument2 pagesThe Essential Role of Love in Learning and TeachingSidney SouzaNo ratings yet
- Test and Non Test AssessmentDocument2 pagesTest and Non Test AssessmentMuammar Rifqi75% (12)
- Lesson Plan English 7Document3 pagesLesson Plan English 7ASHLY LYNA DE ASISNo ratings yet
- 6 Integrated Teaching and Learning ApproachesDocument29 pages6 Integrated Teaching and Learning ApproachesJunard MirandaNo ratings yet