You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Life 2e - Upper Intermediate - Unit 3 Test - WordDocument6 pagesLife 2e - Upper Intermediate - Unit 3 Test - WordDanny QuezadaNo ratings yet
- CASE STUDY-1 and 2 - WORDDocument7 pagesCASE STUDY-1 and 2 - WORDAbdul Khaliq Choudhary100% (1)
- Letter of RecommendationDocument1 pageLetter of RecommendationIsaac Kocherla100% (1)
- Suelo Pelvico Ejercicios Con TamponDocument11 pagesSuelo Pelvico Ejercicios Con TamponDanny QuezadaNo ratings yet
- Terapia VibratoriaDocument4 pagesTerapia VibratoriaDanny QuezadaNo ratings yet
- Alfredson Versus Silbernagel ExerciseDocument9 pagesAlfredson Versus Silbernagel ExerciseDanny QuezadaNo ratings yet
- 4 Insurance Sales Incentive Program Ideas That WorkDocument3 pages4 Insurance Sales Incentive Program Ideas That Workgeorge akamaNo ratings yet
- Ψηφιακός Γραμματισμός ΣταΟπτικοακουστικά Μέσα Σε Διαδικτυακά Περιβάλλοντα ΜάθησηςDocument19 pagesΨηφιακός Γραμματισμός ΣταΟπτικοακουστικά Μέσα Σε Διαδικτυακά Περιβάλλοντα ΜάθησηςSofos LoisosNo ratings yet
- No TitleDocument6 pagesNo Titlehwh8w6jmzsNo ratings yet
- Syllabus ChemDocument5 pagesSyllabus ChemDGA GAMINGNo ratings yet
- FrecklesDocument12 pagesFrecklesEnoque PinheiroNo ratings yet
- IV Fluid ChartDocument1 pageIV Fluid ChartQuality CapitalNo ratings yet
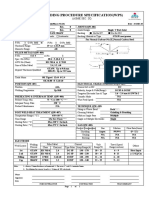
- Welding Procedure Specification (WPS) : (Asme Sec. Ix)Document1 pageWelding Procedure Specification (WPS) : (Asme Sec. Ix)Ahmed Lepda100% (1)
- Union Feb. 10, 2016Document16 pagesUnion Feb. 10, 2016Your News. When You Want It.No ratings yet
- 3rd Quarterly Exam in Mathematics 4Document9 pages3rd Quarterly Exam in Mathematics 4Jaycer De MesaNo ratings yet
- Lab 9Document3 pagesLab 9Tâm NguyễnNo ratings yet
- KBI Admission 2024-25Document1 pageKBI Admission 2024-25jd9170417No ratings yet
- Manual Ga Ma785gt Ud3hDocument104 pagesManual Ga Ma785gt Ud3htrasviviNo ratings yet
- Jawaban Materi 3Document7 pagesJawaban Materi 3Aminatus MahmudahNo ratings yet
- Voltage Divider ExperimentDocument9 pagesVoltage Divider ExperimentJAINo ratings yet
- Yoga Retreat in India - Short Course - Yoga Treatment - Yoga TherapyDocument1 pageYoga Retreat in India - Short Course - Yoga Treatment - Yoga TherapynaveenNo ratings yet
- ASW 0822 Smart Watch With Sleep Function User Guide V10Document2 pagesASW 0822 Smart Watch With Sleep Function User Guide V10Se Jin CoohNo ratings yet
- Prs-021-0025 - C. Melchers - Coca Cola Naga ProjectDocument2 pagesPrs-021-0025 - C. Melchers - Coca Cola Naga ProjectMiko Christopher OroyanNo ratings yet
- A Three-Stage Layer-Based Heuristic To Solve The 3D Bin-Packing ProblemDocument7 pagesA Three-Stage Layer-Based Heuristic To Solve The 3D Bin-Packing ProblemEder NingunoNo ratings yet
- MAX232Document4 pagesMAX232janakiram473No ratings yet
- Marketing Case StudiesDocument10 pagesMarketing Case StudiesSwati ChamariaNo ratings yet
- Revealed Comparative AdvantageDocument5 pagesRevealed Comparative AdvantageiamrahulkumarNo ratings yet
- Sample Size Determination and Confidence Interval Derivation For Exponential DistributionDocument6 pagesSample Size Determination and Confidence Interval Derivation For Exponential DistributionIsmael NeuNo ratings yet
- ECT and A/T Indicator (1KD-FTV, 2KD-FTV), Engine Control (1KD-FTV, 2KD-FTV)Document33 pagesECT and A/T Indicator (1KD-FTV, 2KD-FTV), Engine Control (1KD-FTV, 2KD-FTV)Erick Lizana Neyra100% (4)
- Oil and Gas - Black Gold!Document32 pagesOil and Gas - Black Gold!tabithapangNo ratings yet
- 6 Pre-Transfusion TestingDocument24 pages6 Pre-Transfusion TestingRhema AyuhNo ratings yet
- Trailing Edge Flap Assymmetry PDFDocument6 pagesTrailing Edge Flap Assymmetry PDFViệt DươngNo ratings yet
- Compressed Earth Block: Prepared By: Aditya Shah (M.Tech CPM)Document27 pagesCompressed Earth Block: Prepared By: Aditya Shah (M.Tech CPM)SuryaRajputNo ratings yet
- 40 Questions in 23 Minutes - Maths by Arun SirDocument42 pages40 Questions in 23 Minutes - Maths by Arun SirSatya RanjanNo ratings yet