Professional Documents
Culture Documents
Primera Selección 1 2020
Uploaded by
Ezequiel RiverosCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Primera Selección 1 2020
Uploaded by
Ezequiel RiverosCopyright:
Available Formats
Articles
Investigation of three clusters of COVID-19 in Singapore:
implications for surveillance and response measures
Rachael Pung*, Calvin J Chiew*, Barnaby E Young, Sarah Chin, Mark I-C Chen, Hannah E Clapham, Alex R Cook, Sebastian Maurer-Stroh,
Matthias P H S Toh, Cuiqin Poh, Mabel Low, Joshua Lum, Valerie T J Koh, Tze M Mak, Lin Cui, Raymond V T P Lin, Derrick Heng, Yee-Sin Leo,
David C Lye, Vernon J M Lee*, on behalf of the Singapore 2019 Novel Coronavirus Outbreak Research Team†
Summary
Background Three clusters of coronavirus disease 2019 (COVID-19) linked to a tour group from China, a company Lancet 2020; 395: 1039–46
conference, and a church were identified in Singapore in February, 2020. Published Online
March 16, 2020
https://doi.org/10.1016/
Methods We gathered epidemiological and clinical data from individuals with confirmed COVID-19, via interviews and
S0140-6736(20)30528-6
inpatient medical records, and we did field investigations to assess interactions and possible modes of transmission of
*Contributed equally
severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Open source reports were obtained for overseas cases.
†Members listed at end of
We reported the median (IQR) incubation period of SARS-CoV-2. report
Ministry of Health, Singapore
Findings As of Feb 15, 2020, 36 cases of COVID-19 were linked epidemiologically to the first three clusters of circum (R Pung MSc, C J Chiew MPH,
scribed local transmission in Singapore. 425 close contacts were quarantined. Direct or prolonged close contact was S Chin MPH, C Poh MPH,
reported among affected individuals, although indirect transmission (eg, via fomites and shared food) could not be M Low MPH, J Lum BA,
V T J Koh MPH, D Heng MPH,
excluded. The median incubation period of SARS-CoV-2 was 4 days (IQR 3–6). The serial interval between transmission V J M Lee PhD); National Centre
pairs ranged between 3 days and 8 days. for Infectious Diseases,
Singapore (B E Young MBBChir,
Interpretation SARS-CoV-2 is transmissible in community settings, and local clusters of COVID-19 are expected in M I-C Chen PhD,
Prof Y-S Leo MPH,
countries with high travel volume from China before the lockdown of Wuhan and institution of travel restrictions. D C Lye MBBS); Tan Tock Seng
Enhanced surveillance and contact tracing is essential to minimise the risk of widespread transmission in the Hospital, Singapore (B E Young,
community. Prof Y-S Leo, D C Lye); Saw Swee
Hock School of Public Health,
Singapore (M I-C Chen,
Funding None. H E Clapham PhD, A R Cook PhD,
Prof Y-S Leo, V J M Lee); National
Copyright © 2020 Elsevier Ltd. All rights reserved. University of Singapore and
National University Health
System, Singapore (H E Clapham,
Introduction three linked to a tour group from China, a company A R Cook); Bioinformatics
On Dec 31, 2019, a cluster of viral pneumonia cases, conference, and a church. Institute, Agency for Science,
subsequently identified as coronavirus disease 2019 To contain the spread of COVID-19, several pertinent Technology and Research,
Singapore (S Maurer-Stroh PhD);
(COVID-19), was reported in Wuhan, China.1 Subsequent questions need to be addressed. What is the infectious
Department of Biological
reports suggested that community transmission had ness of cases? What are the settings and activities beyond Sciences, National University
occurred in Wuhan and Hubei province, leading to the family clusters where spread can occur? What measures of Singapore, Singapore
lockdown of Wuhan on Jan 23, 2020, and subsequently should be taken to improve surveillance and case- (S Maurer-Stroh); National
Public Health Laboratory,
other cities in Hubei province, to control COVID-19 detection? What measures can reduce disease spread?
National Centre for Infectious
spread.2,3 WHO declared a public health emergency To answer these questions, we report data for the first Diseases, Singapore
of international concern on Jan 30, 2020.4 As of three clusters of COVID-19 cases in Singapore, the (S Maurer-Stroh, T M Mak PhD,
March 6, 2020, 98 192 confirmed cases and 3380 deaths epidemiological and clinical investigations done to ascer L Cui PhD, R V T P Lin MBBS);
National Public Health and
were reported globally, including 17 481 cases and tain disease characteristics and exposure types, and
Epidemiology Unit, National
335 deaths from 88 regions or countries outside of summary statistics to characterise the incubation period Centre for Infectious Diseases,
mainland China.5 of severe acute respiratory syndrome coronavirus 2 Singapore (M P H S Toh MMed);
Singapore, a city-state in southeast Asia, developed case- (SARS-CoV-2) and the serial interval between transmis Lee Kong Chian School of
Medicine, Singapore
definitions, laboratory tests, and enhanced surveillance to sion pairs. Our findings will be important for countries
(Prof Y-S Leo, D C Lye,
detect affected individuals with COVID-19 early, to enable and cities to calibrate detection and response efforts B E Young); and Yong Loo Lin
containment of the disease. Singapore confirmed its first during the ongoing epidemic. School of Medicine, Singapore
imported case of COVID-19 from Wuhan on Jan 23, 2020.6 (Prof Y-S Leo, D C Lye)
With the lockdown of Wuhan, inbound flights from Methods Correspondence to:
Dr Vernon J M Lee,
Wuhan to Singapore had ceased since Jan 23, 2020. As of Study design
Communicable Diseases Division,
Feb 22, 2020, 89 people in Singapore were confirmed to Since Jan 2, 2020, the Ministry of Health in Singapore Ministry of Health,
have COVID-19, and the first 18 affected individuals has been refining local case-definitions for people Singapore 169852
all reported recent travel to Wuhan. Singapore iden suspected of having COVID-19 (appendix p 4). Doctors vernon_lee@moh.gov.sg
tified several local clusters of COVID-19, with the first are required by law to notify the Ministry of Health of or
www.thelancet.com Vol 395 March 28, 2020 1039
Articles
Dr Barnaby E Young, National
Centre for Infectious Diseases, Research in context
Singapore 308442
barnaby_young@ncid.sg Evidence before this study beyond household clusters. Importation and limited local
See Online for appendix We searched PubMed up to Feb 15, 2020 for reports published transmission of SARS-CoV-2 could have occurred before the
in English with no date limitations using the keywords lockdown of Wuhan and China’s institution of travel restrictions.
“COVID-19” and “cluster”. A family cluster of coronavirus
Implications of all the available evidence
disease 2019 (COVID-19) was reported in Shenzhen,
Countries should focus on enhancing detection and
Guangdong. Transmission of severe acute respiratory syndrome
containment of local clusters of COVID-19, through surveillance
coronavirus 2 (SARS-CoV-2) has also been reported among
of individuals with general pneumonia or influenza-like
co-workers in Germany.
illnesses, and of people who have been in contact with unwell
Added value of this study travellers from China. It is also important for countries to do
We analysed three clusters of COVID-19 in Singapore to assess active case-finding among close contacts of affected
interactions and possible modes of transmission. Our findings individuals, including contacts with mild symptoms, to contain
show that SARS-CoV-2 is transmissible in community settings clusters and stop them from spreading.
cases of COVID-19.7 Further, Singapore implemented COVID-19, either at home or at designated government
enhanced surveillance on Jan 31, 2020, to test for quarantine facilities. We monitored their health status
COVID-19 among patients in intensive care units and daily; people who developed symptoms were conveyed in
people who died of unknown cause, all people with dedicated ambulances to hospital for isolation and testing
pneumonia in hospitals, and individuals with influenza- as part of active case-finding. We video-called individuals
like illness in sentinel primary-care clinics. Hospital- who were quarantined at home three times a day to verify
based doctors also have permission to test patients who their location; quarantine violators were tagged with a
they view with suspicion for clinical or epidemiological continuous tracking device. We placed other contacts
reasons. A confirmed case of COVID-19 is defined as (depending on risk stratification) on phone surveillance
an individual with a respiratory sample positive for or advised them to self-monitor and visit a primary-care
SARS-CoV-2, using a laboratory-based PCR test (appendix clinic if they became unwell.
p 1). Phylogenetic analysis is done of available viral
genomic sequences to ascertain genetic clustering. Clinical management
The Ministry of Health in Singapore identified the We isolated people with confirmed COVID-19 in indivi
first three clusters of COVID-19 cases on Feb 3, 2020, dual negative-pressure rooms with anterooms. We did
Feb 5, 2020, and Feb 8, 2020. All epidemiological inves blood investigations including a complete blood count,
tigations and outbreak containment measures were renal and liver function tests, and amounts of C-reactive
implemented under the Infectious Diseases Act,7 which protein and lactate dehydrogenase. Treatment was mainly
provides for use of data for analysis to control outbreaks. supportive; we started some patients on oral lopinavir
(400 mg) with ritonavir (100 mg) twice daily. We obtained
Epidemiological investigation clinical data for chronic medical illnesses, physical
We interviewed people with confirmed COVID-19 to obtain examinations, laboratory and radiological results, and
data for demographic characteristics, clinical symptoms, clinical progression and outcome from inpatient medical
and activity patterns, from 14 days preceding symptom records.
onset until isolation in hospital. We initiated contact tracing
to identify close contacts (ie, people who spend a prolonged Analysis of disease transmission data
time within 2 m of a confirmed case) and other contacts We reported the median (IQR) incubation period, defined
who had some interactions with the case. We asked people as the duration between estimated dates of infection and
For more on R see with confirmed COVID-19 about possible contact with reported symptom onset, using R. We reported the serial
https://www.R-project.org/ confirmed cases reported overseas in the 14 days before interval range between transmission pairs in the house-
symptom onset. We used open source information from hold cluster. We also calculated the probable number
other countries (including government websites), news of transmissions arising from each confirmed case of
aggregators (eg, ProMed), and media reports to identify COVID-19 by assuming that there was one unknown
secondary transmissions in the respective clusters. For primary case for each of the three clusters.
each cluster, we investigated the implicated setting to
ascertain potential interactions. We reviewed activity maps Role of the funding source
of other confirmed cases in Singapore to identify potential This study received no funding. The corresponding
epidemiological links to each cluster. authors had full access to all data in the study and had
We placed close contacts under quarantine for 14 days final responsibility for the decision to submit for
from last exposure to the individual with confirmed publication.
1040 www.thelancet.com Vol 395 March 28, 2020
Articles
Cluster A
Symptomatic cases Cases with unknown date of onset, Period from exposure to symptom onset Common exposure
Symptomatic cases (next generation) known date of laboratory confirmation Period from symptom onset to admission Home quarantine
Duration of date of (indirect) exposure Cases (next generation) with unknown Period from asymptomatic admission to symptom onset
to date of symptom onset or laboratory date of onset, known date of laboratory
confirmation confirmation
Duration of unknown date of exposure
to date of symptom onset or laboratory
confirmation
AC 48 years, female Asymptomatic at start of home
2 quarantine, conveyed to hospital
AC 40 years, female AC2 when unwell
3
AC 36 years, female
4 AC3
Home quarantine
A AC4
H1 44 years, female, domestic helper
Visit to shop
28 years, female, AC A 6 months,
wife of AH2 1 H3 male, son AH1
Visit to shop
A Household exposure
H2 45 years, male, husband of AC1 AH3
A AC1
GX 71 years, male
1 AH2
A
GX 35 years, female AGX1
2
AT 32 years, female, wife of AJ1 AGX2
1
AT1
AJ
1 39 years, male, husband of AT1 AJ1
Cluster B
Day 1: buffet lunch 1 h 15 min duration Day 2: breakout group session, 4 h duration
Day 1: Chinese banquet dinner, 3 h duration Day 2: teambuilding 2·5 h duration
Period from exposure to symptom onset Period from symptom onset to admission
(laboratory confirmation for cases diagnosed
overseas)
Day 3: workshop 3 h duration Period from unknown date of onset to known
Common exposure date of laboratory confirmation
BB 40 years, female, sister of B1
1 BB1
42 years, male, BB 65 years, female, Chinese new year gathering in Malaysia
Malaysian 2 mother-in-law of B1 Conference BB2
Exposure B1 B1
at
B2 38 years, male, Korean B2
conference
B3 36 years, male, Korean B3
B4 27 years, male, Singaporean B4
B5 38 years, female, Singaporean B5
B6 51 years, male, Singaporean B6
53 years, male, Holiday in France
B7 UK B7
Diagnosed in France
BB BB3–7
3–7 UK
BB UK Diagnosed in Spain
8 BB8
BB Diagnosed in UK
9–13 BB9–13
Cluster C
Period from exposure to symptom onset Common exposure
Period from symptom onset to admission
C1 56 years, male, husband of C2 traveller from Wuhan C1
C2 56 years, female, wife of C1 traveller from Wuhan C2
Visit to church
Visit to church
C3 53 years, male C3
C4 39 years, female C4
C5 52 years, female C5
Jan 8
Jan 9
20
Jan 1
22
Jan 3
24
Jan 5
26
Jan 7
Jan 8
Jan 9
Jan 0
Fe 1
b1
Fe 2
Fe 3
b4
Fe 5
b6
Fe 7
b8
Fe 9
0
0
Jan 8
Jan 9
Jan 0
Jan 1
Jan 2
Jan 3
24
Jan 5
26
Jan 7
28
Jan 9
Jan 0
Fe 1
b1
Fe 2
Fe 3
b4
Fe 5
b6
Fe 7
b8
Fe 9
3
2
2
2
2
3
2
b1
2
2
1
1
2
2
b1
2
3
1
1
b
b
b
b
b
b
b
b
b
Jan
Jan
Fe
Jan
Jan
Fe
Fe
Jan
Jan
Fe
Jan
Fe
Fe
Fe
Jan
Jan
Fe
Date Date
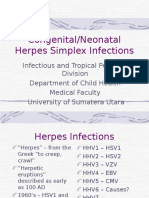
Figure 1: Timing of events and cases in three clusters of COVID-19 in Singapore
Age and sex are shown for each case (left panels), with other pertinent information (eg, relationship or nationality). Timeline of events (right panels); onset dates of symptomatic cases are shown,
when available. COVID-19=coronavirus disease 2019.
www.thelancet.com Vol 395 March 28, 2020 1041
Articles
Results Cluster A
Confirmed cases of COVID-19 The Ministry of Health in Singapore was alerted to
36 individuals were confirmed to have COVID-19, and two individuals with locally acquired COVID-19 on
these people were related to three local clusters, referred Feb 3, 2020 (AC1 and AC2; figure 1 upper panels). They
to as A (containing 11 people), B (consisting of 20 indivi did not fit the case-definition for suspected COVID-19 but
duals), and C (comprising five people; figure 1). Of these were tested because they reported frequent occupational
affected individuals, 17 tested positive for SARS-CoV-2 in contact with Chinese tourists. These two people were
Singapore, of whom only two (both from cluster C) had later identified to be linked epidemiologically to two other
recent travel history to China 14 days before onset of affected individuals (AGX1 and AGX2), a father and
symptoms (table). Two people from cluster A and 17 from daughter reported by official and media websites in
cluster B were reported by the health authorities of Guangxi, China,8–10 to be Chinese tourists who travelled
countries where they resided or travelled to. to Singapore on Jan 22, 2020, and who visited several
tourist sites on Jan 22–23, 2020, as part of a tour group.
AGX1 and AGX2 subsequently departed for Malaysia
Individuals (n=17)
before re-entry into Singapore for their flight to Guangxi
Age (years) 40 (36–51) on Jan 27, 2020, and they developed symptoms on
Gender Jan 28, 2020, after arrival in Guangxi. Details of the
Male 7 (41%) tour participants and the itinerary, obtained through
Female 10 (59%) the Singapore-based tour guide for the Singapore tour
Ethnic origin segment (AT1, who also tested positive for SARS-CoV-2)
Chinese 16 (94%) corroborated with details for AGX1 and AGX2 reported by
Other 1 (6%) Guangxi websites.
Nationality Of 20 tourists in the tour group from Guangxi, five or
Singaporean 13 (76%) six were reported by AT1 to be coughing during the
Chinese 3 (18%) tour. To the best of our knowledge, only AGX1 and AGX2
Indonesian 1 (6%) had laboratory-confirmed COVID-19 (positive PCR for
Cluster SARS-CoV-2).8 However, in view of the reported respira
A (tourist group from China and shopworkers) 9 (53%) tory symptoms among tour group participants, it is
B (company conference) 3 (18%) possible that other tour group members were the primary
C (church) 5 (29%) cases.
Chronic illness Among the places visited by the tour group in Singapore
Yes* 3 (18%) were a complementary health products shop and a
No 14 (82%)
jewellery shop; both shops are patronised frequently by
Travel to China in past 14 days
Chinese tour groups. The visits to the complementary
Yes 2 (12%)
health products shop lasted approximately 30 min,
No 15 (88%)
and the visit to the jewellery shop lasted roughly 1 h.
Four assistants in the complementary health products
Symptoms
shop (AC1, AC2, AC3, and AC4) and one assistant in the
Fever 15 (88%)
jewellery shop (AJ1) were identified to have COVID-19.
Cough 14 (82%)
All five shop assistants were at work on the day the tour
Sore throat 8 (47%)
group from Guangxi visited. AC1, AC2, AC3, and AC4
Shortness of breath 6 (35%)
reported that they would assist customers to apply sam
Myalgia 5 (29%)
ples of medicinal oil on their bodies, and handwashing
Diarrhoea 4 (24%)
was not usually done between customers. Three secondary
Chest pain 3 (18%)
transmission cases were identified in the household of
Runny nose 1 (6%)
AC1 (AH1, AH2, and AH3), none of whom were contacts
Nausea or vomiting 1 (6%)
of other cases.
Chest radiography findings on admission† For the cases who were confirmed on or before
Present 8 (53%) Feb 5, 2020, 179 close contacts who were in Singapore and
Absent 7 (47%) contactable were placed under quarantine, of whom two
Interval between symptom onset and 4 (3–9) close contacts (AC3 and AC4) subsequently reported to be
hospitalisation (days)
unwell and tested positive for SARS-CoV-2. An additional
Data are median (IQR) or n (%). SARS-CoV-2=severe acute respiratory syndrome six close contacts were quarantined. For active surveillance,
coronavirus 2. *Allergic rhinitis (n=1), hypertension (n=1), and cervical
spondylosis (n=1). †Data available for 15 individuals.
16 shop assistants at the complementary health products
shop and the sole remaining uninfected household
Table: Demographic, clinical, and radiological characteristics of
member of AC1, who were all asymptomatic, were tested
individuals who tested positive for SARS-CoV-2 in Singapore
and none were positive for SARS-CoV-2.
1042 www.thelancet.com Vol 395 March 28, 2020
Articles
Viral genomic sequences were available for four cases church on Jan 19, 2020. C5 was identified through active
(AH1, AH2, AH3, and AT1) and phylogenetic analysis case-finding. Two other people with COVID-19 were
confirmed their linkage, as suggested by the epide subsequently linked to this cluster (C1 and C2, who are
miological data (appendix pp 2–3). husband and wife). These individuals were Chinese
nationals from Wuhan who arrived in Singapore on
Cluster B Jan 19, 2020. Re-interviews with C1 and C2 found they
On Feb 4, 2020, Malaysia confirmed a case of COVID-19 had also visited the church on the same day. All
in an individual (B1) who had recent travel history to five people were asymptomatic during the church visit
Singapore on Jan 16–23, 2020, for a company confer (figure 1 lower panels).
ence (a closed business meeting for employees from The church is an independent church that occasionally
company branches globally), which was attended by at receives a few visitors from China at the Mandarin
least 111 participants from 19 different countries on service conducted every Sunday.11 Although C1 and C2
Jan 20–22, 2020. 17 attendees at the conference were were not church members, they attended the 2-h
from mainland China and at least one was from Wuhan. morning service when they travelled to Singapore. They
Subsequently, six participants at the conference who left immediately after the service and did not report
had no recent travel history to China (B2, B3, B4, B5, having lunch at the church. Based on closed-circuit
B6, and B7) tested positive for SARS-CoV-2 (figure 1 camera findings, C5 occupied the same seat as did cases
middle panels). Two affected individuals from Singapore C1 and C2 at the prayer meeting after the morning
were identified through contact tracing of participants service, but they did not recall meeting each other.
after notification from the Malaysian International Among the 227 regular church members, 191 members
Health Regulation (IHR) focal point. were contacted, of whom 142 attended the church on
The conference programme included business presen Jan 19, 2020. Of these people, only two had travel history
tations, workshops, breakout discussions, a welcome to Guangdong, China, 14 days before Jan 19, 2020;
reception and meals, team-building games, and a both reported being well. Six were unwell and referred
Singapore city bus tour. Seating arrangements (where for further management and none tested positive for
available) for the conference, and interviews with SARS-CoV-2. 93 close contacts were placed under quar
affected individuals, indicated close interactions between antine.
cases. Two groups (B1 and B3, and B4 and B7) were No additional cases linked to any of the three clusters
seated at the same tables for a 3-h Chinese banquet-style were identified as of Feb 14, 2020.
dinner on Jan 20, 2020, with three and two attendees
from China, respectively. Four cases (B1, B3, B4, and B5) Analysis of disease transmission data
were in a 4-h breakout session on Jan 21, 2020, with Although we were unable to identify the primary case or
41 other participants, including ten from China, of cases in each cluster with certainty, in cluster A, the cases
whom three had dined with B1 and B3 or B4 and B7 at
the Chinese banquet. Furthermore, the team-building
games entailed close physical contact. 10 Individual data
With initial news of B1, 15 conference participants Median (IQR)
remaining in Singapore were contacted to find out about 9
their health status. Four people reported being unwell
8
with fever, respiratory symptoms, or both and were
tested for SARS-CoV-2; two individuals (B4 and B5) 7
tested positive for the virus. The third local case (B6)
was identified via activity mapping to have attended 6
the conference and had subsequent interactions with
Cases (n)
5
company staff. 153 close contacts were placed under
quarantine. Hotel staff were told to monitor their health 4
status, and none reported being unwell during the
conference or subsequently. 13 secondary cases of 3
COVID-19 were reported among family members of B1
in Malaysia and contacts of B7 in France. 2
1
Cluster C
The Ministry of Health in Singapore identified two people 0
from Singapore (C3 and C4), with no recent travel history 0 2 4 6 8 10 12
to China, who tested positive for SARS-CoV-2 from Time to onset (days)
enhanced pneumonia surveillance. Activity mapping Figure 2: Incubation periods for cases with known probable exposure times
showed that both individuals had visited the same Median (IQR) time to onset was 4 days (IQR 3–6).
www.thelancet.com Vol 395 March 28, 2020 1043
Articles
35 Cluster A few days. Hospital admission was prolonged because of
Cluster B 100 persistently positive SARS-CoV-2 PCR from nasopha
Cluster C
30
Unknown
ryngeal swab testing (median 6 days, range 3–9). One
individual needed supplemental oxygen via nasal prongs
Cumulative transmission (%)
Cumulative 80
25
transmission and another two developed acute respiratory distress
20 60 requiring intubation and intensive care. Four indivi
Cases (n)
duals received experimental treatment of lopinavir with
15
40 ritonavir. No deaths were recorded in these three clusters
10 as of March 7, 2020.
20
5 Discussion
We report three clusters showing local transmission of
0 0
0 2 4 6 8 10 COVID-19 in Singapore. The three clusters involved a
Transmissions per case (n)
Chinese tour group, company conference, and a church
Figure 3: Probable secondary cases arising from each COVID-19 case and show the transmissibility of COVID-19 in community
COVID-19=coronavirus disease 2019. settings beyond household clusters. A household cluster
was previously reported in Shenzhen, Guangdong, China.12
in the two shops and the tour guide had inter-related These findings have implications for public-health mea
interactions with the Guangxi tour group in which sures and outbreak investigations that other countries
two cases were found. Exposures of the shop assistants might consider to detect and contain transmission.
were assumed to occur on Jan 23, 2020, and the tour guide The first indication of human-to-human transmission
on Jan 22, 2020, or Jan 23, 2020. In cluster C, the only in Singapore was detected 11 days after confirmation of
overlap in activities was on Jan 19, 2020, when all five the first imported case. China imposed a lockdown of
cases visited the church and exposures most likely Wuhan on Jan 23, 2020, and suspended all outgoing tour
occurred. For cluster B, we used information on reported groups beginning Jan 27, 2020. Despite these measures,
activities to infer most likely infection times within the local clusters were subsequently identified in Singapore,
meeting. Excluding the household cluster, we had infor with probable links to travellers from China before the
mation on both estimated infection time and reported measures to curb travel were implemented. Although the
date of symptom onset for 19 people. The incubation primary case or cases in all three clusters cannot be
periods are plotted in figure 2. The median incubation conclusively identified, they are postulated to be tourists
period was 4 days (IQR 3–6). Without accounting for or business visitors from China. The tour group impli
potential tertiary transmission within the household cated in cluster A originated from Guangxi at a time
(infected by a case who was not the primary case), the when relatively few cases had been reported in that
serial interval for the three transmission pairs in the region of China.13 Temperature screening for inbound
household cluster ranged between 3 days and 8 days. travellers on flights from Wuhan was implemented in
Assuming one unknown primary case seeded the Singapore on Jan 3, 2020, and expanded to all flights
outbreaks in each cluster, we noted that 31% of trans from China on Jan 22, 2020. Nonetheless, it is
mission pairs were associated with one individual (B7), unlikely that these primary cases could be identified by
and 32 observed cases had no onward transmission temperature screening, because there was no indication
(figure 3). that they were febrile on arrival.
Therefore, it is important that countries, particularly
Clinical findings those with a high travel volume from China, enhance
Of 17 locally confirmed cases, fever and cough were their surveillance system to identify local cases, not
the two most common symptoms, reported in 15 (88%) merely among people with a travel history to China
and 14 (82%) individuals, respectively (table). One case, because cases could be present in the community. The
a 6-month old male infant, was asymptomatic until local cases in cluster C were identified through enhanced
one spike of fever 2 days into hospital admission. pneumonia surveillance of people who had no history of
Pulmonary opacities were reported on chest radiography travel to China, whereas the initial cases in cluster A were
at admission in eight (53%) individuals, and developed identified because of heightened suspicion by health-care
over the course of admission in four additional people. workers, leading to testing. Among the first 84 confirmed
Lymphopenia (<1·1 ×
10⁹ cells per L) was seen in cases in Singapore, ten were detected by enhanced pneu
six people and thrombocytopenia (<150 × 10⁹ cells per L) monia surveillance and testing of patients in intensive
in four individuals over the course of admission. Median care units, and another eight affected individuals were
time from symptom onset to hospital admission was detected based on doctors’ discretion to test patients
4 days (IQR 3–9). whom they viewed with suspicion for clinical or epidemio
The clinical course was uncomplicated for most logical reasons. Such surveillance systems are, therefore,
individuals, with resolution of symptoms over the first important to identify cases in the commu nity who
1044 www.thelancet.com Vol 395 March 28, 2020
Articles
would be missed if the focus were only on travellers, and symptom-onset dates and the movement of and exposure
they have enabled prompt investigation and containment history of cases detected overseas were either based on
measures. Furthermore, with swift response in contact media reports or were unknown. Based on symptom-
tracing and quarantine of close contacts, two close onset dates of 17 local cases, the median incubation
contacts developed symptoms and were confirmed to period (4 days) corroborates other published findings.16,17
be infected with SARS-CoV-2 during their period of Although there is interest on asymptomatic transmission,
quarantine, ensuring no further onward transmission of we are unable to address this point in our study, and
the virus. Only two of 425 close contacts identified by further studies should be done to better understand
contact tracing developed COVID-19 (ie, most cases disease transmissibility of asymptomatic cases.
identified in the clusters did not transmit the SARS-CoV-2 In conclusion, as importation and local transmission
virus to their close contacts), raising the hypothesis that could have occurred in other countries before the
a few spreading events can result in clusters of trans lockdown of Wuhan and institution of travel restrictions
mission, whereas for most cases, transmission ended. by China, local clusters outside China can be expected
The ease of international travel makes containment and efforts should be focused on surveillance for locally
difficult. Cluster B was identified because of sharing of acquired cases and containment efforts to prevent wide
case data in Malaysia through the IHR focal point, spread community transmission. It is important for
and Singapore shared information on attendees at the countries to do active case-finding among close contacts
company conference to respective IHR focal points of cases to prevent clusters from spreading.
where participants at the conference had originated. Contributors
This work led to early identification of cases globally and RP, CJC, BEY, and SC contributed to the literature search, data collection,
highlights the importance of international cooperation data analysis, and writing of the report. HEC and ARC contributed to the
data analysis on disease transmission and figures. SM-S, TMM, LC and
and sharing of information under IHR to aid in active RVTPL contributed to the laboratory testing and analysis. MPHST, CP,
case-finding and containment. ML, JL, and VTJK contributed to the epidemiological data collection and
The cases of COVID-19 in these three clusters are analysis. MI-CC, DH, Y-SL and DCL contributed to the study design and
probably attributable to close or prolonged interactions. writing of the report. VJML contributed to study design, the literature
search, data collection, data analysis, and writing of the report. All authors
Direct physical contact was reported between shop assis read and approved the final report.
tants and tourists at the health products shop (cluster A).
Singapore 2019 Novel Coronavirus Outbreak Research Team
Handshaking and physical contact during team-building Kai-qian Kam, Shirin Kalimuddin, Seow Yen Tan, Jiashen Loh,
activities and sharing of meals were reported among Koh Cheng Thoon, Shawn Vasoo, Wei Xin Khong, Nur-Afidah Suhaimi,
participants of the business meeting (cluster B).14 There Sherlynn J H Chan, Emma Zhang, Olivia Oh, Albert Ty, Charlene Tow,
fore, direct transmission could be possible by contact or Yi Xian Chua, Wei Liang Chaw, Yixiang Ng, Farid Abdul-Rahman,
Shafiq Sahib, Zheng Zhao, Cheryl Tang, Constance Low, Ee Hui Goh,
indirect transmission (eg, via fomites and shared food). We Georgina Lim, Yan’an Hou, Imran Roshan, James Tan, Kelly Foo,
have shown environmental contamination of common- Khine Nandar, Lalitha Kurupatham, Pei Pei Chan, Pream Raj, Yijun Lin,
touch surfaces in the isolation room of a confirmed case.15 Zubaidah Said, Anne Lee, Cherie See, Jessey Markose, Joanna Tan,
This find ing highlights the importance of emphasising Guanhao Chan, Wanhan See, Xinyi Peh, Vincent Cai, Wen Kai Chen,
Zongbin Li, Roy Soo, Angela L P Chow, Wycliffe Wei, Aysha Farwin,
personal and hand hygiene as a key public-health message and Li Wei Ang.
that countries should adopt.
Declaration of interests
Recall bias could affect the accuracy of symptom-onset We declare no competing interests.
dates reported by cases. In cluster A, the date of onset of
References
symptoms for AC2 was uncertain because the individual 1 Wuhan Municipal Health Commission. Report on current
only sought primary-care treatment on Jan 30, 2020, pneumonia epidemic situation in the city (in Chinese). Dec 31, 2019.
http://wjw.wuhan.gov.cn/front/web/showDetail/2019123108989
7 days after reported onset of symptoms. Other exposures (accessed Feb 29, 2020).
are plausible. AC2 reported having symptoms on the day 2 The State Council, People’s Republic of China. Wuhan novel
of the tour group’s arrival, and we could postulate that coronavirus prevention and control command notice (no 1)
(in Chinese). Jan 23, 2020. http://www.gov.cn/xinwen/2020-01/23/
AC2 acquired infection from other tourists before content_5471751.htm (accessed Feb 29, 2020).
Jan 23, 2020, and seeded infections among colleagues, 3 DW.com. Wuhan pneumonia virus continues to spread,
the tour guide, and the two people from Guangxi on Hubei orders 15 cities to be closed (in Chinese). Jan 24, 2020.
Jan 23, 2020. However, case AJ1 had no interactions with https://www.dw.com/zh/a-52132769 (accessed Feb 29, 2020).
4 World Health Organization. Statement on the second meeting of
AC2, unless AC2 acquired infection serendipitously at a the International Health Regulations (2005) Emergency
similar time, independently. Similarly, in cluster C, Committee regarding the outbreak of novel coronavirus
C1 did not report symptoms until 5 days and C2 until (2019-nCoV). Jan 30, 2020. https://www.who.int/news-room/
detail/30-01-2020-statement-on-the-second-meeting-of-the-
3 days, after attending church, and this difference could international-health-regulations-(2005)-emergency-committee-
be attributable to recall bias of symptom-onset dates, regarding-the-outbreak-of-novel-coronavirus-(2019-ncov) (accessed
Feb 29, 2020).
particularly if symptoms were mild.
5 World Health Organization. Coronavirus disease 2019 (COVID-2019):
Other study limitations include the small sample size situation report—33. Feb 22, 2020. https://www.who.int/docs/
used to ascertain the incubation period, because primary default-source/coronaviruse/situation-reports/20200222-sitrep-
33-covid-19.pdf (accessed Feb 29, 2020).
cases could not be identified with certainty. Moreover,
www.thelancet.com Vol 395 March 28, 2020 1045
Articles
6 Ministry of Health, Singapore. Confirmed imported case of novel 12 Chan JF-W, Yuan S, Kok K-H, et al. A familial cluster of pneumonia
coronavirus infection in Singapore; multi-ministry taskforce ramps associated with the 2019 novel coronavirus indicating person-to-person
up precautionary measures. Jan 23, 2020. https://www.moh.gov.sg/ transmission: a study of a family cluster. Lancet 2020; 395: 514–23.
news-highlights/details/confirmed-imported-case-of-novel- 13 World Health Organization. Novel coronavirus (2019-nCoV):
coronavirus-infection-in-singapore-multi-ministry-taskforce-ramps- situation report—3. Jan 23, 2020. https://www.who.int/docs/
up-precautionary-measures (accessed Feb 29, 2020). default-source/coronaviruse/situation-reports/20200123-sitrep-3-
7 Singapore Statutes Online. Infectious Diseases Act, chapter 137. 2019-ncov.pdf (accessed Feb 29, 2020).
July 31, 2003. https://sso.agc.gov.sg/Act/IDA1976 (accessed 14 Channel NewsAsia. 3 new coronavirus cases in South Korea;
Feb 29, 2020). 2 men had travelled to Singapore for conference. Feb 5, 2020.
8 People’s Government of Guangxi Zhuang Autonomous Region. https://www.channelnewsasia.com/news/asia/wuhan-virus-
Emergency notice to find contacts of confirmed cases (in Chinese). coronavirus-south-korea-cases-12394934 (accessed Feb 29, 2020).
Feb 3, 2020. http://m.gxzf.gov.cn/gxyw/20200203-793378.shtml 15 Ong SWX, Tan YK, Chia PY, et al. Air, surface environmental,
(accessed Feb 29, 2020). and personal protective equipment contamination by severe acute
9 Yulin News. 8 confirmed cases in Yulin City are in stable condition respiratory syndrome coronavirus 2 (SARS-CoV-2) from a
(in Chinese). Feb 3, 2020. http://m.gxylnews.com/html/ symptomatic patient. JAMA 2020; published online March 4.
news/2020/02/189458.html (accessed Feb 29, 2020). DOI:10.1001/jama.2020.3227.
10 Guangxi News Network. 2 new cases of pneumonia confirmed by 16 Backer JA, Klinkenberg D, Wallinga J. Incubation period of 2019
new coronavirus infection in Yulin, a total of 7 cases (in Chinese). novel coronavirus (2019-nCoV) infections among travellers from
Feb 2, 2020. https://v.gxnews.com.cn/a/19225623 (accessed Wuhan, China, 20–28 January 2020. Euro Surveill 2020; 25: 2000062.
Feb 29, 2020). 17 Lauer SA, Grantz KH, Bi Q, et al. The incubation period of
11 The Life Church and Missions. About the church (in Chinese). 2019-nCoV from publicly reported confirmed cases: estimation and
http://www.lifechurchmissions.com/ChurchHistory.aspx (accessed application. Feb 4, 2020. https://www.medrxiv.org/content/10.1101/
Feb 29, 2020). 2020.02.02.20020016v1 (accessed Feb 29, 2020).
1046 www.thelancet.com Vol 395 March 28, 2020
You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Eng4 - MELC Q1 - 2 Use Resources Such As A Dictionary, Thesaurus, Online Resources To Find The Meaning of WordsDocument5 pagesEng4 - MELC Q1 - 2 Use Resources Such As A Dictionary, Thesaurus, Online Resources To Find The Meaning of WordsYtsej OganapegNo ratings yet
- Zoonotic Diseases Fact SheetDocument7 pagesZoonotic Diseases Fact SheetEightch PeasNo ratings yet
- Polio by DorothyShepherdDocument3 pagesPolio by DorothyShepherdMiranda Castro Homeopathy100% (1)
- Free GRE Practice Test - 100+ GRE Sample TestsDocument7 pagesFree GRE Practice Test - 100+ GRE Sample TestsPrajwal Praj GNo ratings yet
- A Case Study of Dengue FeverDocument19 pagesA Case Study of Dengue FeverDanny Shrestha100% (1)
- Hepatitis B - DOLEDocument23 pagesHepatitis B - DOLEMary Rose VirtucioNo ratings yet
- Cholera and SalmonellaDocument5 pagesCholera and SalmonellaJonas Marvin Anaque100% (1)
- Jurnal MaternitasDocument11 pagesJurnal MaternitasEndyNo ratings yet
- Expanded Program For ImmunizationDocument23 pagesExpanded Program For ImmunizationJustine Marie AguilarNo ratings yet
- C1 Research Paper FinalDocument10 pagesC1 Research Paper FinalDylan OrtalezaNo ratings yet
- Treatment Guidelines GonorrheaDocument1 pageTreatment Guidelines GonorrheaJoe DettNo ratings yet
- Skripsi Tanpa Bab PembahasanDocument61 pagesSkripsi Tanpa Bab Pembahasanrouf fadil mahmudNo ratings yet
- COLD and FLUDocument44 pagesCOLD and FLUZulaikha ChalkiNo ratings yet
- Clinical Microbiology Laboratory Test RequisitionDocument1 pageClinical Microbiology Laboratory Test RequisitionRhodjane Dela Cruz0% (1)
- One Word Answer Questions Covering DermatologyDocument5 pagesOne Word Answer Questions Covering DermatologyFan Eli50% (2)
- 4a Sickness and Illness PolicyDocument2 pages4a Sickness and Illness PolicyAlina SimionNo ratings yet
- Chest X-Ray Appearances in Pneumonia and BronchiolitisDocument7 pagesChest X-Ray Appearances in Pneumonia and BronchiolitisMariani AniNo ratings yet
- Samenvatting Infectie en InflammatieDocument169 pagesSamenvatting Infectie en InflammatiejeskevandiemenNo ratings yet
- WTM Ticket EBadgeDocument1 pageWTM Ticket EBadgeSmarttNo ratings yet
- A Curious Guide For Courageous Kids Coronavirus DigitalDocument14 pagesA Curious Guide For Courageous Kids Coronavirus Digitalmanal salehNo ratings yet
- Flow Chart Covid-19-Guidance-QuarantineDocument3 pagesFlow Chart Covid-19-Guidance-Quarantineapi-261360994No ratings yet
- Guidelines For PMTCT of HIVAIDS in Kenya-1Document82 pagesGuidelines For PMTCT of HIVAIDS in Kenya-1Simon Wanjiru100% (1)
- Case Study of MicrobiologyDocument4 pagesCase Study of MicrobiologyQaisrani Y9No ratings yet
- 2020 Status Report As of August 31, 2021Document192 pages2020 Status Report As of August 31, 2021Jasper Kenneth PeraltaNo ratings yet
- Hiv VaccinationsDocument5 pagesHiv Vaccinationsblueivy66No ratings yet
- 8258 ID Mengembangkan Evidence Based Public Health Ebph Hiv Dan Aids Berbasis SurveilansDocument8 pages8258 ID Mengembangkan Evidence Based Public Health Ebph Hiv Dan Aids Berbasis SurveilansDamiri100% (1)
- Cepheid GeneXpert System Menu Flyer CE IVD 0293 EnglishDocument2 pagesCepheid GeneXpert System Menu Flyer CE IVD 0293 EnglishJohn KatabasasaNo ratings yet
- Update AnnouncementICTROMIDocument19 pagesUpdate AnnouncementICTROMIPrima ExpeNo ratings yet
- K28 B Congenital HSV KBKDocument25 pagesK28 B Congenital HSV KBKLa Lydia TampubolonNo ratings yet
- Seminar Presentation Plus Ultra 10%Document10 pagesSeminar Presentation Plus Ultra 10%Adaeze Ezem-NjokuNo ratings yet