You might also like
- Comunity Pharmacy Introduction ModDocument42 pagesComunity Pharmacy Introduction Modhumag143No ratings yet
- Vascular Ultrasound Protocol Guide PDFDocument28 pagesVascular Ultrasound Protocol Guide PDFchica_as100% (2)
- Biology Investigatory ProjectDocument21 pagesBiology Investigatory ProjectCrazy about Jungles87% (30)
- Tapas Acupressure Technique 39831 23492Document27 pagesTapas Acupressure Technique 39831 23492Glo Aleman100% (2)
- Adrenocorticosteroids & Adrenocortical AntagonistsDocument20 pagesAdrenocorticosteroids & Adrenocortical Antagonistsapi-3859918No ratings yet
- Mechanisms and Mechanical DevicesDocument10 pagesMechanisms and Mechanical Devicesoana_avram50% (4)
- Endotracheal Intubation GuideDocument4 pagesEndotracheal Intubation Guiderupali gahalianNo ratings yet
- 17 - OET Online Test 4Document20 pages17 - OET Online Test 4Abdullah Mohammad Ibne Haider100% (1)
- Rle Isolation WardDocument6 pagesRle Isolation WardJinaan MahmudNo ratings yet
- Sustainable Building Design For Tropical Climates - 1 PDFDocument427 pagesSustainable Building Design For Tropical Climates - 1 PDFAndré Nery FigueiredoNo ratings yet
- Using Face Masks in The Community: Scope of This DocumentDocument6 pagesUsing Face Masks in The Community: Scope of This Documentathanasios_syrakisNo ratings yet
- Rubio Romero 2020 Disposable Masks Disinfection and SDocument11 pagesRubio Romero 2020 Disposable Masks Disinfection and SdaruNo ratings yet
- MainDocument4 pagesMainAdel AdielaNo ratings yet
- COVID-19 - Prevention and Control Measures in CommunityDocument8 pagesCOVID-19 - Prevention and Control Measures in Communitykadoxe1682No ratings yet
- Pediatria en PandemiaDocument8 pagesPediatria en PandemiaMichellalvarez150No ratings yet
- Intensive Care Unit Setup For COVID-19Document10 pagesIntensive Care Unit Setup For COVID-19BAGUIO CATSNo ratings yet
- Intensive Care Unit Setup For COVID-19Document7 pagesIntensive Care Unit Setup For COVID-19BAGUIO CATSNo ratings yet
- Hospital Infection Control Committee AIIMS, New DelhiDocument25 pagesHospital Infection Control Committee AIIMS, New DelhiRoma ThaiNo ratings yet
- Rational Use of Personal Protective Equipment (PPE) For Coronavirus Disease (COVID-19)Document9 pagesRational Use of Personal Protective Equipment (PPE) For Coronavirus Disease (COVID-19)Karthick AnbuNo ratings yet
- The Utilization of Protective Face Masks Among Polish Healthcare Workers During COVID-19 Pandemic: Do We Pass The Exam?Document10 pagesThe Utilization of Protective Face Masks Among Polish Healthcare Workers During COVID-19 Pandemic: Do We Pass The Exam?Luis-alfredo Perez Bolde HernandezNo ratings yet
- COVID-19 - Infection Control For Persons With SARS-CoV-2 Infection - UpToDateDocument35 pagesCOVID-19 - Infection Control For Persons With SARS-CoV-2 Infection - UpToDateDuy Hùng HoàngNo ratings yet
- Protect Yourself from COVID-19 with Masks and Hygiene (NCDCDocument4 pagesProtect Yourself from COVID-19 with Masks and Hygiene (NCDCJideNo ratings yet
- 2021 ECDC - Using Face Masks in The Community First UpdateDocument31 pages2021 ECDC - Using Face Masks in The Community First UpdateHandy NugrohoNo ratings yet
- An Evidence Review of Face Masks Against Covid-19Document7 pagesAn Evidence Review of Face Masks Against Covid-19IJRASETPublicationsNo ratings yet
- 3945 13062 1 PBDocument5 pages3945 13062 1 PBEltohn JohnNo ratings yet
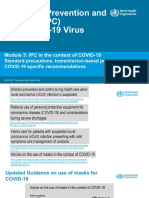
- WHO IPC COVID FINAL.15.03.20.V2 Module3-MinDocument72 pagesWHO IPC COVID FINAL.15.03.20.V2 Module3-MinT Bishop LouisNo ratings yet
- Assignment 3: Research Methodology Hafsa 20l-2506Document3 pagesAssignment 3: Research Methodology Hafsa 20l-2506Hafsa MehmoodNo ratings yet
- Assignment 3: Research Methodology Hafsa 20l-2506Document3 pagesAssignment 3: Research Methodology Hafsa 20l-2506Hafsa MehmoodNo ratings yet
- Infection Control Expert Group: The Use of Face Masks and Respirators in The Context of Covid-19Document24 pagesInfection Control Expert Group: The Use of Face Masks and Respirators in The Context of Covid-19Karen MooreNo ratings yet
- COVID 19 and Dentistry A PerspectiveDocument12 pagesCOVID 19 and Dentistry A PerspectiveAthenaeum Scientific PublishersNo ratings yet
- Infection Prevention and Control and Preparedness For COVID-19 in Healthcare SettingsDocument20 pagesInfection Prevention and Control and Preparedness For COVID-19 in Healthcare SettingsMatthew DavisNo ratings yet
- A Scoping Review of Respirator Literature and A Survey Among Dental ProfessionalsDocument12 pagesA Scoping Review of Respirator Literature and A Survey Among Dental ProfessionalsHNiondiv EdvmpoeirmNo ratings yet
- Guidelines For Setting Up Private Clinic PDFDocument13 pagesGuidelines For Setting Up Private Clinic PDFAMEERDEENNo ratings yet
- A Discussion of The Effectiveness of PPE During The Covid 19 Pandemic Ruairi MooreDocument6 pagesA Discussion of The Effectiveness of PPE During The Covid 19 Pandemic Ruairi MooreAbdurrauf UsmanNo ratings yet
- Short BaseDocument7 pagesShort BaseSajin AlexanderNo ratings yet
- Disposable Over Reusable Face Masks: Public Safety or Environmental Disaster?Document10 pagesDisposable Over Reusable Face Masks: Public Safety or Environmental Disaster?Yaya HizmiNo ratings yet
- Disposable Over Reusable Face Masks: Public Safety or Environmental Disaster?Document10 pagesDisposable Over Reusable Face Masks: Public Safety or Environmental Disaster?Damelys Evelyn Fernandez PeñaNo ratings yet
- Seba Saqer - 20180482 Puplic HealthDocument10 pagesSeba Saqer - 20180482 Puplic HealthSaba SaqerNo ratings yet
- Coronavirus Disease 2019 (COVID-19) - Anesthetic Concerns, Including Airway Management and Infection ControlDocument32 pagesCoronavirus Disease 2019 (COVID-19) - Anesthetic Concerns, Including Airway Management and Infection ControlT GalenNo ratings yet
- Ophthalmic Complaints in Face Mask Wearing Prevalence Treatment and Prevention With A Potential Protective Effect Against SARS CoV 2Document14 pagesOphthalmic Complaints in Face Mask Wearing Prevalence Treatment and Prevention With A Potential Protective Effect Against SARS CoV 2Feli FelNo ratings yet
- Situation:: Nosocomial InfectionDocument4 pagesSituation:: Nosocomial InfectionMysviousNo ratings yet
- Face Mask Use Against Covid-19 Among Medical Students at Kampala International UniversityDocument14 pagesFace Mask Use Against Covid-19 Among Medical Students at Kampala International UniversityKIU PUBLICATION AND EXTENSIONNo ratings yet
- Naming The Coronavirus Disease (COVID-19) and The Virus That Causes ItDocument7 pagesNaming The Coronavirus Disease (COVID-19) and The Virus That Causes ItJay JayNo ratings yet
- COVID-19's Impact on Dental CareDocument49 pagesCOVID-19's Impact on Dental CareShubham PatelNo ratings yet
- Simple Economical Solution For Personal Protection Equipment (Face Mask/Shield) For Health Care Staff During COVID 19Document7 pagesSimple Economical Solution For Personal Protection Equipment (Face Mask/Shield) For Health Care Staff During COVID 19Neel PatelNo ratings yet
- DocumentDocument4 pagesDocumenttangaramariam566No ratings yet
- COVID-19: Occupational Health and Safety For Health Workers: Interim Guidance 2 February 2021Document16 pagesCOVID-19: Occupational Health and Safety For Health Workers: Interim Guidance 2 February 2021Rosiana AgustinNo ratings yet
- CODE OF PRACTICE FOR INFECTION CONTROLDocument23 pagesCODE OF PRACTICE FOR INFECTION CONTROLAnne TjanNo ratings yet
- PIIS0140673620311831Document2 pagesPIIS0140673620311831kayegi8666No ratings yet
- WHO 2019 Ncov IPC - Masks 2020.3 EngDocument5 pagesWHO 2019 Ncov IPC - Masks 2020.3 EngStephanie SommerfeldNo ratings yet
- Effectiveness of Fabric Mask in The Community PDFDocument9 pagesEffectiveness of Fabric Mask in The Community PDFshadijahNo ratings yet
- WHO Masks GuidelinesDocument5 pagesWHO Masks GuidelinesLarryDCurtisNo ratings yet
- Brote de COVID-19 en Italia Proteger La Salud de Los Trabajadores y La Respuesta de La Asociación Italiana de Higienistas IndustrialesDocument15 pagesBrote de COVID-19 en Italia Proteger La Salud de Los Trabajadores y La Respuesta de La Asociación Italiana de Higienistas IndustrialesChristian PinoNo ratings yet
- Etude Masque Covid 19Document22 pagesEtude Masque Covid 19youssouf DossoNo ratings yet
- Implimentation of Health and Safety ProtocolsDocument40 pagesImplimentation of Health and Safety ProtocolsFrancis Ivan PerezNo ratings yet
- Coronavirus Disease 2019 (COVID-19) Is AnDocument2 pagesCoronavirus Disease 2019 (COVID-19) Is AnSadhak AarushNo ratings yet
- Knowledge, and Practice Towards Infection Control Measures For The Novel Corona Virus Among Nurses Working at Isolation DepartmentDocument49 pagesKnowledge, and Practice Towards Infection Control Measures For The Novel Corona Virus Among Nurses Working at Isolation DepartmentOmima MuhammedNo ratings yet
- Environmental Campaign Against Covid-19Document11 pagesEnvironmental Campaign Against Covid-19joshuaNo ratings yet
- When to wear gloves and when not to during Covid 19Document7 pagesWhen to wear gloves and when not to during Covid 19damar soebandNo ratings yet
- Standard masks as effective as respirators for preventing COVID infectionDocument8 pagesStandard masks as effective as respirators for preventing COVID infectionsemabayNo ratings yet
- COVID-19 orthopaedic surgical protocolsDocument23 pagesCOVID-19 orthopaedic surgical protocolsDoctor's BettaNo ratings yet
- Presentation COVID-19 WHO enDocument12 pagesPresentation COVID-19 WHO enEtaferawNo ratings yet
- Supporting The Health Care Workforce During The COVID-19 Global EpidemicDocument2 pagesSupporting The Health Care Workforce During The COVID-19 Global EpidemicDema AlsouqiNo ratings yet
- Social Distancing Role of Smartphone During Coronavirus COVID19 Pandemic EraDocument9 pagesSocial Distancing Role of Smartphone During Coronavirus COVID19 Pandemic EraThobius JosephNo ratings yet
- Base CovidDocument10 pagesBase CovidSajin AlexanderNo ratings yet
- The Risk of COVID-19 Infection Among Healthcare WorkersDocument3 pagesThe Risk of COVID-19 Infection Among Healthcare WorkersIn House Training DialisisNo ratings yet
- Quality Assurance Project PlansDocument42 pagesQuality Assurance Project Plansoana_avramNo ratings yet
- Sophos SEO InsightsDocument15 pagesSophos SEO InsightstragantrasNo ratings yet
- IRA Required Minimum Distribution WorksheetDocument1 pageIRA Required Minimum Distribution Worksheetoana_avramNo ratings yet
- Tabel 20.04.2020 - Dispozitive Medicale Pentru Diagnostic in Vitro (Teste) Inregistrate in Uniunea EuropeanaDocument19 pagesTabel 20.04.2020 - Dispozitive Medicale Pentru Diagnostic in Vitro (Teste) Inregistrate in Uniunea Europeanaoana_avramNo ratings yet
- SEO Work Areas (1-6-20) - 202003030829404748 PDFDocument1 pageSEO Work Areas (1-6-20) - 202003030829404748 PDFoana_avramNo ratings yet
- Search Engine Land Periodic Table of SEODocument1 pageSearch Engine Land Periodic Table of SEOraineherreraNo ratings yet
- Reversible Building Design GuidelinesDocument22 pagesReversible Building Design Guidelinesoana_avramNo ratings yet
- Collaboration Integrated Information and The Project Lifecycle PDFDocument20 pagesCollaboration Integrated Information and The Project Lifecycle PDFoana_avramNo ratings yet
- DI and DII Worksheet PDFDocument2 pagesDI and DII Worksheet PDFoana_avramNo ratings yet
- Collaboration Integrated Information and The Project Lifecycle PDFDocument20 pagesCollaboration Integrated Information and The Project Lifecycle PDFoana_avramNo ratings yet
- CDG Building Design Guidelines PDFDocument48 pagesCDG Building Design Guidelines PDFoana_avramNo ratings yet
- Worksheets For Determaining Evacuation Capability PDFDocument5 pagesWorksheets For Determaining Evacuation Capability PDFoana_avramNo ratings yet
- SEO Work Areas (1-6-20) - 202003030829404748Document1 pageSEO Work Areas (1-6-20) - 202003030829404748oana_avramNo ratings yet
- Who Can Design What Type of Building in CaliforniaDocument1 pageWho Can Design What Type of Building in Californiaoana_avramNo ratings yet
- Search Engine Land Periodic Table of SEODocument1 pageSearch Engine Land Periodic Table of SEOraineherreraNo ratings yet
- CDG Building Design Guidelines PDFDocument48 pagesCDG Building Design Guidelines PDFoana_avramNo ratings yet
- Building Design Calculation WorksheetDocument1 pageBuilding Design Calculation Worksheetoana_avramNo ratings yet
- An Analysis of The Application of Selected SEO TechniquesDocument137 pagesAn Analysis of The Application of Selected SEO Techniquesoana_avramNo ratings yet
- DI and DII Worksheet PDFDocument2 pagesDI and DII Worksheet PDFoana_avramNo ratings yet
- Bird Friendly Building Guide - 2015Document60 pagesBird Friendly Building Guide - 2015oana_avramNo ratings yet
- What Is Search Engine Optimization: SEODocument7 pagesWhat Is Search Engine Optimization: SEOespinete2005No ratings yet
- Trusted Internet PDFDocument20 pagesTrusted Internet PDFoana_avram100% (1)
- Intuos-3 Users ManualDocument0 pagesIntuos-3 Users Manualshinigami_woodsNo ratings yet
- Iic Pub G1 V1.80 2017-01-31Document58 pagesIic Pub G1 V1.80 2017-01-31Pema Chentsho100% (1)
- Child Support Packet Includes FormsDocument66 pagesChild Support Packet Includes Formsoana_avramNo ratings yet
- Xpert Group1 Reference ArchitectureDocument107 pagesXpert Group1 Reference ArchitectureacaldereNo ratings yet
- Lecturer or Senior Lecturer Civil EngineeringDocument6 pagesLecturer or Senior Lecturer Civil Engineeringoana_avramNo ratings yet
- Function of Each GearsDocument6 pagesFunction of Each GearsRacco Roy0% (1)
- I. General ObjectiveDocument5 pagesI. General ObjectiveMr. BQNo ratings yet
- NCM 107 5M Case Analysis PDFDocument9 pagesNCM 107 5M Case Analysis PDFKisha BethelNo ratings yet
- 1 Historical OverviewDocument3 pages1 Historical OverviewClair de LuneNo ratings yet
- Metformin Drug StudyDocument2 pagesMetformin Drug StudyArone SebastianNo ratings yet
- Implant Retained Overdenture: Splint Approach Using Copy DenturesDocument9 pagesImplant Retained Overdenture: Splint Approach Using Copy DenturesSorabh JainNo ratings yet
- Acute Renal Failure-Step23C - 1Document28 pagesAcute Renal Failure-Step23C - 1DEBJIT SARKARNo ratings yet
- Cellular AberrationDocument6 pagesCellular Aberrationirene gomez100% (1)
- 1 - Abbasi Shaheed Hospital Overview-1Document3 pages1 - Abbasi Shaheed Hospital Overview-1Bushra MujeebNo ratings yet
- Hipofisis 7Document13 pagesHipofisis 7RafaelPetitNo ratings yet
- Midterm Worksheet ALHS 1090 AssignmentDocument13 pagesMidterm Worksheet ALHS 1090 AssignmentElijah HallNo ratings yet
- Pricelist SKINTIFIC Jakarta X Beauty II 14 - 17 Dec 2023Document1 pagePricelist SKINTIFIC Jakarta X Beauty II 14 - 17 Dec 2023ZakiyahNo ratings yet
- Clinical PortraitDocument6 pagesClinical PortraitDann Francis SarnilloNo ratings yet
- Martin Harris B. Brodsky MB Michel Y. Lee FS S. y Walters B. 2007. Inicio Tardio de La Deglucion Faringea Variabilidad Normal en Degluciones AdultasDocument11 pagesMartin Harris B. Brodsky MB Michel Y. Lee FS S. y Walters B. 2007. Inicio Tardio de La Deglucion Faringea Variabilidad Normal en Degluciones AdultasLucianaNo ratings yet
- Acute Chest Syndrome (ACS) CCGDocument11 pagesAcute Chest Syndrome (ACS) CCGJessa MaeNo ratings yet
- Hyper Pro Lac Tine MiaDocument47 pagesHyper Pro Lac Tine Miakharbosham100% (3)
- PG Addmision 2021Document3 pagesPG Addmision 2021Harpreet KaurNo ratings yet
- Management of The Urologic Sepsis SyndromeDocument10 pagesManagement of The Urologic Sepsis SyndromeNur Syamsiah MNo ratings yet
- Movement Disorders Movement DisordersDocument32 pagesMovement Disorders Movement Disordersreddyrajiv1526No ratings yet
- Cryptococcus NeoformansDocument10 pagesCryptococcus NeoformansArnab MullickNo ratings yet
- Predicting Neurofibromatosis Type 1 Risk Among Children With Isolated Cafe-Au-Lait MaculesDocument10 pagesPredicting Neurofibromatosis Type 1 Risk Among Children With Isolated Cafe-Au-Lait Maculeszulfan tmNo ratings yet
- Equilibrating SSC Guidelines With Individualized Care: Editorial Open AccessDocument4 pagesEquilibrating SSC Guidelines With Individualized Care: Editorial Open AccessJhon FerrerNo ratings yet
- Deepankar Tiwari - MBA HCM - Prof. Gita Sashidharan PDFDocument27 pagesDeepankar Tiwari - MBA HCM - Prof. Gita Sashidharan PDFAkshit BhutaniNo ratings yet