You might also like
- ArrhythmiaDocument2 pagesArrhythmiaChris Pritchard93% (30)
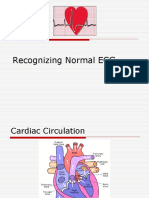
- Recognizing Normal ECGDocument50 pagesRecognizing Normal ECGJosiephine Bucalon100% (3)
- ECG Master Class-1Document132 pagesECG Master Class-1Shohag ID Center100% (1)
- Physical Therapy ProtocolsDocument852 pagesPhysical Therapy Protocolspickach83% (6)
- ECG Interpretation UnismaDocument178 pagesECG Interpretation UnismadefinaNo ratings yet
- EKG Interpretation: UNC Emergency Medicine Medical Student Lecture SeriesDocument58 pagesEKG Interpretation: UNC Emergency Medicine Medical Student Lecture SeriesHasnahdurrNo ratings yet
- Ekg Panum or OsceDocument69 pagesEkg Panum or OsceGladish RindraNo ratings yet
- Use of Vasopressors and Inotropes - UpToDateDocument18 pagesUse of Vasopressors and Inotropes - UpToDateAlbertoMarteNo ratings yet
- Ecg Interpretation New TemplateDocument88 pagesEcg Interpretation New TemplateJonathan NgNo ratings yet
- EKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookFrom EverandEKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookNo ratings yet
- 12 - Lead ECG-A Web Brain For Easy InterpretationDocument54 pages12 - Lead ECG-A Web Brain For Easy Interpretatione-kino3692100% (1)
- ECG TutorialDocument40 pagesECG TutorialAnonymous HAbhRTs2TfNo ratings yet
- Suatu Alat Laboratoris Alat Bantu DiagnosisDocument78 pagesSuatu Alat Laboratoris Alat Bantu DiagnosisMohammad AlmuhaiminNo ratings yet
- EKG Interpretation: UNS Cardiovascular Dept Medical Student Lecture SeriesDocument85 pagesEKG Interpretation: UNS Cardiovascular Dept Medical Student Lecture Seriesandina rosmalianti100% (1)
- This Document For Adult Patients Only. EKG Freq. 0.05-100 HZDocument1 pageThis Document For Adult Patients Only. EKG Freq. 0.05-100 HZLocke Helvet Laurie Kaicer100% (1)
- ECG InterpretationDocument83 pagesECG InterpretationJuana Maria Garcia Espinoza100% (2)
- ECG For InternsDocument31 pagesECG For InternsAgus SyaifudinNo ratings yet
- Suatu Alat Laboratoris Alat Bantu DiagnosisDocument78 pagesSuatu Alat Laboratoris Alat Bantu DiagnosisAnonymous 3LwVkUsdNo ratings yet
- Kuliah Ekg UnswagatiDocument75 pagesKuliah Ekg UnswagatiiikNo ratings yet
- Basics of ECG: DR Subroto Mandal, MD, DM, DC Associate Professor, CardiologyDocument206 pagesBasics of ECG: DR Subroto Mandal, MD, DM, DC Associate Professor, CardiologyRavi SharmaNo ratings yet
- Basic Ecg Reading - McuDocument63 pagesBasic Ecg Reading - McuJofandAndrea MendozaNo ratings yet
- Dr. Anas Yasin - MDDocument58 pagesDr. Anas Yasin - MDMahfouzNo ratings yet
- Basic of EcgDocument82 pagesBasic of Ecgpopescuioana1No ratings yet
- Ekg Normal Dan Acs Sudin TimurDocument59 pagesEkg Normal Dan Acs Sudin TimurArum MaharaniNo ratings yet
- Physiology CVS MCQ (Dr. Nassar)Document23 pagesPhysiology CVS MCQ (Dr. Nassar)زياد سعيدNo ratings yet
- Sally Aburumman Bushra SaleemDocument75 pagesSally Aburumman Bushra SaleemAbdulrahman AlsayyedNo ratings yet
- Anamnesis & PemfisDocument81 pagesAnamnesis & PemfisFikriYTNo ratings yet
- HEENT Focused Exam Soap NoteDocument5 pagesHEENT Focused Exam Soap Noteariel sparkmanNo ratings yet
- ECG Normal and AbnormalDocument74 pagesECG Normal and Abnormalawaniedream8391100% (1)
- Interpretasi EKGDocument81 pagesInterpretasi EKGGyna MarsianaNo ratings yet
- Approach To Pediatric ECGDocument5 pagesApproach To Pediatric ECGMateen ShukriNo ratings yet
- Essential Cardiac Electrophysiology: The Self-Assessment ApproachFrom EverandEssential Cardiac Electrophysiology: The Self-Assessment ApproachNo ratings yet
- ElectrocardiogramDocument52 pagesElectrocardiogramTuong HoangManhNo ratings yet
- Intraoperative Management of Shock in Adults - UpToDateDocument36 pagesIntraoperative Management of Shock in Adults - UpToDateYessica RivasNo ratings yet
- General and Unique Characteristics of The Different Organ Systems in Representative AnimalsDocument51 pagesGeneral and Unique Characteristics of The Different Organ Systems in Representative AnimalsAliah Jeonelle Ramos100% (2)
- Ecg Guidelines: Donna J. Castillo, MDDocument76 pagesEcg Guidelines: Donna J. Castillo, MDBheck Magat100% (1)
- Part 1-2023 (1st Version)Document19 pagesPart 1-2023 (1st Version)Waleed SofiNo ratings yet
- TestBank Lewis Medical Surgical Nursing 11th 2020.pdf-845-864Document20 pagesTestBank Lewis Medical Surgical Nursing 11th 2020.pdf-845-864هدوء النسمةNo ratings yet
- Ecg Presentation 2013Document40 pagesEcg Presentation 2013Samuel FpNo ratings yet
- Suatu Alat LaboratorisDocument78 pagesSuatu Alat LaboratorisHematology 2016No ratings yet
- Kursus Ekg DR Ismi-1Document78 pagesKursus Ekg DR Ismi-1Sekar Ayu WulandariNo ratings yet
- Dasar-Dasar EkgDocument67 pagesDasar-Dasar EkgIGD Kenak MedikaNo ratings yet
- ECG Lecture 4Document44 pagesECG Lecture 4asdasdasdasNo ratings yet
- Dasar-Dasar EKG - Dr. SatriaDocument67 pagesDasar-Dasar EKG - Dr. SatriaSuryadi P. Dwipayana, Ida BgsNo ratings yet
- Dasar Kursus EKG - DR ParwataDocument67 pagesDasar Kursus EKG - DR ParwataPuka Putra AdnyanaNo ratings yet
- ECG For BeginnersDocument61 pagesECG For Beginnersblndffl100% (2)
- Elektro Kardio Grafi - Dasar - : DR Eka Ginanjar, SPPDDocument105 pagesElektro Kardio Grafi - Dasar - : DR Eka Ginanjar, SPPDalmiraerickaiNo ratings yet
- EKG Primer2woEKGsDocument26 pagesEKG Primer2woEKGsDiana HyltonNo ratings yet
- ECG InterpretationDocument168 pagesECG InterpretationPavi YaskarthiNo ratings yet
- Ipd Kuliah Ekg Blok KegawatdaruratanDocument118 pagesIpd Kuliah Ekg Blok Kegawatdaruratansiti solikhaNo ratings yet
- Electrocardiograph Y: Dr. Fatimah Eliana, SPPD, Kemd, FinasimDocument118 pagesElectrocardiograph Y: Dr. Fatimah Eliana, SPPD, Kemd, FinasimTommy WidjayaNo ratings yet
- Electrocardiography-Blok Cardiorespi 1Document49 pagesElectrocardiography-Blok Cardiorespi 1ahmad syauqieNo ratings yet
- ElectrocardiogramDocument11 pagesElectrocardiogramAbby BhevNo ratings yet
- EKG Interpretation: DR K P Tripathy Kims, BhubaneswarDocument58 pagesEKG Interpretation: DR K P Tripathy Kims, BhubaneswarAbhilash MohantyNo ratings yet
- Kamis 10 September 2015 - IPD 2 - Kuliah-Ekg-Blok-KegawatdaruratanDocument118 pagesKamis 10 September 2015 - IPD 2 - Kuliah-Ekg-Blok-KegawatdaruratanIrfanArifZulfikarNo ratings yet
- Basic EKGDocument76 pagesBasic EKGradiologoa1aprilNo ratings yet
- ECG Brief NotesDocument5 pagesECG Brief NotesKalpani Malsha UdawelagedaraNo ratings yet
- ECG at A GlanceDocument53 pagesECG at A Glancenurliah armandNo ratings yet
- EKG Interpretation 1Document56 pagesEKG Interpretation 1usmleusmle86No ratings yet
- EKG Interpretation: UNC Emergency Medicine Medical Student Lecture SeriesDocument58 pagesEKG Interpretation: UNC Emergency Medicine Medical Student Lecture SeriesanisaNo ratings yet
- EKG InterpretationDocument58 pagesEKG InterpretationHasnahdurrNo ratings yet
- ECGforinternsDocument25 pagesECGforinternsusmleusmle86No ratings yet
- EKG InterpretationDocument58 pagesEKG InterpretationIman Sama-aliNo ratings yet
- KULIAH ECG Dinkes PurworejoDocument69 pagesKULIAH ECG Dinkes PurworejoVella NurfatimahNo ratings yet
- EcgDocument6 pagesEcgMohamed IbrahimNo ratings yet
- Artigo 3Document59 pagesArtigo 3AnaLuísaGomesNo ratings yet
- Theophylline Use in Apnoea of Prematurity: Alison KerrDocument27 pagesTheophylline Use in Apnoea of Prematurity: Alison KerrBhawna PandhuNo ratings yet
- Pulmonary Hypertension Associated With Bronchopulmonary Dysplasia A ReviewDocument9 pagesPulmonary Hypertension Associated With Bronchopulmonary Dysplasia A ReviewEduardo Rios DuboisNo ratings yet
- COURAGE TrialDocument39 pagesCOURAGE TrialRirin ChandrikaNo ratings yet
- Cardiac Physiology Dissertation IdeasDocument6 pagesCardiac Physiology Dissertation IdeasBuyAPhilosophyPaperUK100% (2)
- Emergency Medicine Practice: Managing Postpartum Complications in The Emergency DepartmentDocument24 pagesEmergency Medicine Practice: Managing Postpartum Complications in The Emergency DepartmentM'hamedNo ratings yet
- COPD Practice QuestionsDocument8 pagesCOPD Practice QuestionsMikaella CondeNo ratings yet
- Stable Angina PectorisDocument11 pagesStable Angina Pectorismarco_bawNo ratings yet
- Pathophysiology Practice Questions With Answers: A. B. C. D. EDocument93 pagesPathophysiology Practice Questions With Answers: A. B. C. D. EVikash KushwahaNo ratings yet
- 38.17 Cardiac Pacing: Basic Concepts: Renato Pietro RicciDocument16 pages38.17 Cardiac Pacing: Basic Concepts: Renato Pietro RicciurtikikeNo ratings yet
- Heart Failure Care PlanDocument5 pagesHeart Failure Care PlanJustin StuartNo ratings yet
- Enzyme TestsDocument12 pagesEnzyme TestsgireeshsachinNo ratings yet
- Project #7 - HypertensionDocument2 pagesProject #7 - HypertensionKPNo ratings yet
- L12.1-OB-Intrapartum Assessment (Nov1221)Document9 pagesL12.1-OB-Intrapartum Assessment (Nov1221)Erald PaderangaNo ratings yet
- Haemat Pracs NotesDocument10 pagesHaemat Pracs Notesaaron mbindyoNo ratings yet
- Circulatory System TurtleDocument32 pagesCirculatory System TurtleVillamorchardNo ratings yet
- Conduction SystemDocument2 pagesConduction SystemMalik Asif HussainNo ratings yet
- Download pdf Pocket Guide To Diagnostic Hematopathology S David Hudnall ebook full chapterDocument53 pagesDownload pdf Pocket Guide To Diagnostic Hematopathology S David Hudnall ebook full chapterkim.baker981No ratings yet
- Lipitor: (Atorvastatin Calcium) TabletsDocument29 pagesLipitor: (Atorvastatin Calcium) TabletsEvelinaĐulbićNo ratings yet
- Gastro MCQsDocument14 pagesGastro MCQsvaegmundigNo ratings yet
- Introduction To Human Body Systems and Related Medical Terminology - Part 1 PDFDocument207 pagesIntroduction To Human Body Systems and Related Medical Terminology - Part 1 PDFKranthi Kumar KranthiNo ratings yet
- Manlak Daftar KodeDocument139 pagesManlak Daftar KodeZainal SaragihNo ratings yet